
Abstract
Treatment of Stenotrophonomas maltophilia infections is difficult due to its predilection to form biofilms and susceptibility to a limited number of antibiotics. We report a case of S. maltophilia-associated periprosthetic joint infection successfully treated with a combination of the novel therapeutic agent, cefiderocol, and trimethoprim-sulfamethoxazole after debridement and implant retention.
Introduction
Stenotrophomonas maltophilia (S. maltophilia) is a Gram-negative rod mostly associated with hospital-acquired infections in immunocompromised patients. 1 Major sources of S. maltophilia are water and numerous types of hospital surfaces, including ventilators, invasive devices and catheters, and community food sources. 1 This organism predominantly causes respiratory tract infections and, less commonly, infections of the urinary tract, soft tissue, and wounds. 1 Risk factors for infection include invasive procedures and prior antibiotic use. 1 S. maltophilia is considered a low virulence organism, though its ability to attach to surfaces and secrete extracellular proteinases are two virulence factors that contribute to its pathogenicity. The resistance mechanisms that enable it to evade host defenses and limit options for treatment include reduced outer membrane permeability, an ability to form biofilms, and multidrug efflux pumps. 1
Current treatment options for S. maltophilia include trimethoprim-sulfamethoxazole (TMP-SMX), which is the first-line treatment, in addition to fluoroquinolones, minocycline, and for salvage therapy, a combination treatment with the above and either cephalosporins/beta-lactamase inhibitors or colistin.1,2 This organism is resistant to many beta-lactam antibiotics including carbapenems. 2 Cefiderocol, a novel cephalosporin that exploits S. maltophilia’s ability to scavenge iron to enter the bacteria, is a new addition to the limited treatment options for this organism. 3
Little more than a dozen of bone and joint infections due to S. maltophilia are published and only five involve prosthetic joints.1,4–7 Thus, there is a paucity of guidance in the literature related to treatment of these challenging implant-associated infections. Here, we report successful treatment of a S. maltophilia periprosthetic joint infection (PJI) after posttraumatic revision of a total knee arthroplasty (TKA) to distal femoral replacement without prosthesis removal using the novel therapeutic agent, cefiderocol, in combination with TMP-SMX.
Case description
A 52-year-old woman with a medical history of breast cancer metastatic to multiple sites on lapatinib, hypertension, and history of left TKA 9 years prior sustained a Type 3A open periprosthetic left distal femur fracture in a motor vehicle collision (Figure 1). Associated injuries included a quadriceps tendon rupture and closed tibial shaft fracture. She received 2 g of cefazolin and 5 mg/kg of gentamicin upon arrival to the emergency room and was urgently treated with surgical irrigation and debridement and left lower extremity external fixator placement. She was continued on IV cefazolin 2 g every 8 h until definitive revision surgery, and in delayed fashion, she was treated with conversion of her TKA to distal femoral replacement (Figure 1). She remained on standing IV cefazolin 2 g every 8 h until indwelling drain was removed a week later and initially recovered well. However, approximately 3 months later, she presented to clinic with increasing pain within the knee. Due to concerns in clinic for a PJI, arthrocentesis was performed. The synovial fluid analysis revealed 3960 nucleated cells/ml with 85% granulocytes and S. maltophilia was identified using Vitek. It was found to be sensitive to TMP-SMX [minimum inhibitory concentration (MIC) ⩽1/19 µg/ml], levofloxacin (MIC 2 µg/ml), and minocycline (MIC 1 µg/ml). Irrigation and debridement (I&D) of the knee/distal femur with single stage revision of all modular components of the distal femoral replacement was performed (cemented stems remained in place) with placement of minocycline-loaded biocomposite beads (Stimulan®, Biocomposites, Wilmington, NC, USA). Intraoperative culture again grew S. maltophilia. Levofloxacin was administered post-operatively, first in intravenous then in oral form, which was transitioned to oral minocycline 100 mg q12h monotherapy upon discharge home. The patient was plagued with postoperative wound drainage concerning for persistent infection; therefore, she returned to the operating room for three additional surgical I&Ds until intraoperative cultures were negative.
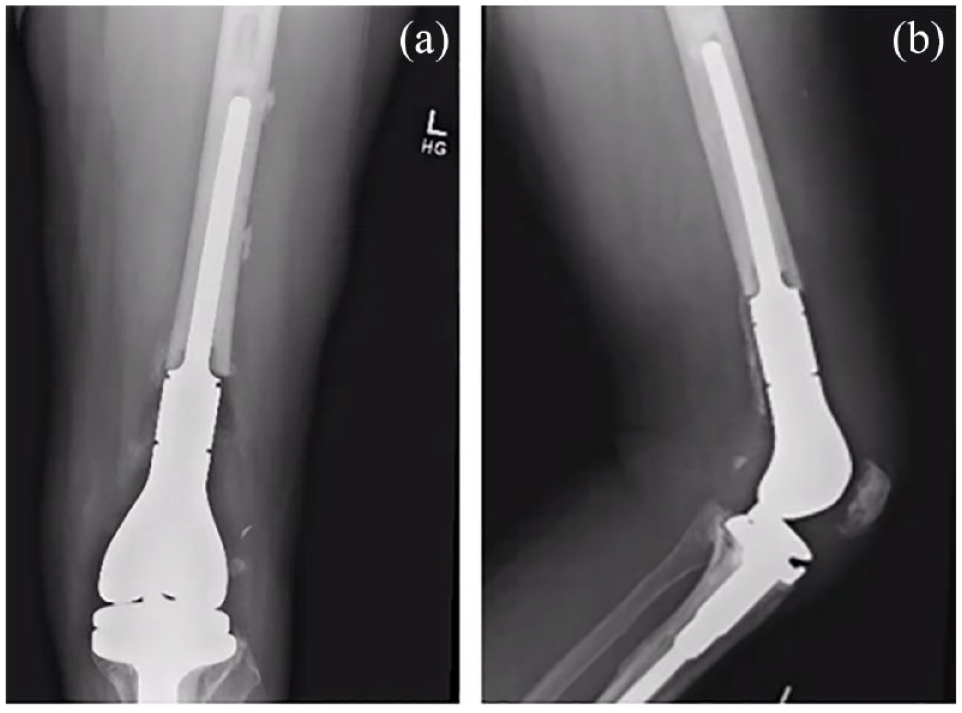
(a and b) The anteroposterior and lateral radiographs, respectively, of the distal femoral end-prosthetic replacement construct performed for comminuted periprosthetic distal femur fracture. Subsequently, this implant developed periprosthetic infection treated with multiple washouts, modular component exchanges, and antibiotics as described.
Based on prior reports of Stenotrophomonas PJI treatment using dual antibiotic therapy and the in vitro demonstration of synergy between cefiderocol and TMP-SMX, the patient was initiated on cefiderocol 2 g every 8 h after the initial I&D on readmission, and TMP-SMX double-strength (DS) 2 tabs orally twice daily was added 2 days later.6,8 While on dual antibiotic therapy, the patient developed hyperkalemia, which resolved after lisinopril was discontinued, and nausea, which was well-controlled with ondansetron and lorazepam. Cessation of TMP-SMX was offered, but the patient wished to continue both antibiotics. Erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) were followed throughout the course of this infection and began to trend downward upon initiation of IV cefiderocol. Due to a no-show at the 6-week endpoint appointment, the patient completed 8 weeks of dual antibiotic therapy. At 2-month follow-up after her final I&D, the ESR and CRP had normalized, the incision was well healed, and symptoms of pain, swelling, and erythema had resolved. She continued suppressive TMP-SMX DS one pill twice daily for 6 months after cessation of cefiderocol and continues to have full ambulatory function, well-healed surgical incisions, and evidence of durable infection eradication at 20 months from most recent surgery.
Discussion
The incidence of S. maltophilia infections and its growing resistance to empirical antibiotic treatments are challenging when formulating an active and tolerable antibiotic plan. Its role in musculoskeletal system infections has not been well documented in the current literature. However, S. maltophilia readily forms biofilms and should be in the differential diagnosis of PJIs that develop in the setting of recent healthcare system exposure.
Treatment of PJIs is challenging, both surgically and microbiologically, especially due to biofilm formation, which is a well-known property of S. maltophilia. Generally, deep tissue penetration and high doses of antimicrobial therapy are required in addition to removal of the prosthesis in order to achieve long-term effective infection eradication. 7 Debridement, antibiotics, and implant retention (DAIR) is one surgical option for PJI that occurs within 3 months of implantation versus 1-stage and 2-stage exchanges.9,10 Gram-negative infections have variable outcomes with the DAIR approach.9,10 A two-stage exchange approach is recommended for multidrug-resistant organisms, but in this case this was not feasible due to the large size of the implant and defect that would have resulted, and the patient fervently declined an above-the-knee amputation. 9 Thus, in this case, biofilm formation by S. maltophilia on the prosthesis and the inability to completely remove it prompted the initiation of a novel therapeutic agent.
Cefiderocol, a novel siderophore cephalosporin, was Food and Drug Administration (FDA) approved in 2019 for the treatment of complicated urinary tract infections and hospital-acquired and ventilator-associated pneumonia. 11 Its utility in treating multidrug-resistant bacterial infections in addition to less common non-lactose-fermenting Gram-negative rods, such as S. maltophilia, has been demonstrated. 3 The unique ability of cefiderocol to facilitate entry into bacterial cells via active membrane-bound iron transporters gives it an advantage over more commonly used antibiotics that are susceptible to bacterial efflux pumps, lack of porin channels, and inactivation by carbapenemases. 3 Furthermore, another advantage of cefiderocol is its ability to not only penetrate but also reduce the mass of Stenotrophomonas biofilms. 12 Due to the novelty of cefiderocol, we were unable to locate commercial susceptibility testing; thus, the patient’s Stenotrophomonas isolate was unable to be tested for cefiderocol susceptibility. However, we were confident in its activity against our patient’s isolate because cefiderocol is indeed novel and multiple published time-kill studies demonstrated cefiderocol susceptibility among all tested Stenotrophomonas isolates. 8
The use of combination therapy in multiple published reports of Stenotrophomonas musculoskeletal infections was the foundation to use two antibiotics in this case.4,6,7 Furthermore, in vitro synergy between cefiderocol and each of the following: TMP-SMX, levofloxacin, and minocycline has been demonstrated. Our rationale to use cefiderocol and TMP-SMX in combination was twofold. First, TMP-SMX is the treatment of choice for S. maltophilia. Second, the combination of cefiderocol and TMP-SMX had the highest rate of bactericidal activity in synergy studies compared with cefiderocol in combination with levofloxacin or minocycline. 8
In this case of a S. maltophilia PJI in which the prosthesis was unable to be completely removed and replaced with a temporary spacer, treatment with cefiderocol in combination with high-dose TMP-SMX after DAIR proved to be efficacious when minocycline monotherapy failed. We hope that this case will add to the limited literature detailing treatment of Stenotrophomonas musculoskeletal infections and increase awareness of cefiderocol as an option for S. maltophilia PJI.
For patients with rare S. maltophilia musculoskeletal infections such as PJI, the continued development and increased awareness of the novel therapeutic options available are imperative. In addition, the potential for monotherapy failure should be considered when selecting treatment. The ability of cefiderocol to penetrate biofilms may also have contributed to the successful outcome in this patient after DAIR. The use of cefiderocol as part of combination therapy substantiates its efficacy and thus should be considered a viable option for Stenotrophomonas maltophilia PJI therapy.