Phospholipid vesicles for detection of Group B Streptococcus
Emelie E.C. Alsheim1,2, Naing T. Thet1, Maisem Laabei2, A. Toby A. Jenkins1
1Department of Chemistry, University of Bath, Bath, UK, 2Department of Biology and Biochemistry, University of Bath, Bath, UK
Introduction:Streptococcus agalactiae, or Group B Streptococcus (GBS) colonises 20–40% of all pregnant women in the United Kingdom (UK)1. Transmission from mother to child cause serious disease in neonates, which can cause life-long disability, or in worst case, death2. Due to transient carriage of GBS, routine screening during pregnancy is not provided in the UK3.
Objective: Develop a rapid, affordable, and effective point-of-care test for detection of maternal GBS carriage status intrapartum using GBS sensitive phospholipid vesicles: nanoscale spheres of lipid containing a fluorescent dye which on release gives a colour change. GBS expresses virulence factors which breakdown the lipid vesicles, thus effecting dye release, allowing a visual change in colour that can be used as a diagnostic tool.
Method: Phospholipid vesicles containing 5(6)-carboxyfluorescien were produced using standard extrusion protocol. Single species 48-hour old GBS biofilms (from clinical strains of GBS), as well as common commensals were grown on 6mm cellulose membranes. The biofilms were aseptically added to phospholipid vesicle solution and incubated for 45 min at 46°C, after which the fluorescence intensity was measured.
Results: The GBS biofilms showed a significant (p⩽0.01) lysis of the phospholipid vesicles, increasing the absolute fluorescence unit (AFU) compared to most commensals (Figure 1).
Shows AFU after incubation of biofilms with phospholipid vesicles at 46°C for 45 min. Clinical samples of GBS (523, 6073, KX1050, NPX0066, NPX0090, SGX0300), E. faecalis and S. gallolyticus were obtained from St George’s Hospital, London, UK. C. auris were obtained from Public Health England (PHE). P-value ⩽ 0.01 was calculated by a One-Way Anova.
Conclusion: This study demonstrates the possibility of using phospholipid vesicle technology in the future to produce a low cost, rapid, point-of-care swab test to be used intrapartum and post-partum to determine maternal and neonatal carriage.
Acknowledgements
This project has received funding from the European Union’s Horizon 2020 research and innovation programme under the Marie SKŁODOWSKA-CURIE grant agreement No 955664. Thank you to Dr Kirsty Le Doare’s group at St Georges Hospital in London, UK, for clinical samples.
Abstract ID: 2
Subcategory: Vaccines
Naturally acquired serotype-specific anti-GBS CPS IgG concentrations: A pilot UK prospective cohort study
K. Karampatsas1, T. Hall1, L. Ramkhelawon1, N. Andrews2, P. T. Heath1, K. Le Doare1,3,4
1Paediatric Infectious Diseases Research Group, Institute of Infection and Immunity, St. George’s, University of London, London, UK, 2 UK Health Security Agency, London, UK, 3 MRC/UVRI @LHSTM Uganda Research Unit, Entebbe, Uganda, 4 Pathogen Immunity Group, Public Health England, Porton Down, UK
Background & objective: Group B Streptococcus (GBS) is a major cause of invasive neonatal infections (iGBS). A vaccine targeting pregnant women could protect infants through placentally transferred antibodies. We studied naturally derived anti-capsular polysaccharide (CPS) immunoglobulin G (IgG) in UK neonates.
Methods: A prospective cohort study of pregnant women and their infants was conducted in two phases (iGBS feasibility study). Participants were recruited from five maternity units in London and South England from 1st July 2018 to 30th November 2020. iGBS cases were identified through parallel surveillance in selected NHS Trusts in England. Cord blood samples were collected from healthy babies born to mothers with a positive rectovaginal swab obtained from 35 weeks gestation and non-colonised women. Acute disease sera from infants with early-onset GBS disease (EOGBS) were included in the analysis. GBS isolates from colonised women and infected infants were serotyped by PCR. Quantitative serum serotype-specific anti-CPS IgG concentrations were measured using the GASTON multiplex immunoassay (MIA) based on the Luminex technology platform for six serotypes (Ia, Ib, II, III, IV and V).
Results: The analysis included eight serotype III (STIII) EOGBS cases, 30 healthy infants born to colonised mothers with STIII and 264 healthy infants born to non-colonised women. IgG geometric mean concentrations (GMCs) were higher in healthy infants born to GBS colonised women than in neonates with EOGBS (0.10 vs 0.006 µg/mL; P = 0.001). IgG concentrations in cord blood of babies born to colonised women were not affected by demographic factors (maternal age, ethnicity, gestational age) and antenatal clinical factors (co-morbidities, immunosuppressive medication, GBS colonisation in previous pregnancy).
Conclusions: Our findings show a trend for reduced anti-CPS IgG STIII titres in infants that develop STIII EOGBS compared to healthy infants born to mothers colonised with STIII GBS. Compared to previous studies, IgG concentrations were lower across all groups (EOGBS cases, cord blood of infants born to colonised and non-colonised women). These differences could be due to the different assays, and standard sera used. A larger UK case-control study is underway to compare STIII-specific IgG levels in infants with iGBS and infants born to colonised mothers who do not develop iGBS.
Abstract ID: 3
Subcategory: Clinical Care
Rates of lumbar puncture after antibiotics in infants with sepsis: an italian multicenter study
Luca Bedetti1,2, Licia Lugli2, Francesca Miselli2, Barbara Perrone3, Cinzia Auriti4, Cryssoula Tzialla5, Giuseppe Latorre6, Jenny Bua7, Giulia Vellani8, Bacchini Pier Luigi9, Martina Buttera10, Isotta Zinani10, Alberto Berardi2
1PhD Program in Clinical and Experimental Medicine, University of Modena and Reggio Emilia, 2Neonatal Intensive Care Unit, University Hospital of Modena, 3Neonatal Intensive Care Unit, Ospedali Riuniti, Ancona, 4Neonatal Intensive Care Unit, Ospedale Pediatrico Bambin Gesù, Roma, 5Neonatal Intensive Care Unit, San Matteo Hospital, Pavia, 6Neonatal Intensive Care Unit, Miulli Hospital, Bari, 7Neonatal Intensive Care Unit, Burlo Garofalo Hospital, Trieste, 8Neonatal Intensive Care Unit, Civico Hospital, Palermo, 9Pediatric Department, Fidenza Hospital, Parma, 10Pediatric Postgraduate School, University of Modena and Reggio Emilia
Background: Lumbar puncture (LP) is essential for diagnosing meningitis in infants. LP should be performed before the start of antibiotic therapies to maximize the yield of pathogens.
Aim: The aim of this study was to evaluate the rate of LP in infants with culture-proven sepsis, and the proportion of LP performed after initiation of antibiotic therapy.
Methods: Our data comes from an Italian surveillance network (31 centres) on culture-proven bacterial infections (group B streptococcus, E. coli) diagnosed within 90 days of life. Gestational age at LP, rates of LP and the start of antibiotics before LP were evaluated.
Results: From January 2016 to February 2022, 366 neonates were diagnosed culture-proven sepsis (group B Streptococcus, n=234; Escherichia Coli, n=132). Twenty-four (6.5%) of 366 neonates were asymptomatic. Median gestational age at LP was 40 weeks (interquartile 35–43 weeks). LP was performed in 207 infants (56.6%) of which 111 (54.1%) were performed after antibiotic administration, (median 24, IQR 10-48 hours). With respect to E. coli, GBS infections were more likely to undergo an LP (163 of 234, 69.6% vs 44 of 132, 33.3%, p<0.001). LP was less likely to be performed in asymptomatic (7 of 24, 29.2%), with respect to symptomatic neonates (200 of 342, 58.5%, p=0.005)
Discussion: LP is essential to rule out meningitis. However, LP should be postponed in hemodynamically unstable infants or during severe thrombocytopenia. We found a low rate of LP performance and frequently antibiotics were given before an LP. However, the yield of pathogens in cerebrospinal fluid may be lower after antibiotic therapies. Therefore, meningitis would be underdiagnosed, and antibiotic therapies could be less appropriate.
Conclusions: LP should be performed (whenever possible) prior to antibiotic administration in any symptomatic infant with culture-proven sepsis.
Abstract ID: 4
Subcategory: Epidemiology
Invasive Group-B Streptococcus disease in the neonatal period and risk of epilepsy – a population-based cohort study
MR Lykke1, JE Lawn2, HT Sorensen1, E. Horváth-Puhó1
1Department of Clinical Epidemiology, Aarhus University, Denmark, 2Faculty of Epidemiology and Population Health, London School of Hygiene and Tropical Medicine, London, United Kingdom
Background: Group B Streptococcus (GBS) disease is a well-established risk factor for neurodevelopmental impairment, but the risk of epilepsy following GBS in the neonatal period is poorly understood.
Objective: To investigate the association between GBS (sepsis or meningitis) in the neonatal period and the risk of epilepsy, stratified by sex, prematurity, and maternal socioeconomic position (SEP).
Methods: Population-based retrospective, matched cohort study of children born in Denmark between January 1, 1997, and December 31, 2017, followed-up until December 31, 2018, diagnosed with GBS sepsis or meningitis within the first 89 days of life. Matched 1:10 on sex, year and month of birth and gestational age. SEP was defined by maternal income, highest achieved education calculated from the preceding year prior to the child’s birth date. Incidence rates (IRs) calculated as per 1000 person/years and cumulative incidence proportions (CIP) calculated treating death as competing risk. We used Cox proportional hazards regression analysis to compute hazard ratio (HR) including 95% confidence interval (CI) as a measure of relative risk.
Results: 1432 children were registered with GBS, 1264 had sepsis and 168 meningitis. 21·4% (306/1432) were born premature. Median follow-up time was 12·6 years (interquartile range (IQR) 6·3–18 years). Overall CIP of epilepsy in GBS children was 3·64% compared to 2·27% in the comparison cohort. Overall IR for epilepsy in GBS children was 2·39 (95% CI 1·66–3·12) compared to 1·16 (1·00–1·32) in the comparison cohort. The IR for epilepsy in GBS children during the first 5 years of life was 4·52 (95% CI 2·87–6·16) compared to 1·41 (95% CI 1·12–1·69) in the comparison cohort. CIP for GBS meningitis was 15.10% (95% CI 8.92–22.81), and 2.22% (95% CI 1.35–3.44) for GBS sepsis. Adjusted HR for GBS children combined was 2·04 (95% CI 1·46-2·85).
No differences in CIP were found between sexes: boys 3·55% and girls 3·78% (95% CI 2·19–6·03), adjusted HR’s being 2·22 (1·41–3·48) for boys and 1·85 (1·12–3·07) for girls. Premature GBS children had a higher CIP 5·99% (95% CI 3·18–10·05) compared to the comparison cohort 2·04% (95% CI 1·68–2·45). The adjusted HR for epilepsy when born premature was 2·30 (95% CI 1·28–4·13). If the mother belonged to the low-income and low-education group, the CIP for epilepsy increased for iGBS children comparted to the children in the comparison cohort.
Conclusion: Neonatal GBS, especially meningitis, was associated with an increased risk of epilepsy in later childhood. GBS Children born premature had a higher cumulative risk of epilepsy than GBS children born at term. Furthermore, the cumulative incidence and incidence rate of epilepsy increased if the mother was categorized in the low-income group compared to the high-income group.
Abstract ID: 5
Subcategory: Clinical care
Incidence of maternal Group B Streptococcus (GBS) bacteraemia and clinical impact on mother and baby in a maternity unit in North West London
G Gopal Rao, Bonilla Nayar, Adnan Aali, Anam Fayadh, Stephen Hiles
London North West University Healthcare NHS Trust
Background: In pregnant and postpartum women, GBS is an important cause of maternal sepsis, frequently resulting in maternal bacteraemia. There are few published studies that describe the clinical impact of GBS bacteraemia on the mother and the baby.
Aim: To describe the incidence of maternal GBS bacteraemia in a maternity unit in North West London and its clinical impact on the mother and baby.
Methods: Retrospective Observational Study of mothers who delivered at the Northwick Park Hospital and had pyrexia or sepsis and GBS bacteraemia and Babies born to mothers with GBS bacteraemia in the period January 2018- December 2020. Data were collected from the laboratory and maternity information management software. The following information was collected and analysed for the mother: Age, Gravida, Parity, Mode of delivery, length of hospital stay, outcome of infection. The following information was collected for the baby: Gestational age, birth weight, clinical signs of sepsis or foetal distress (pyrexia, cardiotocograph (CTG) abnormality, meconium staining) and clinical outcome.
Results: During the study period, there were 13400 deliveries. Twenty women had maternal GBS bacteraemia with incidence of 1.48/1000 deliveries Average age of bacteraemic mothers was 28 years (range 21–43 years); Average gravida 3 (range 1–13); parity 2 (range 1–6). Racial origins of the mothers were: Indian subcontinent (9); white ‘other’ (5); White British (2); Black (2) Unspecified (2). Mode of delivery of the baby was Caesarean section in 9 (8 emergency; 1 elective); Forceps delivery in 3; Vacuum (Kiwi) delivery in 2 and Spontaneous vaginal delivery in 6. The average length of hospital stay of mothers was 6 days (range 1–11 days). In accordance with hospital guidelines, all mothers were treated empirically with cefuroxime and metronidazole and then changed to benzyl penicillin or amoxicillin after detection of GBS bacteraemia. All mothers recovered and were discharged to their homes. The average weight of the babies was 3319.5 grams (range 2270–4065 grams) and gestational age was 39 weeks (range 37–41 weeks). 10 babies had abnormal CTG, 2 had meconium staining and 10 developed pyrexia. All babies recovered and were discharged alive.
Conclusion: This study shows that maternal GBS bacteraemia has a significant clinical impact both on the mother and the baby. In addition to morbidity due to sepsis, maternal GBS bacteraemia results in increased number of emergency caesarean sections and instrumental deliveries; increased length of hospital stay, antimicrobial treatment and foetal distress and pyrexia in the newborn.
Abstract ID: 6
Subcategory: Vaccines
The US Centers for Disease Control and Prevention-led study to establish immunologic endpoints associated with protection against infant invasive group B streptococcal disease: methodology and updates
J Rhodes, S Schrag, P Maniatis, Y Chung, L McGee, S Bolcen, W Xing
National Center for Immunization and Respiratory Diseases, Division of Bacterial Diseases, Centers for Disease Control and Prevention, Atlanta, GA, USA
Objective: Maternal group B streptococcal (GBS) vaccines to prevent young infant invasive GBS disease are in development and may be licensed based on immunologic endpoints. To help establish immunologic endpoints for infant GBS disease based on antibodies to the capsular polysaccharide, we are conducting a case-control study built on CDC’s Active Bacterial Core (ABCs) multistate surveillance.
Methods: Cases are defined as isolation of GBS from a normally sterile site in an infant aged <90 days. Controls are defined as infants without invasive GBS disease in the first 90 days of life born to mothers identified as GBS-colonized through antenatal GBS screening. Study specimens include case-associated GBS isolates and control-associated maternal GBS screening specimens for serotyping, as well as remnant newborn screening dried blood spots for measurement of serotype-specific capsular IgG antibody level and function via International GBS Assay Consortium endorsed assays.
Results: The study is in progress; 362 cases and 1336 controls are enrolled to date with a projection of greater than 500 cases and 2400 controls when enrollment of eligible participants is completed in 2021. Serotype is currently available for 258 cases; serotype III predominates at 52%, followed by Ia (14%); Ib (10%); II (9%); IV (8%); and V (7%). Among 216 controls with serotype results, serotype II is predominant (33%); followed by III (19%); V (18%); Ia (12%); Ib (11%) and IV (6%). CDC’s immunology laboratory has demonstrated proficiency with functional and binding assays and participated in the GBS Consortium-led inter-laboratory validation study. We will discuss anticipated timelines for interim and final study results.
Conclusion: ABCs provides access to a large series of invasive GBS infant cases. By leveraging this resource, along with a robust US newborn screening dried blood spot repository, this study has the potential to help establish reliable serotype-specific infant GBS immunologic endpoints for a US setting.
Abstract ID: 7
Subcategory: Epidemiology
GBS antenatal screening and recto-vaginal colonization rates before and during the COVID-19 pandemic
Daniela Menichini1,2, Maria Longo2, Francesca Miselli3, Luca Bedetti3, Francesca Monari2, Alberto Berardi3, Fabio Facchinetti2
1International Doctorate School in Clinical and Experimental Medicine, Department of Biomedical, Metabolic and Neural Sciences, University of Modena and Reggio Emilia, Italy; 2Obstetrics Unit, Mother Infant Department, University Hospital Policlinico of Modena, Modena; 3Neonatologic and Pediatic Department, University Hospital Policlinico of Modena, Modena, Italy
Background: The SARS-CoV-2 pandemic has resulted in the implementation of recommendations to reduce interpersonal contact. From March 2020, rules were applied also in Italian Obstetrics units. Recent data report reduced rates of nosocomial and surgical site infections during the pandemic period. We wonder whether measures for containment of SARS-CoV-2 transmission would affect Group B streptococcus (GBS) maternal recto-vaginal colonization rates, usually screened at 36–37 weeks’ gestation. The primary endpoint of this study was to evaluate the rate of maternal GBS colonization at antenatal screening.
Methods: This is a retrospective observational study (carried out in district of Modena), comparing maternal GBS colonization rates in the pre-COVID-19 (2018–2019) and during the pandemic period (2020–2021). Rates of recto-vaginal colonization were retrieved from the laboratory database. The total number of deliveries was collected. Data were analyzed by using the Chi-Squared test, also evaluating the adherence to the GBS screening. A p-value < 0.05 was considered significant.
Results: A total of 10968 and 10802 deliveries occurred in the pre-COVID-19 and the Pandemic period respectively (overall reduction in deliveries of 1.5%). The adherence to the antenatal GBS screening declined from 96.6% (pre-COVID-19 era) to 91.6% (pandemic era, p<0.001). Notably, the proportion of positive GBS screening remained stable (18.3% in 2018–2019 and 18.2% in 2020-2021, p=0.80).
Conclusion: During the SARS-CoV-2 pandemic, we reported a reduced adherence to antenatal GBS screening. SARS-CoV-2 containment measures adopted by both the population and hospital professionals did not affect GBS colonization rates.
Abstract ID: 8
Subcategory: Microbiology and testing
Group B Streptococcus surveillance among pregnant women in Rio de Janeiro, Brazil over a period of 14 years (2008–2021)
Nery, D. C. M¹, Botelho A. C. N.¹, Silva, L. M B1, Simões, L. C.1, Oliveira, L. M. A.1, Santos, M. L R.¹, Costa, N. S1, Alvim, D. S., Rocha, A., Marinho P², Joffre Amim Jr ², Fracalanzza, S. E. L.¹, Teixeira L. M¹, Pinto, T.C.A.¹
¹Instituto de Microbiologia, UFRJ, ²Maternidade Escola, UFRJ, Rio de Janeiro, Brazil
Introduction:Streptococcus agalactiae or Group B Streptococcus (GBS) is a major cause of neonatal disease worldwide. Although it might vary according to the country, about 20%–30% of pregnant women are colonized by GBS, representing a risk for mother and neonate health. Knowing regional GBS colonization rates and GBS characteristics are crucial to help design preventive and treatment measures for GBS diseases, but in Brazil these data are still largely unknown.
Objectives: The current work aimed to investigate GBS colonization among pregnant women in a public maternity in Rio de Janeiro, Brazil along a period of 14 years (2008–2021).Methods: Clinical and sociodemographic data were obtained via questionnaire, during the screening appointment, under informed consent. The local ethics research committee approved the project. Statistical analysis was performed with jamovi software (v. 2.2.5) by Pearson’s chi-squared test. Also, 303 GBS strains (25% of total) isolated along the period of study were randomly selected and characterized regarding capsular type by latex agglutination and antimicrobial susceptibility profile by disk-diffusion according to CLSI.
Results: From 5744 pregnant women screened, GBS was detected in 1216 (21.2% overall), but this rate varied along the years, ranging from 28.3% in 2014 to 6.0% in 2021. Sociodemographic data (age, ethnicity, place of birth) did not correlate with GBS colonization, but clinical data, including presence of vaginal discharge, history of previous neonatal death and presence of a maternal pathology, were significantly associated with GBS positivity (p<0.05). Within pathologies, diabetes (pre, gestational and mellitus) was the most common (59%) followed by arterial hypertension (25,6%) and correlated with GBS detection (p<0.05). Among GBS strains analyzed, serotype Ia was the most frequent (48.5%) and well distributed over the years, followed by II (18.2%) and V (16.8%). All strains were susceptible to penicillin, 88% were resistant to tetracycline, 4% to clindamycin and 14% to erythromycin; 1% were multidrug resistant. Although overall resistance rates were low, an upward trend in macrolide resistance was detected since 2015.
Conclusions: In general, our results add valuable information on GBS epidemiology in Rio de Janeiro, Brazil regarding clinical aspects and strain characteristics of GBS among pregnant women, which can serve as a basis for designing public health polices to prevent GBS neonatal disease.
Abstract ID: 9
Subcategory: Epidemiology
Brain lesions complicating Group B Streptococcus Early and Late-Onset Disease
1Pediatric Postgraduate School, University of Novara, Novara, 2Pediatric Postgraduate School, University of Modena and Reggio Emilia, Modena, 3Neonatal Intensive Care Unit, University Hospital of Modena, Modena, 4PhD Program in Clinical and Experimental Medicine, University of Modena and Reggio Emilia, Modena, 5Pediatric Emergency Unit, Scientific Institute for Research and Healthcare (IRCCS), Sant’Orsola Hospital, Bologna, 6Neonatal Intensive Care Unit, Infermi Hospital, Rimini, 7Department of Infectious Diseases, Istituto Superiore di Sanità, Rome, 8Neuroradiology Unit, Department of Neuroscience, Civil Hospital S. Agostino Estense, Modena, 9Pediatric Department, Hospital of Imola, Imola
Background: Group B streptococcus (GBS) is a leading cause of neonatal sepsis and meningitis. Characteristics of GBS-associated brain lesions are poorly defined1.
Intrapartum antibiotic prophylaxis (IAP) has substantially reduced the rates of early-onset disease (EOD; onset on day 0–6 postpartum), but does not prevent late-onset disease (LOD; onset on day 7–89 postpartum).
Methods: Our study is a retrospective multicentre, including 13 Italian centres.
Population included: infants born from 2006 to 2014, with GBS yielded from blood or cerebro-spinal fluid within 90 days of birth. We revaluated images of brain magnetic resonance imaging (MRI) within 6 months of infection.
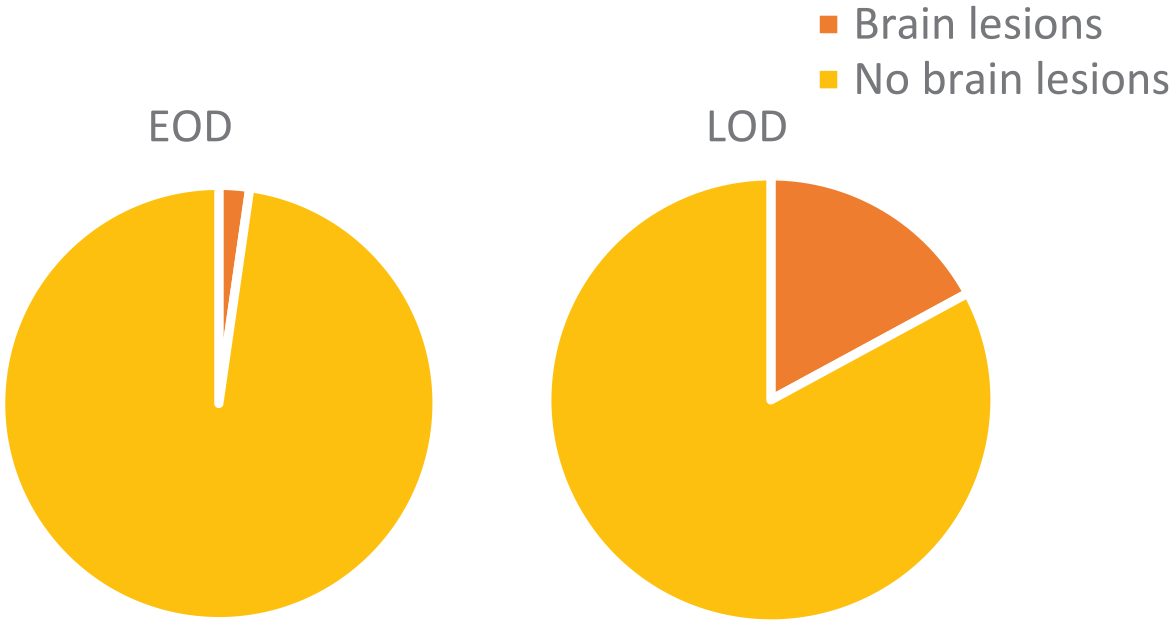
Results: 203 GBS neonatal infections were reported, of whom 34 received MRI within 6 months of infection. EOD and LOD were 5 (15%) and 29 (85%), respectively. Brain lesions were documented in 22 infants (65%): 16 were full-term and 6 were preterm. Brain lesions (Figure 1) were more likely in LOD (20 out of 117, 17%) compared to EOD (2 out of 86, 2%) (p<0.001).
Incidence of brain lesions in LOD compared to EOD.
Conclusions: This study provides Italian data on brain lesions complicating EOD and LOD in both preterm and full-term infants (Figure 2). Full-term infants: in order of frequency lesions affected mostly the cerebral cortex, cerebellum, and thalamus. Preterm infants: lesions frequently led to ventricular dilatation, and affected both the grey and white matter (periventricular leukomalacia). We found an increased risk of brain injuries in LOD compared to EOD (Figures 3) It is likely that this difference could be related to the prevention strategies for EOD, including widespread diffusion of IAP targeted to mothers colonized with GBS and/or risk factors2.
Type of brain lesions found in full-term and preterm infants.
Example of neuroimaging finding in LOD - Multifocal superficial cortical infarction, and ischemic infarction involving the right thalamus.