
Abstract
Background:
Standard therapy for early syphilis involves intramuscular injections of penicillin G, which frequently faces shortages in several countries. Fourteen-day amoxicillin therapy has been suggested as an alternative to benzathine penicillin G, but the optimal duration of amoxicillin therapy remains unclear and could theoretically be shortened to less than 14 days. The aim of this study was to explore the effectiveness of short-term amoxicillin therapy for early syphilis.
Methods:
We retrospectively explored the effectiveness of short-term amoxicillin therapy for early syphilis. The treatment data of patients who had received amoxicillin therapy for less than 14 days for unintended reasons were reviewed. Diagnosis was confirmed based on either the physician’s description or clinical presentation. Successful treatment was defined as a fourfold or greater decline in the rapid plasma reagin titer or sero-reversion to negative within 12 months.
Results:
Of 295 patients, 8 received short-term amoxicillin treatment. All were men who had sex with men and people living with human immunodeficiency virus. Their median age, CD4 count, and treatment duration were 34 years (range, 26–40), 258/mL (range, 112–930), and 9.5 days (range, 5–11), respectively. One patient had primary syphilis, six had secondary syphilis, and one had early latent syphilis. All patients, except one who showed reinfection, demonstrated a serological response within 4 months. The median time for serological response was 112 days.
Conclusion:
The results indicate that early syphilis could potentially be treated with 5–11 days of amoxicillin therapy combined with probenecid. This suggests that short-term amoxicillin therapy might be a sufficient treatment for early syphilis instead of the standard 14-day course.
Keywords
Introduction
The standard treatment for early syphilis is a single intramuscular injection of benzathine penicillin G (BPG). 1 However, there has been a shortage of BPG for decades. According to a worldwide survey, 39 of 95 countries (41%) reported a BPG shortage from 2014 to 2016. 2 These global shortages are mainly due to unstable manufacturing processes, low profitability, and inaccurate forecasts of infections by respective countries. 2 Owing to the shortage of BPG, a supply challenge arises, compromising syphilis treatment and increasing the number of cases of congenital syphilis.2,3 Identifying an alternative treatment is a major challenge. Guidelines in the United Kingdom recommend the use of amoxicillin as an alternative to BPG in treating syphilis. 4 In Japan, amoxicillin has been the first choice of treatment for early syphilis for several decades because BPG was not available until January 2021, 4 although the optimal dose and duration are still under investigation. Japanese domestic guidelines recommend 1.5 g/day oral amoxicillin for a median of 4 weeks against early syphilis. 5 The overall serological cure rate with 1.5 g/day amoxicillin monotherapy for a median of 4.5 weeks against early and late syphilis is 94.9%. 6 According to previous studies, 3.0 g/day amoxicillin plus probenecid for 14 days against syphilis demonstrated a high efficacy of 94.8–97.5%. 7 Recently, our open-label randomized controlled noninferiority trial showed that 1.5 g/day amoxicillin monotherapy for 14 days and 3.0 g/day amoxicillin and probenecid combination therapy for 14 days achieved 93.5% and 97.9% cure rates against early syphilis, respectively. 8 In addition, doxycycline for 14 days can be an alternative drug for early syphilis treatment in most countries. 1 However, several guidelines suggest that a duration of 7–10 days with appropriate serum levels of penicillin may be sufficient to treat early syphilis successfully.4,9 In general, a short-term treatment has several benefits, including improved adherence, reduced costs, and possibly fewer adverse effects. To the best of our knowledge, there are no reports on short-term treatment (<14 days) for syphilis. Herein, we aimed to demonstrate that short-term 3.0 g/day oral amoxicillin plus probenecid could be an alternative treatment by reviewing the clinical results of patients with early syphilis treated with amoxicillin for less than 14 days for any reason in our human immunodeficiency virus (HIV) clinic.
Methods
Study population and treatment
We retrospectively reviewed the data of 295 patients with early syphilis treated for syphilis between 1 January 2011 and 31 August 2021, using the medical records at the AIDS Clinical Center, National Center for Global Health and Medicine, Tokyo, Japan. This study included three participants from an ongoing randomized clinical trial designed to investigate the efficacy of two regimens of amoxicillin treatment for syphilis in patients with HIV-1 infection (UMIN000033986; ethical committee approval number NCGM-G-002559-00). The exclusion criteria for this study were as follows: (i) neurosyphilis or ocular syphilis and (ii) intake of additional antibiotics before rapid plasma reagin (RPR) decline.
Diagnosis and testing
A syphilis diagnosis was primarily confirmed by a physician in charge based on serological changes: (i) positive RPR conversion or (ii) a fourfold or greater increase in RPR compared with previous values. When there was no clear description, the diagnosis was made based on the clinical presentation, such as a history of rashes or sexual activity in the medical record. Early syphilis included primary, secondary, or early latent syphilis.
After treatment, patients were followed up quarterly for the measurement of RPR titer until successful treatment was confirmed. Successful treatment was defined as a ⩾fourfold or greater decline in the RPR titer or sero-reversion to negative within 12 months. The RPR titer was evaluated using either a serial dilution method (Sanko RPR test; Sekisui Medical Co., Tokyo, Japan) until March 2020 or an automated method (Mediace; Sekisui Medical Co., Tokyo, Japan) after March 2020. The type of RPR test was not changed during the follow-up period.
Statistical analyses
We obtained descriptive statistics from the collected data. Patients’ age, CD4 count, and duration of treatment are represented as the median and range.
Results
Among the 295 patients treated for syphilis, 8 patients received amoxicillin treatment for less than 14 days for unintended reasons (Table 1). All eight patients were people living with HIV (PLWH) and men who had sex with men (MSM). The RPR titers of the eight patients were evaluated within 12 months, and no one was lost to follow-up. The median age at treatment initiation, CD4 count, and treatment duration were 34 years (range, 26–40), 258/mL (range, 112–930), and 9.5 days (range, 5–11), respectively. In terms of syphilis stage, one patient had primary syphilis, six had secondary syphilis, and one had early latent syphilis. Seven patients received 1.0 g amoxicillin and 250 mg adjunctive probenecid three times a day, while one patient received 1.5 g amoxicillin and 500 mg adjunctive probenecid twice a day. Treatment delay after the RPR titer test was a median of 6 days (range, 0–28). Seven patients discontinued their prescribed treatment with amoxicillin plus probenecid because of drug eruptions and did not receive any complementary treatment during the entire course of treatment. Amoxicillin treatment was ceased in one patient because of a missed appointment after having received the drug for 5 days.
Characteristics of patients with early syphilis treated with amoxicillin for less than 14 days.

Baseline RPR titer was measured using the automated method in patient no. 1 and the serial dilution method in patient nos. 2–7.
AMPC, amoxicillin; CD, cluster of differentiation; PB, probenecid; RPR, rapid plasma reagin.
We described the RPR titer trend of all patients, with 100% as the baseline RPR in each patient (Figure 1). Among the eight patients, seven were successfully treated for syphilis with amoxicillin within 12 months. Treatment failure was recorded in one patient (no. 8), in whom the RPR titer declined from 1:128 before treatment to 1:64 at 3 months after treatment; however, it increased to 1:128 again at 5 months after treatment, when the patient exhibited new systemic macular rashes and a history of sexual activity, which were consistent with reinfection. Furthermore, one patient (no. 7) showed an increase in RPR titer after treatment success, which was attributed to reinfection because of sexual activity. During the follow-up period, the RPR measurement method was changed in one patient (no. 2) after the confirmation of treatment success using the serial dilution method. The median time for serological response among seven cured patients was 112 days (range, 35–131) (3.7 months).
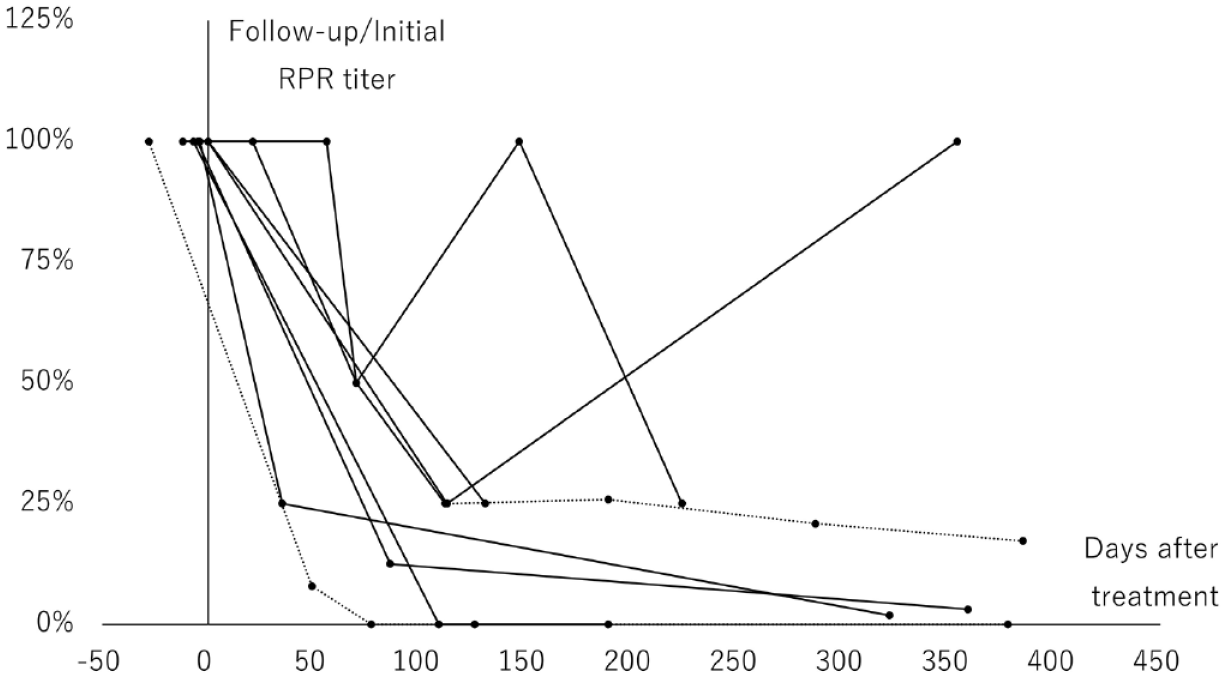
RPR trend after treatment.
Discussion
This study suggested that short-term amoxicillin treatment (5–11 days) was clinically effective when a complete 14-day treatment course had to be interrupted for some reason. The rationale for short-term treatment was based on previous reports. As Treponema pallidum, the causative agent of syphilis, cannot be cultured, it has never been possible to use conventional in vitro methods to assess antimicrobial susceptibility; therefore, its susceptibility is estimated based on microscopic motility or by using a rabbit model. 10 For the successful treatment of early syphilis, a serum penicillin level of 0.003 mg/mL is required for the immobilization of T. pallidum; for a treponemicidal effect, a serum penicillin level of 0.018 mg/mL must be maintained for 7–10 days and subtreponemicidal intervals should not exceed 30–33 h.9,10 In the case of amoxicillin, 0.07 mg/mL is required for immobilization and 0.42 mg/mL is required for a treponemicidal effect. 11 This treponemicidal level would be achieved using 3 g amoxicillin plus probenecid treatment regimens, as observed in this study, from the perspective of pharmacokinetics.11–13 Ingesting 1000 mg amoxicillin enables the maintenance of the treponemicidal blood concentration for 6–8 h, and this concentration of amoxicillin is augmented by the coadministration of probenecid.11–13
During the follow-up period, we confirmed treatment success (a ⩾fourfold decline) among seven patients. The median time of confirmation was 3.7 months after treatment. A previous 14-day amoxicillin treatment for early syphilis showed a median serological response duration of 4 months (interquartile range: 3–6). 7 Therefore, the short-term (5–11 days) amoxicillin treatment in this study appeared to be as effective as the standard (14 days) treatment. In comparison with the standard therapy, BPG injection treatment resulted in a successful serological response of 59.5% within 3 months and 81.5% within 6 months after treatment; these findings are also similar to those of our study. 14
This study has some limitations. First, this was a single-center, observational study with only eight cases without a control group. Thus, we could not conclude whether short-term treatment has sufficient efficacy. At most, the treatment efficacy was expected to be approximately 97% based on previous studies on 14-day 3.0 g amoxicillin and probenecid combination therapy.7,8 Except for the one case presumed to be of reinfection, we confirmed that the remaining seven cases were successfully treated with short-term therapy. However, we could not conclude whether short-term 3.0 g amoxicillin and probenecid combination therapy was noninferior to 14-day therapy because of the abovementioned limitation. It is also unclear whether the duration of treatment could have been reduced further; more extensive prospective investigations are needed to address these limitations. Second, owing to the small number of patients, we could not determine whether short-term treatment reduces adverse effects compared with full-course treatment. A previous study showed that 9.8% of patients receiving 14-day amoxicillin treatment had adverse effects, such as drug rashes, fever, and diarrhea. 7 Third, all patients were MSM and PLWH, and the effectiveness of the short-term treatment might not be generalized to other populations. However, the serological failure rate is higher in PLWH than in non-HIV patients. 1 Therefore, if the short-term treatment was sufficiently effective among our immunocompromised patients, the same treatment could be adapted to immunocompetent people without HIV infection, except for pregnant women. Fourth, the RPR titer could vary without treatment. A recent report suggested that 16.8% of early syphilis patients had a ⩾fourfold RPR titer change within 14 days of a delay between diagnosis and treatment. 15 In our study, six of the eight patients started treatment after a median of 6 days (range, 0–28), and thus, the RPR titer could have changed before treatment, and our results could have been overestimated or underestimated. However, most of the RPR titer would not have been affected. Nevertheless, the precise efficacy of short-term therapy needs to be evaluated in further studies.
In conclusion, this is the first study to suggest that early syphilis could be treated with 5–11 days of amoxicillin treatment without any complementary treatment during the entire course. However, our study did not clarify the adequate duration of therapy and efficacy, warranting further examination. To control the globally widespread incidence of syphilis, short-term amoxicillin treatment should be investigated as an attractive option to combat the global shortage of BPG.
Footnotes
Acknowledgements
The authors thank Takahiro Aoki, Yasuaki Yanagawa, Koji Watanabe, Haruka Uemura, Kunihisa Tsukada, and Katsuji Teruya of the AIDS Clinical Center for data collection and Takashi Nemoto, Chihiro Eguchi, and other laboratory staff of the Laboratory Department of NCGM for their support.