
Abstract
Introduction:
Innovative discovery begins with diverse perspectives; research teams should harness this model. Black, Indigenous, and other People of Color (BIPOC) and women are underrepresented as researchers. Team science leverages collaborative and cross-disciplinary approaches to diversify the research workforce, and introduces academic (and non-academic) faculty with limited research exposure/experience to clinical research.
Methods:
In 2020, two Black women academic physicians implemented an academic collaborative – COVID-19 Characteristics, Readmissions, Outcomes, and Social Determinants of Health (CROSS) – to investigate COVID-19 health inequities, with intentional recruitment of BIPOC and women. The 37 CROSS team members were of diverse races, ethnicities, sex, specialties, and disciplines, and represented eight hospitals. Team members were electronically surveyed to determine their interest, desired activities, and level of participation in research activities; concurrently, self-identified demographics (including race, ethnicity, sex, and language(s) spoken) were obtained.
Results:
All team members completed the survey: 78.4% (n = 29) were BIPOC and 78.4% (n = 29) were women. Team members spoke 18 languages (including English). Academic medical ranks included Assistant Professor (32.4%; n = 12), Associate Professor (16.2%; n = 6), and Full Professor (2.7%; n = 1). Each member identified desired activities (data collection, data analytics, manuscript development, abstract development/poster presentation, serving as a consultant) and the percentage of time they intended to allocate to each. Between June 2020 and February 2023, the team produced five original peer-reviewed manuscripts (including this article); five members served as first or senior authors. Twenty-one abstracts were presented at local conferences, and 10 at national and regional conferences. Five members achieved academic promotion, and team members were awarded three intramural grants resulting directly from team collaborations.
Conclusion:
Intentional recruitment and assessment of team members’ desired levels of participation in an integrated clinical research team is an effective strategy to engage BIPOC and women. The CROSS Collaborative is a model for diversity and inclusion in team science and clinical research.
Keywords
Introduction
Building a diverse and inclusive workforce begins with an awareness of the current state followed by intentional actions to address gaps. Medical school faculty are comprised of diverse disciplines; however, the diversity of this biomedical workforce has yet to reflect the population it serves. The 2020 United States Census found that 42.2% of the population identified as Black, Indigenous, and other People of Color (BIPOC), with 18.7% identifying as Hispanic or Latino and 12.1% as Black or African American. 1 As of 2018, though 36.1% of full-time US medical school faculty identified as BIPOC, only 3.6% were Black (or African American) and 5.6% were of Hispanic, Latino, or Spanish origin.2,3 Medical school faculty engaged in research has a diversity gap, as demonstrated in 2018 data from the Association of American Medical Colleges (AAMC) where 8747 White physicians listed research as a major professional activity compared with 3992 physicians in all other racial/ethnic categories combined. 4 A diverse biomedical workforce is necessary to mitigate health inequities and has been associated with improved patient satisfaction, medication adherence, and reach into BIPOC and medically underserved communities.5–7 To provide the best care to diverse patient populations, it is necessary that the biomedical workforce represents the community in terms of race/ethnicity, sex, immigration status, sexual orientation, physical ability status, and socioeconomic class. 7
Diverse teams outperform less diverse teams and are associated with better problem solving and improved innovation. 8 Ethnically diverse research teams are associated with increased publication citations and publications in higher impact journals.9,10 One analysis of more than 6 million scientists and 9 million manuscripts assessed research impact and its relationship with five classes of diversity (ethnicity, sex, affiliation, discipline, and academic age); the diversity class most strongly associated with scientific impact was ethnic diversity, with an impact gain of 46.7% for scientists and 10.6% for manuscripts. 9 Women remain underrepresented as research paper authors, especially in senior authorship: one study of authors who published COVID-19 manuscripts early in the pandemic (early 2020) found that women represented 34% of all authors, with lower percentages of both first and last authors. 11 Sex heterogeneity in authorship teams resulted in 34% more citations in journal articles than in sex-uniform teams. 12
Diversity in the research workforce allows for innovation in ideas and the expansion of scientific research questions that target traditionally underrepresented populations; conversely, lack of diversity limits research questions and interpretation of the results, and negatively impacts the engagement of marginalized populations in research studies.8,13 In order to maintain a diverse research workforce, diversifying the network of mentors is essential. 13 Team science collaborations among diverse researchers aid in addressing complex research questions by applying concepts and methodology from multiple disciplines, professions, and cultures, resulting in impactful and effective collaborative interprofessional research practice.14–17
An academic collaborative, titled CROSS (COVID-19 Characteristics, Readmissions, Outcomes, and Social Determinants of Health Study), was developed and led by two Black women academic physicians (Assistant Professor and Associate Professor at the inception of the team) with intentional and targeted recruitment of predominantly BIPOC and women team members. In this article, we describe the team formation and scholarly output of our cross-disciplinary academic clinical research team that was developed to investigate COVID-19 health inequities.
Methods
Recruiting the team
The CROSS Collaborative was established in June 2020 to investigate COVID-19 health inequities, leveraged by the perspectives of a purposefully diverse research team. Intentional and targeted recruitment of predominantly BIPOC and women was conducted. There was no target number of team members or proportion of BIPOC and women sought; however, diversity with respect to race, ethnicity, sex, specialties, disciplines, academic rank, hospital representation, and hospital systems leadership was a priority when recruiting team members.
Academic medical center faculty who were investigating (or interested in investigating) clinical research questions related to patients hospitalized with COVID-19 were recruited. Team members were sought if they were involved in direct care of patients hospitalized (or readmitted) with COVID-19 (e.g. hospitalists) as well as non-hospital based clinicians who would subsequently care for these patients in the outpatient setting (e.g. family medicine and internal medicine physicians). The team members involved in direct patient care provided care of patients at eight Atlanta, Georgia, hospitals. Four hospital systems (including eight hospitals) were included: an academic health system (six hospitals), a historically Black academic medical system (one hospital), a traditionally non-academic health system (providing inpatient care in two of the academic health system hospitals), and a US Department of Veterans Affairs system (one hospital). The hospitals included a small hospital (less than 100 beds), medium hospitals (between 100 and 499 beds), and large hospitals (500 or more beds). Of the six academic health system hospitals, one was small, three were medium, and two were large. The US Department of Veterans Affairs system hospital was medium, and the historically Black academic medical system hospital was large.
Considering the quality improvement, resource utilization, primary care, and public health implications of patients being hospitalized and readmitted to the hospital, key stakeholders with leadership roles and expertise in these areas were personally invited to the team by one of the team leads (who also served as the Chief Quality Officer at one of the academic institutions). She leveraged her relationships with fellow academic leaders and was instrumental in inviting, via email and personal communication, another physician who served as the Chief Medical and Chief Quality Officer of an academic healthcare network. Several infectious disease physician team members also served in leadership roles at their respective institutions (e.g. Medical Directors of Antimicrobial Stewardship, a Chief of Infectious Diseases, and an Associate Hospital Epidemiologist).
There was a desire to leverage various innovative data analytic methodologies such as machine learning and integration of social determinants of health; thus, additional partnerships with epidemiologists were leveraged. Next, representation of medical trainees and faculty at various ranks (Assistant Professor, Associate Professor, and Full Professor) was sought to provide exposure to research collaboratives and connection to more experienced research mentors. Finally, recruitment efforts focused on those with an interest or expertise in health disparities research and interventions.
Determining team member demographics, desired research team activity, and intended level of participation
Once the full team was established, assessment of desired participation was critical to engagement, accountability, and appropriate representation of contribution to scholarly content. An initial electronic survey was sent to each member in March 2021 to document their self-identified demographics. The demographic survey consisted of eight questions, including members’ name; institution (e.g. academic institution, Veterans Affairs); primary hospital of employment; sex (only consisting of a free text box to allow members to fully self-identify themselves with no restrictions); race/ethnicity (also only a free text box to allow members to fully identify themselves with no restrictions); academic rank/non-academic role [Assistant Professor, Associate Professor, Full Professor, Non-academic Physician, Advanced Practice Provider (nurse practitioner or physician assistant), Trainee (medical student or internal medicine resident), and Research/Quality Staff (data analyst, project manager)]; a free text box for ‘other’ leadership roles (e.g. Chief of Service, Chief Quality Officer, Hospital Epidemiologist); and a question asking what language(s) were spoken in addition to English (free text box only).
A second survey was performed in March 2021 to assess each team member’s research team activity interest and intended level of participation. Five activities were provided: data analytics, data collection, manuscript development, abstract development/poster presentation, and serving as a consultant. Level of participation was assessed by quantifying the proportion of time that each team member intended to contribute to each activity (by quartiles): none; 1–25%; 26–50%; 51–75%, or 76–100%.
Structure of meetings
Administrative structure was instituted that included team meetings (30 min–1 h) held virtually on a weekly basis during the first year and then twice monthly during the second year. Team members were encouraged to attend, but were not penalized for lack of attendance (especially given clinical, administrative, and family responsibilities during the COVID-19 pandemic). The team meetings incorporated five standing agenda items: grant status updates, data collection and analysis updates, regulatory affairs updates, scholarly updates (e.g. abstract progress, manuscript progress), and next steps/distribution of responsibilities. A 5-min ‘Celebrations’ agenda item (e.g. promotions, academic and non-academic celebratory items) was subsequently added to the agenda as well. A four-woman steering committee, including the two team leaders (Black women at the ranks of Assistant and Associate Professor at the inception of the team), a hospitalist service lead physician (a White woman), and project manager (a Black woman), was also developed and met virtually for 30 min twice monthly.
Evaluation of scholarly output
The steering committee maintained records of all scholarly activities, the team members who participated in each activity, the name(s) of the members who served as presenting author, lead author, and senior author on each abstract and manuscript. The project manager managed the Institutional Review Board (IRB) and Data Use Agreement approvals between healthcare systems and hospitals, monitored grant expenditures, arranged and scheduled the virtual meetings for both the steering committee and the CROSS research team, and developed data collection tools.
Results
Team member demographics, desired research team activity, and intended level of participation
All 37 team members responded to the demographics survey: 29 (78.4%) were BIPOC and 29 (78.4%) were women (Table 1). Eighteen languages (including English) were spoken by team members (Table 1). Academic medical ranks included 12 (32.4%) Assistant Professors, 6 (16.2%) Associate Professors, and a single (2.7%) Full Professor. Medical trainees (medical students and internal medicine residents) comprised 13.5% (n = 5) of the team (Figure 1). Non-academic roles were comprised by 35.1% (n = 13) of the team, and these roles included advanced practice providers (a nurse practitioner and three physician assistants), two non-academic physician administrators, four non-academic physicians, as well as three research/quality team members (a hospital medicine research supervisor, a data analyst, and a data scientist) (Figure 1).
Demographic characteristics of CROSS team members.

BIPOC, Black, Indigenous, and People of Color.
BIPOC was defined as individuals who identified as Black, African American, Non-Hispanic; Black/South-Asian; Hispanic, Latina; Asian; Asian American; Asian Indian; and South Asian. Individuals who identified as White, Caucasian, non-Hispanic were not categorized as BIPOC.
Individuals could select more than one language spoken, so categories are not mutually exclusive.
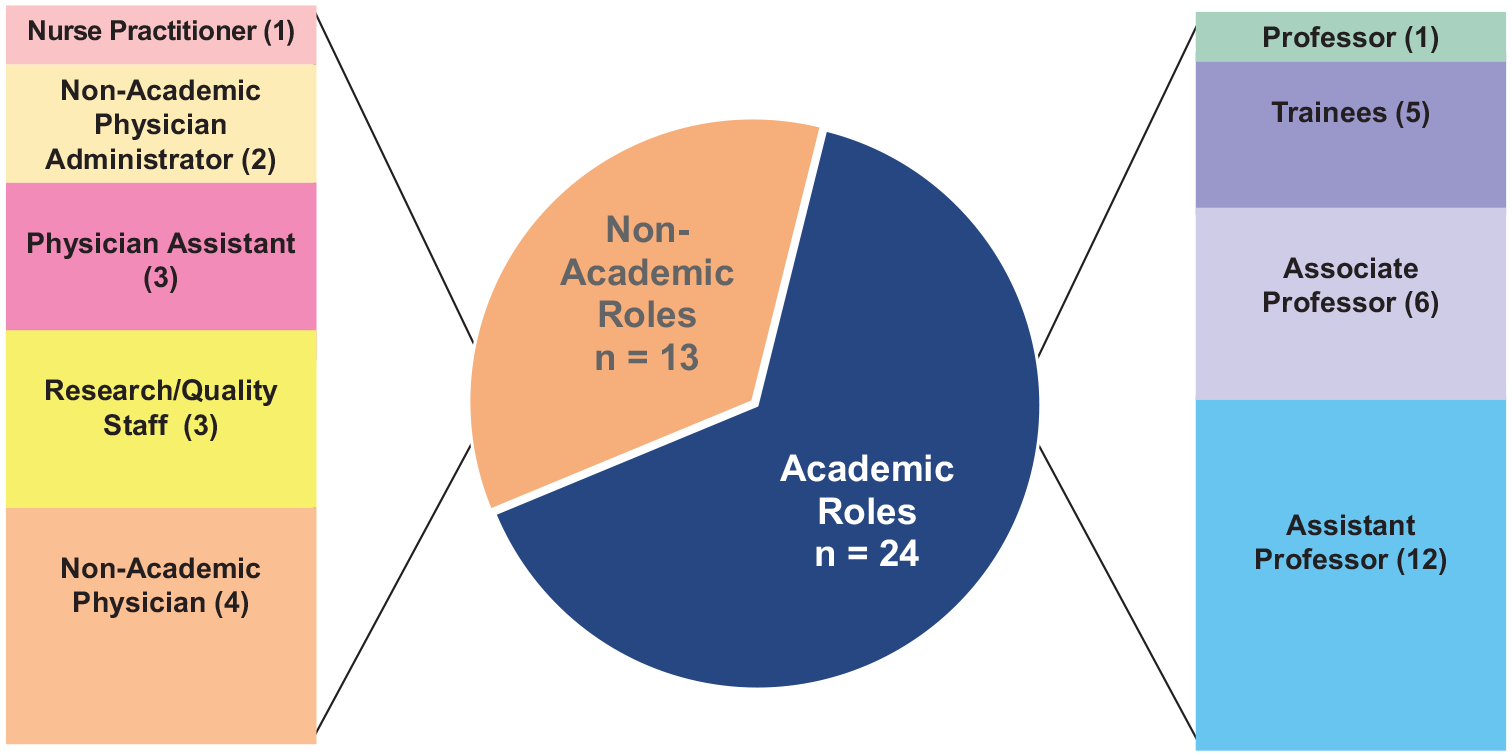
CROSS team member roles.
Many team members held senior leadership roles within their hospital or healthcare system (e.g. hospital Chief Information Officer, Chief Quality Officer, Chief of Infectious Diseases, Hospital Medicine Service Directors, Director of Antimicrobial Stewardship, Assistant Health Director of a primary care clinic). Most team members were employed by academic hospitals or health systems (n = 35, 94.6%).
The majority of team members (n = 36, 97.3%) responded to the research activity interest and participation survey (Figure 2). There was a varied distribution of CROSS team members’ desired areas of participation by intended allocation of effort. For example, for data analytics, 16.7% (n = 6) of the 36 team members who responded to the survey wanted to spend more than 50% of their time dedicated to this effort. On the contrary, 36.1% (n = 13) of the respondents wanted to devote over 50% of their time to data collection.
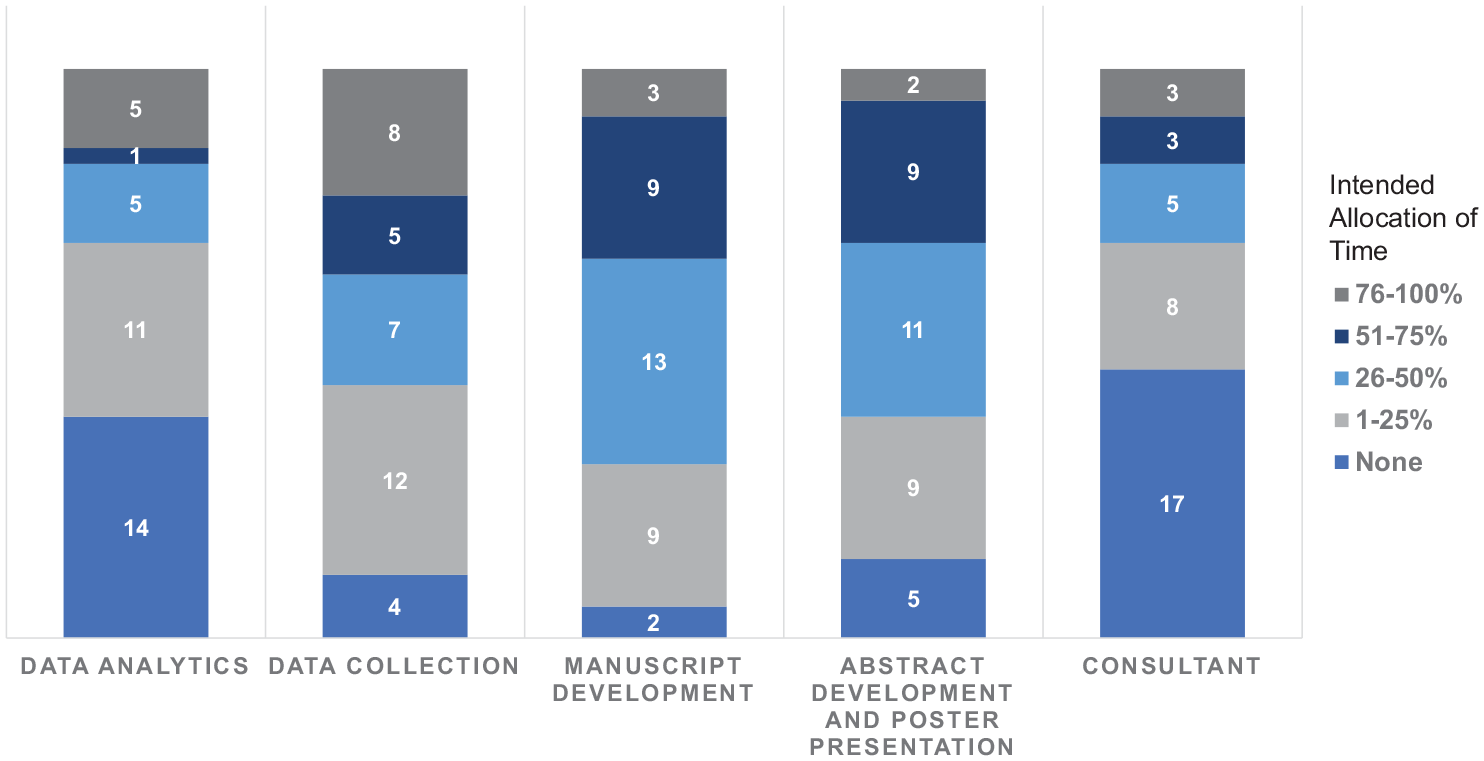
Distribution of CROSS team members’ desired areas of participation by intended allocation of effort.
Scholarly outputs
The CROSS team had three intramural grants funded over the 2 years described. The first, and largest, CROSS grant funded was $200,000 via an intramural COVID-19 funding opportunity. The two team leads (both Black women) served as co-Principal Investigators (co-PIs) for this grant. A large proportion of the grant funding was allocated to protecting the academic time of most of the team members (ranging from a low of 2% for most team members and up to 20% for the project manager). The grant funding was also utilized to pay the cost of manuscript publications, abstract submission fees, and travel to national conferences to present abstracts. Two $25,000 seed grants were subsequently funded; both had CROSS members serve as PIs for the grant opportunities (one to support a COVID-19 vaccine web-based decision tool and one to support a machine learning prediction tool to evaluate kidney disease in COVID-19 survivors). Both of the recipients of the seed grants (Asian men) were at the rank of Assistant Professor when the grants were awarded.
Multiple abstracts were presented by CROSS members. Twenty-two abstracts were submitted to conferences and 21 (95.5 %) were accepted. Of the 21 accepted abstracts, 5 (23.8%) were accepted to national conferences (4 poster presentations and 1 oral presentation), and 5 (23.8%) were accepted to regional conferences (all oral presentations); the remaining 11 were presented in institutional venues, either as poster presentations (n = 9) or oral presentations (n = 2). One member (a Black woman at the rank of Assistant Professor) won the Best Clinical and Health Services Research Oral Presentation Award at the 2021 Emory School of Medicine Department of Medicine Research Day. The CROSS Collaborative received both the second-place and third-place awards for two separate abstract presentations at the 2021 Emory Division of Hospital Medicine Research Day.
A significant proportion of CROSS members (n = 12, 32.4%) served as presenters of accepted abstracts [including a medical student (Black woman), an internal medicine resident (Asian woman), the project manager (Black woman), and a data analyst (White woman)]. A total of five manuscripts, including this article, were published between June 2020 and Feb 2023. The primary CROSS manuscript published was titled ‘Clinical Characteristics and Social Determinants of Health Associated with 30-day Hospital Readmissions of Patients with COVID-19’. 18 Three other publications followed, including a publication on COVID-19 vaccine hesitancy in healthcare workers, one evaluating telemedicine versus in-person visits and one assessing differences in diabetes control in telemedicine versus ambulatory in-person-only visits.19–21 Five CROSS members served as first or senior author on these manuscripts, including the two Co-PIs, data analyst, an Assistant Professor, and two Associate Professors.
Professional development, service, media, and community outreach
Five CROSS team members were awarded academic promotion between June 2020 and February 2023. The co-PIs were promoted (one to Full Professor and one to Associate Professor). Three other members were promoted to Associate Professor. All five promoted team members were BIPOC (three Black women, one Latina woman, and one Asian male). We also celebrated the promotion of our data analyst (White woman) from a Data Analyst II to a Data Analyst III position. Other accomplishments by team members included receipt of hospital advocacy awards, guest editor and author for a local medical association journal issue on COVID-19, acceptance into scientific leadership development programs, and promotion to academic system outpatient Chief Quality Officer.
Community service is a pillar in the CROSS Collaborative, and the CROSS team members were very active in academic and non-academic COVID-19-related outreach. This non-traditional scholarship work included articles in major print and news outlets, national outreach, social media, and local community outreach. The community outreach included COVID-19 vaccine events at historically Black Atlanta churches, COVID-19 vaccine education at a science fair, webinars targeting women members of historically Black sororities, and outreach to the Latinx community via in-person and virtual events (Table 2). The CROSS Collaborative (under the umbrella of the Emory Woodruff Health Sciences Center’s Collaborative Community Outreach and Health Disparities group) were group award recipients of the 2021 Emory School of Medicine Martin Luther King Service Award.
Outreach and non-traditional scholarship activities.

NA, not available.
Discussion
In this article, we describe the team formation and scholarly output of a diverse and cross-disciplinary academic clinical research team. Our CROSS team was established by two Black women academic physicians. Our 37 team members were predominantly women (n = 29; 78.4%) and BIPOC (n = 29; 78.4%) and comprised persons with both academic (n = 24; 64.9%) and non-academic roles (n = 13; 35.1%). Our team was also diverse in the types of hospitals represented, the specialties of the physicians, and inclusion of advanced practice providers (a nurse practitioner and physician assistants). Our team was very productive over 2 years and scholarly output included five original peer-reviewed manuscripts (including this article); five members served as first or senior authors. Twenty-one abstracts were presented at local conferences, and 10 at national and regional conferences. Five of our members achieved academic promotion, and team members were awarded three intramural grants resulting directly from team collaborations.
We learned that in order to develop a diverse team, there had to be intentionality with respect to recruiting team members. Although the team leads (both Black women) did not have an exact proportion of women and BIPOC in mind when they developed the team, they were very intentional in ensuring that the team was diverse with respect to sex, race, and ethnicity. Also, in the midst of a global pandemic, when many of our team members had additional family responsibilities, we knew that it was essential to ask team members both how much time they had to offer and which activities they were most interested in contributing to.
We found it helpful to ensure that all academic ranks were included as team members which allowed for traditional mentorship opportunities (e.g. an Associate Professor guiding a medical student through abstract preparation) as well as peer mentorship opportunities (e.g. Assistant Professors working together on the vaccine hesitancy manuscript). Our regular meetings provided a platform for information sharing, informed by both personal and clinical experiences, and varied opinions and approaches were welcome and openly discussed. Our team diversity allowed us to benefit from tapping into different networks that expanded our inter-institution collaborations. For example, two of our team members were institutional leaders in quality (one an academic hospital Chief Quality Officer and the other an academic clinic network Chief Quality Officer). This allowed us the advantage of leveraging their leadership to obtain currently available clinical data and broadly survey the workforce of each system in additional research projects. We also took pride in the collaboration between a predominantly White academic healthcare institution with a historically Black academic healthcare institution. Often the ‘minority tax’, the burden of additional responsibilities and activities placed on BIPOC faculty, may not result in academic promotion.22,23 However, our approach to team science allowed for direct mentorship, grant funding, opportunities to present scientific data via abstracts (at institutional, regional, and national venues), and authorship on manuscripts, all of which allowed for promotion opportunities. 23
A key component of the team meetings was a time to share ‘Celebration’ moments which supported engagement and retention of our members. These discussions also provided cultural learning opportunities and further insight into the humanity of the individuals on our team and their desire to impact their communities. One of our team leaders was featured in the New York Times for her personal mission to educate her family and community in rural Alabama on the importance of COVID-19 vaccination (Table 2). This time also provided a safe space to give voice to any challenges at work and home impacting our ability to deliver on our shared goals.
Another strength of our collaborative was the participation of hospitalists. Hospitalists and hospital medicine advanced practice providers comprised a hefty 40.5% (n = 15) of our CROSS team and represented seven of our eight hospitals. Hospitalists are greatly underrepresented as clinician investigators despite rapid growth in the specialty. 24 These groups reported needing support for junior faculty development activities (e.g. research mentorship), opportunities to network with other researchers, and access to multi-site clinical data. 24 Our CROSS Collaborative offered each of these levels of support.
Our collaborative resulted in numerous national, regional, local community, and institutional presentations; successful intramural grant applications; ancillary studies in collaboration with multiple specialties, hospitals, medical schools, and healthcare systems; and five (including this article) peer-reviewed manuscripts. This was especially significant as it fostered opportunities for scholarship and set a prospective for academic and non-academic career advancement.
Conclusion
The ability to establish a diverse team with respect to race, ethnicity, sex, specialties, hospitals, and hospital systems is not readily available to many clinical research teams, especially those that are not associated with academic institutions, those without established research programs, those in rural locations, and, most importantly, those without current BIPOC and women clinicians and researchers. Pathways to increase the numbers of BIPOC and women clinical researchers will take both time and intentional action to increase diversity. Intentional and targeted recruitment ensuring racial and ethnic diversity as well as assessment of team members’ desired levels of participation in an integrated clinical research team is an effective strategy to engage BIPOC and women. The CROSS Collaborative is a model for diversity and inclusion in team science and clinical research.