
Abstract
Background:
Many patients with decubitus-related osteomyelitis are ineligible for myocutaneous flapping, and optimal management in this population is unknown. We describe treatments and outcomes of hospitalized patients with decubitus ulcer-related osteomyelitis who did not undergo surgical reconstruction or coverage.
Methods:
We systematically identified hospitalized patients with diagnoses of pelvic, sacral, or femoral osteomyelitis due to decubitus ulceration between 1 January 2018 and 31 December 2018. Demographics, comorbidities, laboratory data, and outcomes were collected by manual chart review. T-tests or Chi-square tests were used for descriptive statistical comparisons; logistic regressions were used to explore the odds of readmission, osteomyelitis-related readmission, and death.
Results:
Of 89 patients meeting inclusion criteria, 34 (38%) received surgical debridement and ⩾6 weeks of antibiotics; 55 (62%) received either antibiotics alone or debridement and <6 weeks of antibiotics. Mean age was 55 (standard deviation 18) years, 55% of patients were male, and 69% had spinal cord injury or other form of paralysis. Within 1 year, 56 (63%) patients were readmitted, 38 (44%) patients were readmitted due to complications from osteomyelitis, and 15 (17%) died. We found no significant differences in readmission (OR = 1.33, 95% CI: 0.54–3.21, p = 0.53), readmission related to osteomyelitis (OR = 1.64, 95% CI: 0.69–4.04, p = 0.27), subsequent sepsis (OR = 2.27, 95% CI: 0.83–6.93, p = 0.13), or death (OR = 2.88, 95% CI: 0.83–13.4, p = 0.12) by treatment group.
Conclusions:
Among patients with decubitus-related osteomyelitis who did not undergo myocutaneous flapping, outcomes were generally poor regardless of treatment, and not significantly improved with prolonged antibiotics. Prospective studies are needed to assess best practice strategies for this challenging patient population.
Background
Pressure injuries and decubitus ulcers are a frequently encountered comorbidity in hospitalized patients and a common reason for hospitalization. 1 Globally, prevalence estimates for pressure injuries among hospitalized patients is as high as 12.8%. 2 In high risk populations such as those with spinal cord injuries, the prevalence of decubitus ulcers can reach as high as 30%.3,4 The estimated incidence of decubitus ulcers is as high as 23% in patients receiving long-term care and as high as 17% in those receiving home care. 1 Management of pressure ulcers is costly both in terms of healthcare dollars and emotional burden to patients, families, and healthcare providers.5,6 For individual patients, the average cost associated with a pressure ulcer can exceed $100,000, and for healthcare systems, the costs of managing pressure ulcers is billions of dollars annually.4,7
The infection of decubitus ulcers and subsequent complications of acute or chronic osteomyelitis pose additional costs and challenges. While incidence of infection of existing pressure injuries is difficult to estimate, prior studies suggest that 6% of all nursing home residents will require treatment for infected pressure ulcers at any given point.8,9 The presence of exposed bone, once thought to indicate high likelihood of osteomyelitis, has been found to be a poor predictor of infection. 10 Magnetic resonance imaging has good sensitivity, up to 98% in some studies, but may not be possible in all patients, is limited in terms of specificity, and is unable to differentiate acute from chronic osteomyelitis, thus influencing treatment course.10,11 Therefore microbiologic and histopathologic analyses of bone biopsies are the standard for diagnosis, with microbiologic data showing that infections are frequently polymicrobial with Staphylococcus aureus, coagulase negative Staphylococci, Streptococcal species, and Enterobacteriaceae predominating.7,10,12,13
While there are a number of strategies for preventing the formation of pressure injuries, consistent guidelines on management of existing ulcers with underlying osteomyelitis are lacking.1,10 Multiple studies have shown success with a multidisciplinary approach involving bone biopsy, directed antibiotics toward isolated organisms, optimized nutrition, pressure off-loading, fecal diversion, and surgical coverage with myocutaneous flaps.10,12 This combined treatment modality has been shown to improve successful healing and also decrease rates of readmission when compared to antibiotics alone. 7 In the absence of surgical wound coverage, antibiotic use and duration appear to have no bearing on rate of recurrent osteomyelitis.10,14 However, there are often significant social and medical barriers that prevent patients from undergoing the combined treatment of decubitus wounds complicated by osteomyelitis, and the utility of alternative strategies such as antibiotics and debridement alone in preventing readmission and recurrent infection in this population is an unknown but often utilized strategy. Our goal was to describe treatments and outcomes of hospitalized patients with decubitus ulcer-related osteomyelitis who did not undergo surgical reconstruction or coverage, and the impact of tiered strategies: (1) debridement and at least 6 weeks of antibiotics versus (2) any other treatment (debridement alone, antibiotics alone, debridement with shorter antibiotic courses, etc.) on outcomes of death or readmission.
Methods
We identified patients hospitalized within the University of Colorado Health (UCHealth) system who had a diagnosis of pelvic, sacral, or femoral osteomyelitis due to decubitus ulceration between 1 January 2018 and 31 December 2018. The electronic medical record was systematically searched by International Classification of Disease-10 codes relating to sacral decubitus ulceration and osteomyelitis (Supplemental Information 1). Patients were included if they were at least 18 years of age, had a diagnosis of osteomyelitis identified by computed tomography or magnetic resonance imaging, pathologic examination, or positive bone culture with accompanying diagnosis in the electronic medical record, as defined by physician documentation. All patients additionally must have had the presence of an overlying stage 4 decubitus ulceration. Patients were excluded if osteomyelitis was unrelated to a decubitus ulcer, if they had inadequate duration of follow-up, defined as no documentation in the medical record at 1 year from initial admission (unless primary outcome occurred prior to 1 year), death during initial admission, or discharge to hospice after initial admission. Charts were manually reviewed for inclusion or exclusion. After initial review, a second reviewer surveyed a subset of eligible and ineligible patients to assess for agreement.
Demographic and limited clinic data were abstracted and stored on a secure REDCap database (Research Electronic Data Capture secure database). The study was reviewed and approved by the Colorado Multiple Institution Review Board (IRB #29-3943).
Patients were categorized as having received (1) debridement, directed antibiotics, and myocutaneous flapping, (2) debridement plus extended antibiotics (6 or more weeks), or (3) non-optimal (all other combinations) therapy. Antibiotic initiation, regimen, and duration were at the discretion of the treating provider. In the case that patients died during the 6 weeks from the index admission, they were classified by intended antibiotic course. As the goal was to compare outcomes among those who did not undergo myocutaneous flapping and small sample sizes, the comparative analyses were restricted to groups 2 and 3.
The primary outcomes included hospital readmission related to osteomyelitis or readmission for any cause within 1 year. Secondary outcomes of interest were mortality due to any cause and subsequent sepsis as a consequence of decubitus ulcer. Additional characteristics included self-reported race and ethnicity, categorized as Hispanic (regardless of race), non-Hispanic Black, non-Hispanic White, Other (all other combinations, including did not answer), age, comorbidities including diabetes mellitus, prior amputation, prior decubitus ulcer or osteomyelitis, stroke, dementia, cognitive impairment, neurodegenerative disease, spinal cord injury or other paralysis, immunocompromising conditions, and malignancy, laboratory values including maximum C-reactive protein (CRP) during admission, lowest albumin during admission, and maximum white blood cell concentration during admission.
Statistical analysis
Statistical comparisons were performed for a subset of variables chosen a priori using t-tests for continuous variables [body mass index (BMI), age at admission, laboratory values] or Chi-square tests for categorical variables (ethnic/racial minority, sex, diabetes, spinal cord injury, prior sacral osteomyelitis, prior decubitus ulcer, dementia, antibiotic use, imaging performed, and consultations performed); an equivalent exact test was used to evaluate dementia due to low prevalence. Lab values that fell below the detectable threshold were recorded as half the minimum detectable value (N values changed = 1). CRP and white blood cell count (WBC) values were log transformed due to distributional skew. Univariable logistic regressions were used to explore the odds of readmission, osteomyelitis-related readmission, and death comparing the debridement plus at least 6-week of antibiotics group (Table 3) to the non-optimal group.
Results
Among 903 patients with relevant ICD-10 codes who were admitted during the time-period of interest, 89 met criteria for inclusion (Figure 1). Eight hundred three patients were excluded from the analysis: 561 had no diagnosis of osteomyelitis, 135 had osteomyelitis that was unrelated to decubitus ulcer, 50 had inadequate duration of follow-up, 56 had multiple reasons for exclusion, and one patient had no information in their medical record number. Eleven patients underwent debridement, direct antibiotic therapy, and myocutaneous flapping and are described further here, but not included in the 89 for the primary analysis. The decision to offer flap was at the discretion of the plastic surgeons who at our institution have strict criteria that must be met before a patient is considered for flap closure. Of the 89 patients, 34 (38%) received six or more weeks of antibiotics and underwent surgical debridement, and 55 (62%) received either antibiotics alone or debridement with less than 6-weeks of antibiotic therapy.
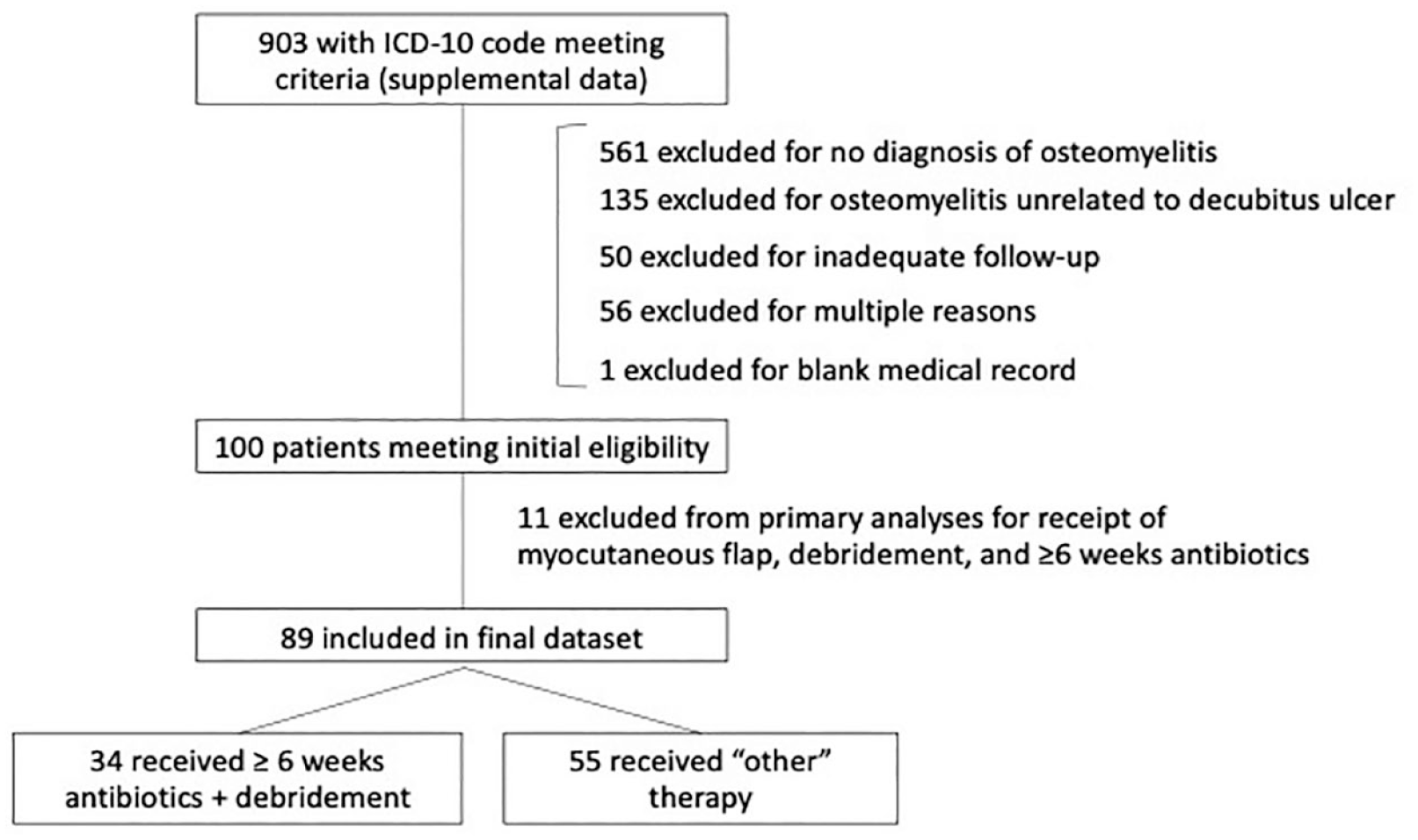
Patients who were screened, excluded, and included.
Thirty patients, 15 of whom were included for analysis and 15 of whom were excluded, were randomly selected and assessed by a second reviewer for agreement for inclusion. Reviewers agreed on 28 of 30 (93%) of cases, with consensus on remaining two cases being reached after conference.
The mean age at initial admission was 54.8 (standard deviation 18.2) years, 55% of patients were male, and 70% non-Hispanic White. A majority of patients were admitted to the hospital from home or independent living (73%). Sixty-one patients had spinal cord injury or other form of paralysis (69%), with 54% having paraplegia and 15% having quadriplegia. Sixty-nine patients had diagnosis of previous decubitus ulceration and 37% had diagnosis of at least one prior episode of femoral, pelvic, or sacral osteomyelitis. Median peak CRP was 97.4 mg/L (inter-quartile range, 60.80–178.03 mg/L; normal <10 mg/L), and median peak WBC count during the index hospitalization was 12.60 × 109/L (inter-quartile range, 9.38–16.20 × 109/L; normal range 4.5–11.0 × 109/L). Cross-sectional imaging was performed in 89% of patients with 38% of patients undergoing computerized tomography scan, 40% of patients undergoing magnetic resonance imaging, and 10% of patients undergoing both. 39% of patients had pathologic examination of tissue.
The two treatment groups (either receiving debridement plus ⩾6 weeks of antibiotics or receiving other therapy) were similar in terms of age, sex, race/ethnicity and laboratory values (albumin, WBC, and CRP). The group receiving debridement plus ⩾6 weeks of antibiotics had a significantly higher mean BMI (29.5 versus 25.3 kg/m2, p = 0.03) and significantly fewer prior diagnoses of decubitus ulcer-related osteomyelitis (27% versus 42%, p = 0.006) (Table 1). The group receiving debridement plus ⩾6 weeks of antibiotics was also more likely to have had an infectious disease consultation, 97% versus 69% (p = 0.003) but had similar rates of wound care (100% versus 96%, p = 0.60) and physical medicine and rehabilitation (24% versus 18%, p = 0.74) consultations.
Patient characteristics at hospital admission.

HIV, bone marrow or solid organ transplant, autoimmune connective tissue disease.
CRP, C-reactive protein; SD, standard deviation; WBC, white blood cell.
Patients who underwent debridement plus ⩾6 weeks of antibiotics received a median 44.5 (inter-quartile range, 43.3–101.8) days of antibiotic therapy. In the other group, 18% of the patients underwent debridement, and the median duration of antibiotic therapy was 29.0 (inter-quartile range, 10.0–57.5) days (Table 2).
Diagnostics and interventions by treatment group.

Overall, 56 patients (63%) were readmitted within 1 year for any reason, 38 (43%) were readmitted due to complications from osteomyelitis, 24 (43%) were readmitted with sepsis, and 15 (17%) died; details by treatment group are detailed in Table 3. When comparing outcomes between the two groups, we found no difference in our primary outcome of readmission for any reason between patients receiving debridement plus ⩾6 weeks of antibiotics and patients receiving other therapy (OR = 1.33, 95% CI: 0.54–3.21, p = 0.53). We similarly found no differences in readmission related to osteomyelitis (OR = 1.64, 95% CI: 0.69–4.04, p = 0.27), or sepsis at readmission (OR = 2.27, 95% CI: 0.83–6.93, p = 0.13). Those in the “other” group had a trend toward greater mortality, though numbers in both groups were small (3 deaths with debridement and ⩾6 weeks of antibiotics, 12 deaths with debridement and <6 weeks of antibiotics or antibiotics alone) and did not reach statistical significance (OR = 2.88, 95% CI: 0.83–13.4, p = 0.12).
Outcomes by treatment group, including those receiving myocutaneous flapping.*

Excluded from main analyses.
For comparison, we also explored outcomes for the 11 patients who underwent myocutaneous flapping: 9 (82%) were readmitted for any reason, 4 (36%) had readmission related to osteomyelitis, 5 (56%) were readmitted with sepsis, and 1 died (9%) within 1 year (Table 3).
Discussion
In this review of patients with decubitus ulcer-related osteomyelitis, we found high rates of hospital readmission from any cause, readmission related to decubitus ulcers, and mortality in all groups. In comparing patients receiving debridement and extended antibiotics and those receiving other therapy, we did not find significant differences in outcomes, including readmission for any reason, readmission related to osteomyelitis, or sepsis at readmission. A trend toward decreased mortality with debridement and longer antibiotics failed to reach statistical significance, however the trend suggests that there may be benefit to more intensive therapy in some populations. Notably, even those who did undergo myocutaneous flapping had a high rate of poor outcomes over the subsequent year, emphasizing the detrimental impact of decubitus ulcers.
High-quality prospective, randomized, and controlled evidence on best-practices for treatment of existing complicated decubitus ulcers and osteomyelitis are lacking, and recommendations are largely based upon retrospective data and expert opinion.1,15,16 Although guidelines suggest that multidisciplinary management with radiographic evaluation, combination of debridement of necrotic tissue and myocutaneous flap coverage, rehabilitation, optimized nutrition, and systemic antimicrobial therapy is ideal, in reality, there is wide variability in the availability and implementation of these practices both within and between institutions.7,10,11,17–19 Even when myocutaneous flapping is performed, flaps have high rates of complications and require high levels of participant engagement with nutritional, nursing, and logistical support to facilitate long periods of pressure offloading and fastidious wound care.20–22 Given these high rates of complication and failure, patients at high risk for adverse outcomes are often not considered candidates for myocutaneous flapping in some hospitals, and clinicians are left navigating the best of several sub-optimal options when treating patients deemed to be poor surgical candidates. 20 Our study is unique in that we purposefully examined the clinical characteristics and outcomes of patients receiving what is often considered sub-optimal therapy, which, given the discordance between ulcer incidence and rates of flapping, likely reflect the majority of patients living with decubitus ulcer-related osteomyelitis. 22
In our population of patients not undergoing myocutaneous flapping, we discovered a lack of consistency in the approach to both workup and management. While 89% of the patients in our study received cross-sectional imaging, the modality utilized was divided evenly between computed tomography and magnetic resonance imaging. Additionally, while 49% of patients underwent bone biopsy or debridement, only 37% of all patients had samples evaluated by pathology for the presence of osteomyelitis. This inconsistency in diagnostic workup can lead to clinical uncertainty, and subsequent risk that patients receive antibiotics not tailored to the underlying diagnosis. As antibiotic exposure is a well-known risk factor for both development of Clostridiodes difficile infection and acquisition of antibiotic resistant Enterobacteriaceae, overly broad or unnecessarily long durations of antibiotics can increase risks of long-term adverse outcomes.23–25
Despite the consensus that multidisciplinary care facilitates improved outcomes, we found that few patients in our study received comprehensive evaluation and consultation: only 14 (16%) patients received full non-surgical consultation including infectious disease, wound care, and physical medicine and rehabilitation services. Multidisciplinary teams do exist for the management of pressure ulcers and related osteomyelitis; however, they operate primarily in the outpatient setting and require patients to be medically stable enough to undergo diagnostic and therapeutic procedures and have access to resources to be able to engage in outpatient care. Systematic approaches to diagnosis and both short- and long-term management are needed at the initial point of contact in the inpatient care setting.
Patients with decubitus ulcers and osteomyelitis present a challenge for retrospective study, and our study had several limitations largely related to its retrospective design. While there were no statistically significant differences in outcome between the two groups, there was a trend toward higher mortality seen in the “other” group which may reflect more severe baseline illness in this group. The populations examined in this study did not undergo myocutaneous flapping, and the underlying medical and psychosocial reasons for lack of flapping eligibility are possible confounding variables. Another limitation is the uncertainty regarding the chronicity of infection. Acute and chronic osteomyelitis are often treated differently (debridement with antibiotics versus antibiotics alone); however, we found that definitive pathologic diagnosis in our population was often lacking or ambiguous, leading providers to make a clinical determination about the chronicity of underlying osteomyelitis based on clinical presentation and the presence of an ulcer, which likely influenced both treatment duration and outcomes. 11
Conclusion
In this retrospective cohort study, we found that patients with decubitus ulcer-related osteomyelitis who did not undergo myocutaneous flapping are at high risk for adverse outcomes irrespective of debridement or duration of antibiotic therapy with high rates of readmission, readmission related to decubitus ulcer, and mortality. We observed no difference in readmission, readmission related to osteomyelitis, sepsis at readmission, or mortality in patients with decubitus ulcer-related osteomyelitis who had ⩾6 weeks of antibiotic therapy plus debridement or other therapy. Patients with decubitus ulcer-related osteomyelitis can be challenging to manage given the multifactorial drivers underlying this disease, and there are many reasons why patients may be ineligible for the gold-standard treatment of debridement, antibiotics, and myocutaneous flapping. There is likely a role for a systematic approach to diagnosis, staging, and management in the inpatient setting, with extensive social, nursing, and therapy support needed during the transition into the outpatient care setting. In many patients, a palliative approach may be most appropriate. Prospective studies are needed to assess best practice strategies for management of patients with decubitus ulcers and osteomyelitis.
Supplemental Material
sj-docx-1-tai-10.1177_20499361231196664 – Supplemental material for Retrospective analysis of the management of pelvic decubitus ulcers and their outcomes
Supplemental material, sj-docx-1-tai-10.1177_20499361231196664 for Retrospective analysis of the management of pelvic decubitus ulcers and their outcomes by Laura Damioli, Zachary Shepard, Melissa P. Wilson and Kristine M. Erlandson in Therapeutic Advances in Infectious Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.