
Abstract
Abstract ID: 1
Novel point-of-care biosensor for group B Streptococcus testing
1Department of Chemistry, University of Bath, Bath, UK, 2Department of Life Science, University of Bath, Bath, UK

Schematic of biosensor mode of action.
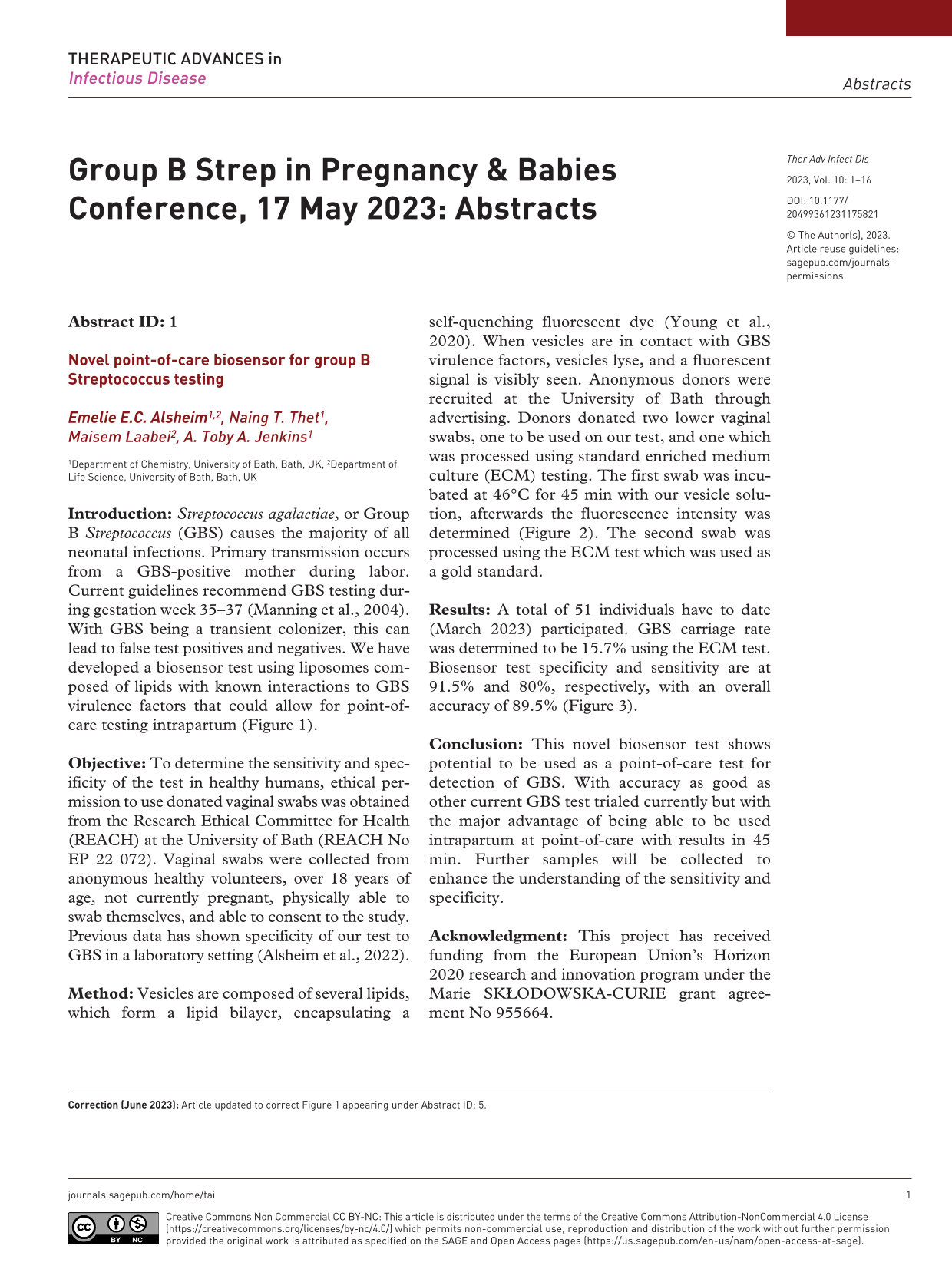
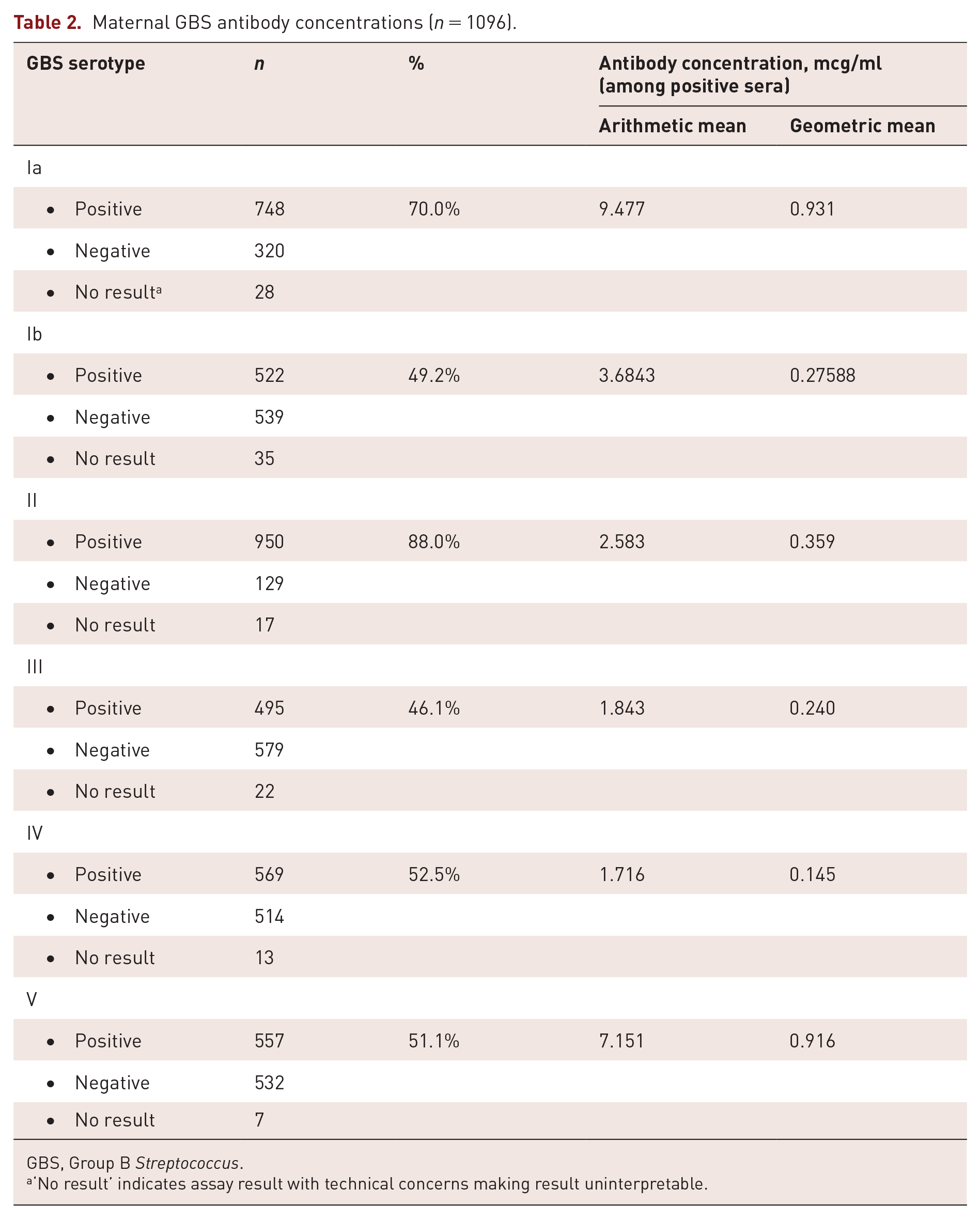
Biosensor fluorescence response for 51 participants in study.
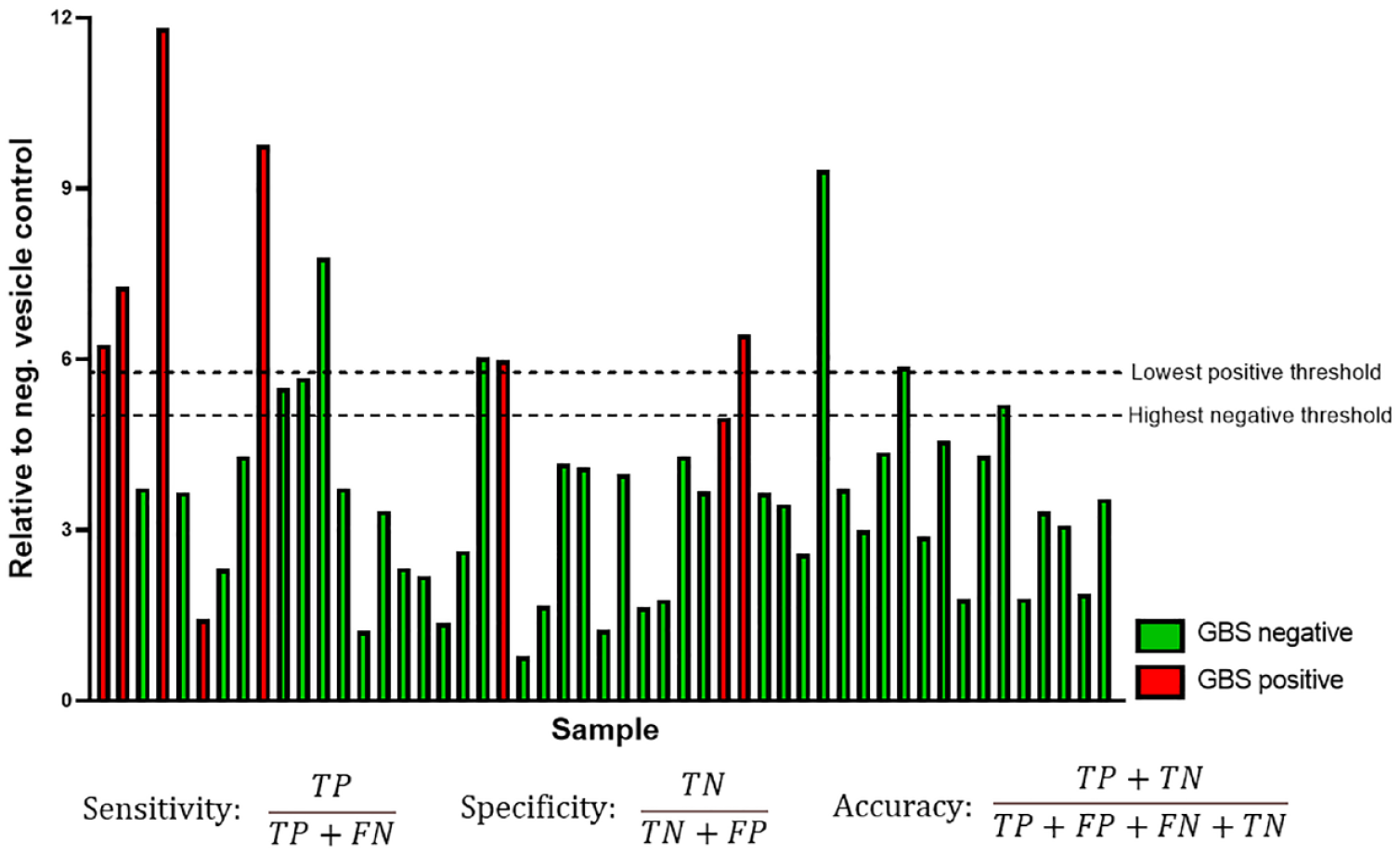
Standards for reporting of diagnostic accuracy (STARD) flow diagram.
Abstract ID: 2
Should the NHS offer universal group B Streptococcus screening to pregnant women?
1Faculty of Medicine, Imperial College London, London, UK, 2Health Protection Team, UK Health Security Agency South West, Bristol, UK, 3Department of Primary Care and Public Health, Imperial College London, London, UK
Abstract ID: 3
Population genetics of Group B Streptococcus from maternal carriage in an ethnically diverse community in London
1Parasites and Microbes Programme, Wellcome Sanger Institute, Hinxton, UK, 2Departments of Microbiology, Northwick Park Hospital, London North West University Healthcare NHS Trust, London, UK, 3Faculty of Medicine, Imperial College, London, UK, 4Cambridge Institute for Medical Research and School of Clinical Medicine, University of Cambridge, Cambridge, UK, 5World Health Organization Collaborating Centre for Diphtheria and Streptococcal Infections, UK Health Security Agency, London, UK, 6Department of Veterinary Medicine, University of Cambridge, Cambridge, UK
Abstract ID: 4
Group B Streptococcus antibodies and placental antibody transfer ratios among persons presenting for childbirth 2019–2021
1Children’s Hospital of Philadelphia, Philadelphia, PA, USA, 2Emory University School of Medicine, Atlanta, GA, USA, 3University of Texas Houston, Houston, TX, USA, 4Duke University, Durham, NC, USA, 5Centers for Disease Control and Prevention, Atlanta, GA, USA
Maternal demographic and clinical characteristics.

GBS, Group B Streptococcus.
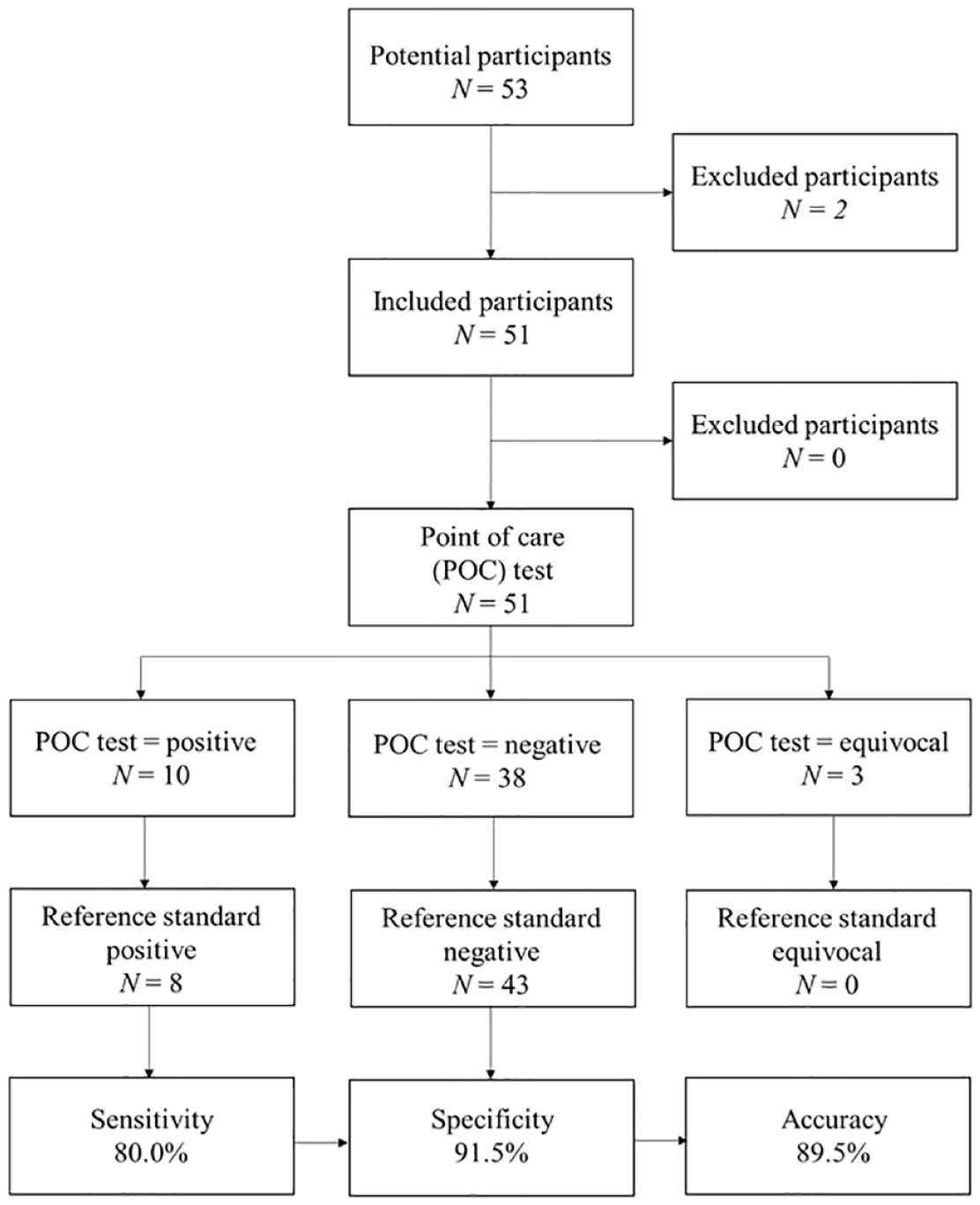
Maternal GBS antibody concentrations (n = 1096).
GBS, Group B Streptococcus.
‘No result’ indicates assay result with technical concerns making result uninterpretable.
Maternal and neonatal antibody concentrations and transfer ratios by gestational age at delivery (n = 348 pairs).
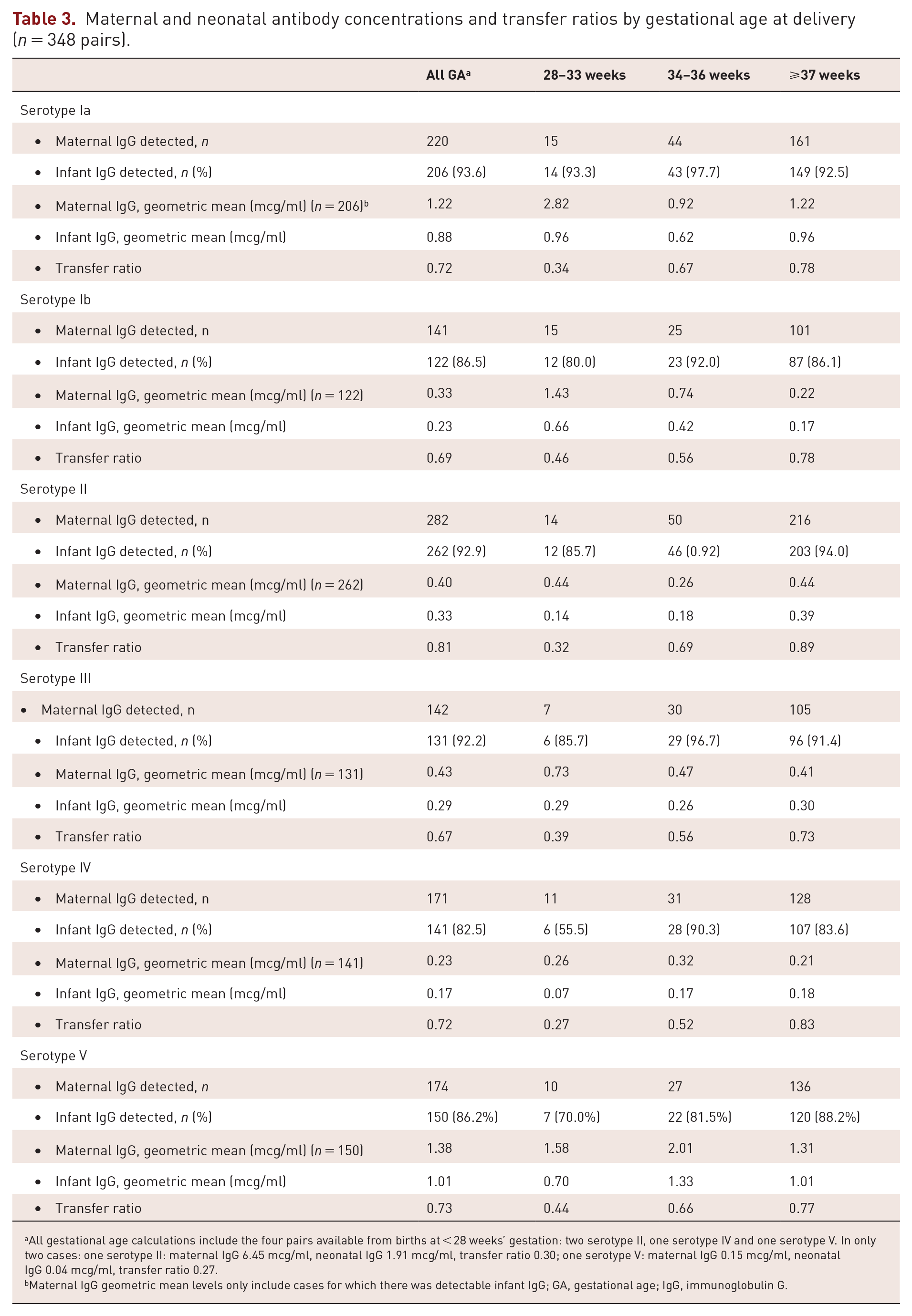
All gestational age calculations include the four pairs available from births at < 28 weeks’ gestation: two serotype II, one serotype IV and one serotype V. In only two cases: one serotype II: maternal IgG 6.45 mcg/ml, neonatal IgG 1.91 mcg/ml, transfer ratio 0.30; one serotype V: maternal IgG 0.15 mcg/ml, neonatal IgG 0.04 mcg/ml, transfer ratio 0.27.
Maternal IgG geometric mean levels only include cases for which there was detectable infant IgG; GA, gestational age; IgG, immunoglobulin G.
Abstract ID: 5
The risk of epilepsy after neonatal Group B Streptococcus disease is modified by the child’s sex, gestational age and maternal socioeconomic position
Malene Risager Lykke1, Henrik Toft Sørensen1, Joy Elisabeth Lawn2, Erzsébet Horváth-Puhó1
1Department of Clinical Epidemiology, Aarhus University and Aarhus University Hospital, Aarhus, Denmark, 2Faculty of Epidemiology and Population Health, London School of Hygiene & Tropical Medicine, London, UK
Objective: To evaluate the risk of epilepsy among GBS-affected infants in various sub-groups.

Proportion of the incidence rates per 1000 person-years attributable to Group B Streptococcus alone, sex (boy versus girl), prematurity (preterm versus term), maternal education (medium versus low and high versus low), and the interaction.
Proportion of the incidence rates per 1000 person-years attributable to Group B Streptococcus alone, sex (boy versus girl), prematurity (preterm versus term), maternal education (medium versus low and high versus low), and the interaction.
Abstract ID: 6
Evaluation of clinical-epidemiological aspects and pathogenicity of Streptococcus agalactiae isolated from pregnant women and newborns
1Laboratory of Molecular Biology and Physiology of Streptococci, Institute of Biology Roberto Alcantara Gomes, Rio de Janeiro State University (UERJ), Rio de Janeiro, Brazil, 2Department of Medical Microbiology, Universidade Federal do Rio de Janeiro, Rio de Janeiro, Brazil
*Correspondence should be addressed to:
†Authors contributed equally to this work.
Abstract ID: 7
Characterization of Group B Streptococcus isolated from carriage and infection in Brazil since 1978 regarding surface proteins, serotypes, sequence types, and resistance
1Instituto de Microbiologia Paulo de Góes, Universidade Federal do Rio de Janeiro, Rio de Janeiro, Brazil, 2Faculdade de Medicina and Maternidade Escola, Universidade Federal do Rio de Janeiro, Rio de Janeiro, Brazil, 3Wellcome Sanger Institute, Hinxton, UK
CC1 (30.6%), CC23 (27.8%), and CC17 (22.2%), although CC19 (11.1%) and CC130 (5.6%) were also found. A total of 80.6% of dGBS carried tet genes (tetM = 63.9%, tetO = 16.7%, tetL = 2.8%), but macrolide resistance genes were not identified. As seen among cGBS, nearly all (97.2%) dGBS carried alpha protein family genes (rib = 55.6%, alp1 = 22.2%, alpha = 11%, alp2/3 = 8.3%), pili genes (PI-1 = 61%, PI-2a1 = 39%, PI-2a2 = 33%, PI-2b = 22%), and serine-rich repeat glycoprotein determinants (srr1 = 75%, srr2 = 22%).
Abstract ID: 8
COVID-19 pandemic and fluctuations in the Group B Streptococcus colonization rates among pregnant women in Brazil
1Instituto de Microbiologia Paulo de Góes, Universidade Federal do Rio de Janeiro, Rio de Janeiro, Brazil, 2Maternidade Escola, Universidade Federal do Rio de Janeiro, Rio de Janeiro, Brazil, 3Public Health England, London, UK
Abstract ID: 9
Breast milk sugars inhibit the proinflammatory response in response to Group B Streptococcus infection
Rebecca E. Moore and Jennifer A. Gaddy
Vanderbilt University Medical Center, Tennessee, USA
Abstract ID: 10
Epidemiology of Group B Streptococcal Meningitis in the United States, 2008–2021
1Division of Bacterial Diseases, Centers for Disease Control and Prevention, Atlanta, GA, USA, 2Epidemic Intelligence Service, Centers for Disease Control and Prevention, Atlanta, GA, USA, 3California Emerging Infections Program, Oakland, CA, USA, 4Berkeley School of Public Health, University of California, Berkeley, CA, USA, 5Colorado Department of Public Health and Environment, Denver, CO, USA, 6Connecticut Department of Public Health, Hartford, CT, USA, 7Atlanta VAMC and Department of Medicine, Emory University School of Medicine, Atlanta, GA, USA, 8Johns Hopkins Bloomberg School of Public Health, Johns Hopkins University, Baltimore, MD, USA, 9Minnesota Department of Health, St. Paul, MN, USA, 10New Mexico Emerging Infections Program, New Mexico Department of Health, Santa Fe, NM, USA, 11New York State Department of Health, Albany, NY, USA, 12Public Health Division, Oregon Health Authority, Portland, OR, USA, 13Department of Health Policy, Vanderbilt University School of Medicine, Nashville, TN, USA
Abstract ID: 11
Alternative molecular typing method of serotype III Group B Streptococcus by CRISPR1-RFLP
Instituto de Microbiologia Paulo de Góes, Universidade Federal do Rio de Janeiro, Rio de Janeiro, Brazil
Abstract ID: 12
Call for action: preventive strategies for Group B Streptococcus late-onset sepsis are needed
1University of Modena and Reggio Emilia, Modena, Italy, 2Neonatal Intensive Care Unit, University Hospital of Modena and Reggio Emilia, Modena, Italy, 3Department of Medical and Surgical Sciences for Mother, Child and Adult, University of Modena and Reggio Emilia, Modena, Italy, 4Department of Specialistic, Diagnostic and Sperimental Medicine, Sant’Orsola Malpighi Univesity Hospidal, University of Bologna, Bologna, Italy, 5Pediatric Postgraduate School, University of Modena and Reggio Emilia, Modena, Italy, 6Unit of Microbiology, Reference Center for Microbiological Emergencies (CRREM), Sant’Orsola Malpighi University Hospital, Bologna, Italy, 7Department of Infectious Diseases, Istituto Superiore di Sanità, Rome, Italy
When considering full-term infants, the incidence of EOD (0.19 per 1,000 LBs 95% CI: 0.16–0.23) and LOD (0.23 per 1000 LBs 95% CI: 0.19–0.27) remained stable. Among preterm infants, the incidence of LOD (1.61 per 1000 LBs 95% CI: 1.26–2.04) was more than twice than that of EOD (0.70 per 1000 LBs 95% CI: 0.48–1.00) and steadily increased from 1.62 per 1000 LBs in 2003–2006 to 2.88 per 1000 LBs in 2015–2018 (p < 0.01). Notably, in the last period (2015–2018), the incidence of LOD among preterm infants (2.88 per 1000 LBs 95% CI: 1.92–4.16) was almost 10-time fold higher than that of EOD (0.31 per 1000 LBs 95% CI: 0.06–0.90, p < 0.001). GBS isolates remained universally susceptible to penicillin.
Abstract ID: 13
Patterns of intrapartum antibiotic chemoprophylaxis and efficacy in preventing GBS vertical transmission—a mini-review
1Neonatal Intensive Care Unit, University Hospital of Modena, University of Modena and Reggio-Emilia, Modena, Italy, 2University of Modena and Reggio-Emilia, Modena, Italy
Abstract ID: 14
The acceptability of implementing routine GBS testing from the perspectives of women and healthcare professionals participating in the GBS3 trial in the UK
1Centre for Maternal and Child Health Research, City, University of London, UK, 2Nottingham Clinical Trials Unit, University of Nottingham, UK, 3Population and Lifespan Unit, School of Medicine, University of Nottingham, UK
Abstract ID: 15
Prevalence and antimicrobial susceptibility pattern of anorectal and vaginal Group B Streptococci isolates among pregnant women in Jimma, Ethiopia
1Department of Medical Laboratory Science, School of Medicine and College of Health Sciences, Debre Markos University, Debre Markos, Ethiopia, 2Department of Medical Laboratory Science and Pathology, College of Public Health and Medical Sciences, Jimma University, Jimma, Ethiopia, 3Armauer Hanssen Research Institute, Addis Ababa, Ethiopia
Footnotes
Correction (June 2023):
Article updated to correct Figure 1 appearing under Abstract ID: 5.