
Abstract
Background:
Outpatient parenteral antimicrobial therapy (OPAT), when required, is beneficial to patients and healthcare systems by reducing hospital length-of-stay, providing cost savings, and improving patient satisfaction.
Objectives:
The purpose of this study is to determine readmission rates and associated risk factors in patients receiving OPAT at home.
Methods:
This retrospective study included hospitalized patients 15 years and older who were discharged on intravenous antimicrobial therapy via OPAT at home between January 2018 and December 2019. Patients receiving antimicrobials at a skilled nursing facility, long-term acute care, or dialysis center, and those who began OPAT at home directly from the outpatient setting were excluded. The primary outcome of this study was all-cause 30-day readmission rate. Secondary outcomes included 90-day readmission rate, rates of complications related to OPAT, emergency department visits during OPAT, and predictors of all-cause 30-day readmission through a logistic regression analysis.
Results:
Two hundred individual patients were included in the analysis; 60% were male and the mean age was 49 years. The most common indications for OPAT at home were bone and joint infection (52%) and bacteremia (26%). Forty patients (20%) experienced an unplanned, all-cause 30-day readmission, with a total of 48 readmission events. Of the 40 patients who were readmitted within 30 days, 20 (50%) were due to non-OPAT related reasons. Sixty patients (30%) experienced an OPAT-related complication, and chronic kidney disease was found to be an independent predictor of readmission (OR: 2.8, 95% CI: 1.0–7.6).
Conclusions:
Patients receiving OPAT at home are at increased risk for early hospital readmission, but it is often due to reasons not associated with OPAT. Patients with chronic kidney disease beginning OPAT at home should be closely monitored after discharge.
Background
Outpatient parenteral antimicrobial therapy (OPAT) has existed since the 1970s, and is utilized by patients who need continued treatment with intravenous (IV) antimicrobial therapy after acute-care hospital discharge. OPAT has been shown to reduce hospital length-of-stay, providing potential financial benefit and improving patient satisfaction. 1 Despite its benefits, OPAT carries risks inherent to the intervention but also due to decreased supervision and monitoring, which include adverse drug reactions (ADRs), vascular access device (VAD) complications, and hospital readmission.2,3
With the growing availability of OPAT services, it is critical to assess the rates of complications and hospital readmissions. Previous literature has shown 30-day hospital readmission rates between 10% and 30%.4–8 Currently, there is no well-defined assessment tool to assess patients’ risk for readmission or complications related to OPAT. However, various risk factors for readmission have been identified, including hospital admission within the previous 12 months, treatment of bacteremia, history of drug-resistant organisms, lack of a primary care provider, and discharge to a skilled nursing facility.8–11 In this study, we aimed to determine 30-day readmission rates and which factors influence the risk of readmission using OPAT data from a large academic medical center in the southern United States.
Methods
The Outpatient Antimicrobial Service (OAS) at the University of Mississippi Medical Center (UMMC) was established in the early 2000s and consists of an infectious diseases (IDs)-trained physician, a nurse practitioner, and a nurse coordinator. Pharmacists are not directly part of the OAS team, but the institutions’ antimicrobial stewardship pharmacists and the pharmacists that work with the ID consult teams assist with discharge antibiotic decisions and with questions regarding OAS patients. OAS is tasked with managing outpatients requiring parenteral antimicrobial therapy at home for at least 7 days after hospital discharge. OAS follows criteria published in current Infectious Diseases Society of America guidelines to determine patients’ candidacy for OPAT at home. 12 Patients can be referred to OAS during their hospitalization after inpatient ID consultation and after final antimicrobial recommendations have been provided. Then, patients are assessed to determine if they are appropriate candidates for OPAT at home. OAS is responsible for coordinating home health services, infusion services, laboratory monitoring, and outpatient follow-up. OAS is not involved with OPAT administered at rehabilitation facilities, skilled nursing facilities, or dialysis centers. After discharge, patients under OPAT at home are seen for follow-up in either the outpatient ID clinic or the OAS clinic, typically via in-person visits. The decision on the location for and time-frame to follow-up is left to the ID consultant’s discretion. OAS conducts formal once-weekly rounds where each individual patient receiving OPAT at home is discussed in a multidisciplinary fashion, laboratory results are reviewed, and decisions are made in coordination with ID consultants. Additionally, critical lab results are responded to 24 h a day, 7 days a week by OAS during office hours and after hours by the ID consultant on call.
In this single-center, retrospective cohort study, patients who were hospitalized and discharged from UMMC to receive OPAT at home were evaluated for unplanned, all-cause, 30-day readmission rates. Patients with an index hospitalization discharge between January 2018 and December 2019 were identified through OAS records. Institutional Review Board (IRB) approval was obtained from the UMMC IRB and informed consent was waived.
Inclusion criteria
All patients had met OPAT at home appropriateness criteria which included the following: an inpatient ID consult during index admission, discharge to a safe environment at home with water, electricity, refrigerator, and available caregiver, and a planned course of parenteral antimicrobial therapy greater than 7 days after discharge. A consecutive sample of patients were subsequently included in this study based on the following criteria: 15 years of age and older, discharged from UMMC and accepted by OAS while inpatient, and received IV antimicrobial therapy through a peripherally inserted central catheter (PICC) or midline.
Exclusion criteria
The following patients were excluded from the analysis: diagnosis of cystic fibrosis, patients accepted by OAS from the outpatient setting, OPAT delivery at a dialysis center, infusion center, or skilled nursing facility. Patients were not excluded based on type of infection, microorganism, socioeconomic status or immune status.
Data sources and data collection
Patients were identified through OAS historical records which included a list of patients accepted for management of OPAT at home during the study period. To ensure minimum risk to patient confidentiality, study data were collected and managed using REDCap (Research Electronic Data Capture) hosted at UMMC. 13 Each patient was assigned a random coded number, and a de-identified patient list was generated.
The data collected included pertinent patient demographics, comorbidities, OPAT indication, microbiology, inpatient and outpatient antimicrobial regimen, type of vascular access, ADRs, readmissions, and reason for readmission. Patients were categorized as having a primary bacteremia if blood cultures were positive but no source was identified. Immunocompromised was defined as bone marrow transplant, solid organ transplant, hematologic transplant, hematologic malignancy, solid organ malignancy, or human immunodeficiency virus (HIV) infection with a CD4 <200. A Charlson Comorbidity Index (CCI) score was calculated for each patient which estimates the risk of death from comorbid disease. Patients were determined to have a drug-resistant organism if one of the following organisms was identified via culture: methicillin-resistant Staphylococcus aureus (MRSA), vancomycin-resistant Enterococcus, extended-spectrum beta-lactamase-producing Enterobacterales, or carbapenem-resistant Enterobacterales. Unplanned 30-day readmission was defined as a hospital readmission within 30 days of discharge from the index hospitalization that was not planned ahead of time for a specific reason.
Outcome measures
The primary outcome of this study was the frequency of unplanned, all-cause 30-day hospital readmission. Secondary outcomes included all-cause 90-day readmission rate, frequency of complications related to OPAT, emergency department (ED) visits, and an evaluation of patient-specific factors that contributed to an increased risk of all-cause 30-day readmission.
Statistical analysis
Descriptive statistics (frequencies and percentages) were utilized to report demographic and clinical characteristics. Clinical and demographic characteristics were compared between readmitted and non-readmitted patients using the Student t, Wilcoxon rank-sum, Pearson X2, and Fisher exact tests, as appropriate. Logistic regression was used to assess the independent effects of the risk factors on odds of 30-day readmission. Factors were included based on univariate p-values and authors’ discretion. A p-value of less than 0.05 was utilized to determine significance for the logistic regression models. Data were analyzed using SPSS version 26 (IBM SPSS Statistics, Armonk, NY, USA).
Results
Two hundred thirty-six patients discharged through OAS were screened for eligibility. Of these, 36 patients were excluded, and a total of 200 patients were included in the analysis (Figure 1). A summary of patient demographics as well as index hospitalization information is presented in Table 1. The mean age was 49 years, and 120 (60%) were male. The majority of patients had public insurance [109 (54.5%)] through Medicare or Medicaid, and 153 (76%) patients had an assigned primary care provider. Prior to the index hospitalization, 104 (52%) patients had at least one previous hospitalization within the previous 12 months. Twenty-two (11%) patients had a documented infection with a drug-resistant organism within the previous 12 months, with MRSA being the most common. Twenty-nine (14.5%) patients were admitted to the intensive care unit (ICU) during the index hospitalization (Tables 2 and 3).

Study enrollment.
Demographics and clinical characteristics of patients receiving OPAT.
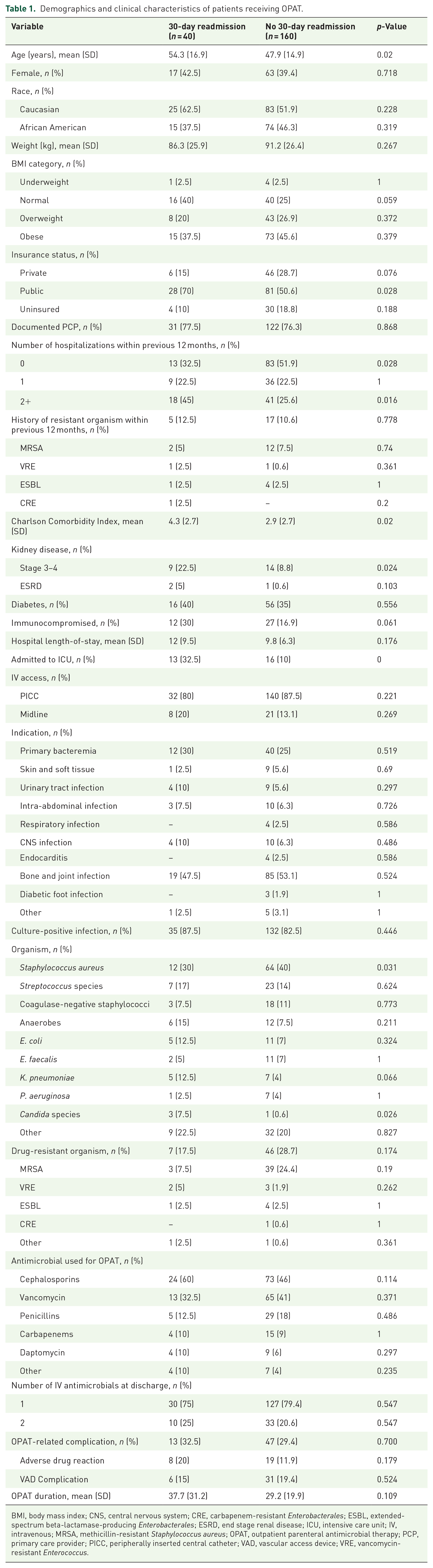
BMI, body mass index; CNS, central nervous system; CRE, carbapenem-resistant Enterobacterales; ESBL, extended-spectrum beta-lactamase-producing Enterobacterales; ESRD, end stage renal disease; ICU, intensive care unit; IV, intravenous; MRSA, methicillin-resistant Staphylococcus aureus; OPAT, outpatient parenteral antimicrobial therapy; PCP, primary care provider; PICC, peripherally inserted central catheter; VAD, vascular access device; VRE, vancomycin-resistant Enterococcus.
Clinical outcomes.

ADR, adverse drug reaction; ED, emergency department; OPAT, outpatient parenteral antimicrobial therapy; PICC, peripherally-inserted central catheter; VAD, vascular access device.
Patients could have more than one documented complication.
Patients could have more than one ED visit during OPAT therapy.
Patients could have more than one 90-day readmission.
Logistic regression model assessing risk factors influencing 30-day readmission.

OPAT, outpatient parenteral antimicrobial therapy.
The most common indication for OPAT therapy was bone and joint infection (52%) followed by primary bacteremia (26%). The majority of patients [167 (83.5%)] had positive cultures during the index hospitalization, and 53 (26.5%) had an infection with a drug-resistant organism. Of those who had a positive culture, the most common microorganisms were Staphylococcus aureus [76 (32%)], Streptococcus species [30 (13%)], and coagulase-negative staphylococci [21 (9%)] as shown in Table 1. The most common antimicrobials utilized included cephalosporins, vancomycin, and penicillins.
Of the 200 patients included in the analysis, 40 (20%) patients were readmitted within 30 days of hospital discharge. Seven of these 40 patients had multiple readmissions during this time period. Non-OPAT related reasons [20 (50%)] were the most common reason for readmission. The most common OPAT-related reasons for readmission were need for incision and drainage [8 (20%)], worsening infection [5 (12.5%)], and new infection [5 (12.5%)]. The readmitted group was older in comparison to the non-readmitted group (54.3 years versus 47.9 years, p = 0.035), more likely to have public insurance (70% versus 50.6%, p = 0.028), and more likely to have two or more hospitalizations in the 12 months prior to index hospitalization (45% versus 25.6%, p = 0.016). The readmitted group also had a higher mean CCI score (4.3 versus 2.9, p = 0.02), were more likely to have a history of stage 3–4 chronic kidney disease (CKD) (22.5% versus 8.8%, p = 0.024), as well as a higher incidence of ICU admissions during the index hospitalization (32.5% versus 10%, p < 0.001).
Sixty patients (30%) experienced a total of 66 OPAT-related complication events during antimicrobial therapy. VAD complications were the most common type of complication [37 (56%)] followed by ADRs [21 (41%)]. VAD complications occurred more frequently in patients with PICC lines (33/37, 89%) compared to midlines (4/37, 11%). ADRs mostly consisted of acute kidney injury (AKI) episodes [10 (38.5%)] and allergic reactions [9 (34.6%)]. All AKI episodes occurred in patients receiving vancomycin. Forty-three patients (22%) had an ED visit during OPAT therapy, for a total of 54 visits. VAD complications were the most common reason [29 (54%)] for ED visits followed by non-OPAT related reasons [20 (37%)]. All-cause 90-day readmission rates were also assessed with 70 (35%) patients readmitted within 90 days of index hospital discharge, for a total of 106 readmission episodes. Similar to 30-day readmissions, the most common cause of 90-day readmission was non-OPAT related reasons [56 (53%)].
A multivariate regression model was utilized to determine if certain factors put patients at an increased risk of readmission, and history of CKD at discharge was found to be an independent predictor of readmission [odds ratio (OR): 2.803, 95% CI: 1.036–7.581]. Of the 15 readmissions among patients with CKD, only two were related to OPAT with one of these being attributed to a supratherapeutic vancomycin level.
Discussion
In this single-center, retrospective cohort study, we found 20% of patients receiving OPAT at home experienced unplanned, all-cause 30-day readmission. We also evaluated risk factors for all-cause readmission. A select number of previously identified risk factors for readmission (i.e. discharge to a skilled nursing facility, lack of inpatient ID consultation) were not included in our analyses due to our OPAT program acceptance criteria. We identified several factors that were associated with hospital readmission in univariate analysis: older age, two or more hospitalizations in the previous 12 months, and a higher CCI score. Our findings are consistent with previous studies in which these same factors were found to be associated with 30-day readmission.4,8,10 Additionally, we found that patients with a public insurance plan, a history of CKD, and ICU admission during the index hospitalization were more common in patients who were readmitted, which were not identified risk factors in previous studies.
Based on a multivariate analysis, CKD was identified as the only independent risk factor for readmission. However, patients with CKD generally are at higher risk of readmission than patients without CKD. Based on data from the National Institutes of Diabetes and Digestive and Kidney Diseases, 21.4% of patients with CKD had a 30-day readmission compared with 15.7% in patients without CKD in 2020, matching trends from previous years. 14 In our population, only two of the readmissions in CKD patients were due to OPAT, indicating OPAT itself was not the driver of readmissions in this population.
Though our study found a similar rate of all-cause readmission in OPAT patients, a notable difference is the reason for readmission.4–11 Of the 40 patients readmitted, 20 (50%) were due to non-OPAT related reasons, which is significantly higher than reported in previous studies.9,11 In one study of 782 OPAT patients at a single academic medical center, 26% of the cohort experienced an unplanned 30-day readmission. Readmissions due to non-OPAT related reasons occurred in 30% of patients. 9 Similarly, Huang et al. 11 found a 21% rate of 30-day readmissions in OPAT patients with 12 (29%) being not related to infection or line complications. This may be due to differences in baseline characteristics of our population compared with previous studies. For example, in contrast to the two studies mentioned, our patients who were readmitted had a higher CCI score, which may have contributed to the non-OPAT related readmissions.
Though a large number of readmissions in this study were due to non-OPAT related reasons, identifying strategies to decrease readmissions and limit complications in the remaining patients is critical. For example, more than half of the complications related to OPAT therapy were related to VADs. Although the majority of these did not lead to a hospital readmission, they did result in many ED visits. In addition, most of the ADRs were AKIs due to vancomycin, which remains a common antibiotic used at discharge. The findings of recent studies regarding oral step-down therapy are challenging the traditional practice of prolonged parenteral antimicrobial therapy for many difficult-to-treat infections, including bacteremia, infective endocarditis, and osteomyelitis.15–18 The implementation of long-acting IV antimicrobials, such as lipoglycopeptides, could also limit the need for VAD and routine infusions at home. These options may also decrease risk of AKI by using alternatives to vancomycin. Retrospective data suggest that the effectiveness of these agents may be similar to current standard-of-care and be more cost effective.19–25
In addition, it has been suggested that early outpatient follow-up after discharge for patients with risk factors for hospital readmission could provide the opportunity to address any problems that may arise before leading to a readmission. A previous study identified that an OPAT clinic visit was associated with lower readmission compared to non-OPAT clinic visits. 26 Telehealth visits could provide benefit to patients by eliminating travel to and from clinic. In our OPAT program, telehealth has been an option for years, but during the COVID-19 pandemic its use became more widespread. Future studies should evaluate the difference in readmission rates between those with in-person OPAT clinic visits and with telehealth visits. In patients with CKD, closer follow-up with more frequent laboratory monitoring could be considered to prevent complications and readmissions. Based on the results of this study, our OAS program has recommended that patients with CKD should be seen for their first outpatient follow-up visit within 2 weeks of discharge.
There are several limitations to this study. The single-center nature of this study limits its size, and our findings are not necessarily generalizable to a broader population. Given the retrospective design, documentation of diagnoses and treatment details can suffer from missing or conflicting data. Hospital readmission, ED visits, and OPAT-related complications reported to other institutions were not able to be captured which could have resulted in a higher rate than what was found in this study. Outpatient documentation and clinical information may be more limited compared to documentation in the inpatient setting.
Conclusion
A significant proportion of patients receiving OPAT at home are readmitted within 30 days of hospital discharge, but the majority of patients in our study were due to non-OPAT related reasons. A diagnosis of CKD was found to be an independent predictor of readmission, but, similar to the overall reasons for readmission, only two of the patients with CKD were cases of readmissions due to OPAT. Further studies are needed to identify additional factors leading to readmission during OPAT as well as ways to minimize the risk.