
Abstract
SARS-CoV-2 (severe acute respiratory syndrome coronavirus-2) infection is being one of the most significant challenges of health care systems worldwide. Bacterial and fungal infections in hospitalized patients with coronavirus disease 2019 (COVID-19) are uncommon but consumption of antibiotics and antifungals has increased dramatically during the ongoing pandemic resulting in increased selective pressure for global antimicrobial resistance. Nosocomial bacterial superinfections appear to be more frequent than community-acquired coinfections, particularly among patients admitted to the intensive care unit (ICU) and those receiving immunosuppressive treatment. Fungal infections associated with COVID-19 might be missed or misdiagnosed. Existing and new antimicrobial stewardship (AMS) programmes can be utilized directly in COVID-19 pandemic and are urgently needed to contain the high rates of misdiagnosis and antimicrobial prescription. The aim of this review is to describe the role of bacterial and fungal infections and possible strategies of AMS to use in daily practice for optimal management of COVID-19.
Keywords
Introduction
The coronavirus disease 2019 (COVID-19) pandemic is having a profound and devastating impact on global healthcare systems. Bacterial and fungal infections represent important complications of respiratory viral diseases and have been reported after COVID-19.1,2 Despite the infrequency of confirmed coinfection and secondary infections from early reports during the COVID-19 pandemic, consumption of antibiotics has increased dramatically and misuse of antimicrobials has resulted in increased selective pressure for global antimicrobial resistance (AMR).3,4 Overprescribing of antibiotics and antifungals in patients infected with SARS-CoV-2 has probably been the result of high morbidity and mortality of acute illness and the absence of significantly effective therapeutic options.5–9 Significant misconceptions about the use of pharmacological products for COVID-19 have been observed due to the initial uncertainty about therapeutic benefit and limited available data. 10 Moreover, COVID-19 has led to a fundamental reorganization of hospitals and ICUs, and increased workload for health care workers. Altogether, this new situation significantly impacted AMS efforts but the use of antimicrobial agents in the COVID-19 pandemic has highlighted the importance of upholding old and new AMS principles in daily practice. 9
The aim of this review is to understand the role of bacterial and fungal infections and patterns of antibiotic and antifungal use in patients with COVID-19, for optimal empirical management strategies and AMS programmes.
General stewardship principles
Since the 1970s, AMS has evolved to become a coherent set of actions designed to use antimicrobials responsibly, with the main current aim to combat AMR. AMS programmes have been shown to improve patient outcomes, to lower the rate of antibiotic adverse events (namely Clostridium difficile infection) and to decrease health system costs, the length of stay and readmission rates.11–13
AMS programmes can be persuasive (with educational programmes, prospective audits and feedback), restrictive (with restrictions on the use of antibiotics and pre-authorization requirements) or structural (with decision support systems and computerization of records). 14 AMS interventions may be vertical, as systemic interventions carried out by the facility, or horizontal, as punctual interventions for a specific antimicrobial or infection.15,16 AMS programmes involve several personnel including administrative leadership, infectious disease physicians, pharmacists, nurses, microbiologists, pharmacologists, allergists, laboratory staff, public health specialists and information technology programmers, aiming as a whole to prescribe the right antibiotic in terms of antibiotic choice, pharmacokinetic/pharmacodynamic parameters, dosage, route of administration, treatment duration, patient compliance, allergy history, local epidemiology and cost-effectiveness. The best antibiotic may be no antibiotic at all if not needed.17,18 A crucial step is diagnostic AMS, which is based on adequate sampling strategies that precede antibiotic prescription and requires the competence to correctly order and interpret the result of the test.19,20 Non-pharmacological interventions such as the withdrawal of the central venous catheter must also be considered as additional actions (Table 1).
AMS intervention in the pre- and post-COVID-19 pandemic eras.

IV, intravenous; MDR, multidrug-resistant; RSV, respiratory syncytial virus; SARS-COV-2, severe acute respiratory syndrome coronavirus 2.
Once the programme has been implemented, a continuous quality improvement strategy is essential through meetings among the AMS staff to monitor indicators of effectiveness and adverse events, to manage interventions and to update local guidelines with microbiology cumulative susceptibility reports, pharmacy reports and new molecules. 21 Electronic health records are of great support. 22
AMS can be applied to the management of community-acquired pneumonia (CAP) to optimize treatment while maintaining or improving the quality of patient outcomes. 23 AMS programmes for CAP have been shown to reduce intravenous therapy, the length of antibiotic therapy and hospital stay, and expenditure on antibiotics and to be long-lasting.24,25 AMS interventions for CAP include differentiating viral from bacterial aetiologies, performing an adequate diagnostic work-up, an early switch to oral antibiotics and short therapy. A recent meta-analysis showed that 24.5% of CAP have a viral aetiology and molecular testing for virus and atypical pathogens has been demonstrated to reduce the use of intravenous antibiotics.5,26,27 Procalcitonin (PCT) has been successfully used to guide antibiotic treatment, reducing antibiotic use and exposure in all clinical settings and lowering mortality in critical patients, especially when embedded into a clinical algorithm.28,29 A methicillin-resistant Staphylococcus aureus nasal swab can be useful in de-escalating therapy due to its high negative predictive value.30,31
Of note is that in recent years, concerns on the emergence of antifungal resistance and inappropriateness of antifungal prescription have motivated the development of antifungal stewardship (AFS) programmes. Many AFS programmes designed in tertiary centres have succeeded in reducing mortality32–34 improving the appropriateness of antifungal use and decreasing the economic burden of new antifungals35,36 with the additional support of fungal biomarkers.37,38 AMS has been shown to reduce the use of antifungals by increasing prescribers’ awareness and mitigating risk factors for fungal infections.39,40
Problems of AMS in daily practice in COVID-19 and possible solutions
AMS is urgently needed to contain the high rates of antimicrobial prescription described, reversing the downward trend resulting from AMS practices.41–43 The increase in patient density in wards and the generous amount of broad-spectrum antibiotics given will possibly lead to an increase in AMR in the next years, and it might result in a pandemic due to multidrug-resistant (MDR) organisms. 44
In critically ill patients and in the context of the current COVID-19 pandemic, the benefits of AMS practices may be overlooked. An increase up to 35% of blood cultures collection has been described but with a low prevalence of bloodstream infections and high rate of blood culture contamination due to a decrease in diagnostic stewardship adherence.45–47 The prolonged use of personal protective equipment, in combination with a low adherence to infection control practices, has been shown to increase the contamination from enteric microorganisms. 48 Tiri et al. 49 showed that prone positioning in the intensive care unit (ICU), a manoeuvre requiring several healthcare workers, in addition to the use of protective personal equipment for many hours and to the presence of new staff untrained to AMS and infection control techniques, increased carbapenem-resistant Enterobacterales acquisition from 6.7% to 50%. In the pandemic period, where all energies are mainly focused on COVID-19 hospitals, policy makers should make an effort to fund AMS programmes in an attempt to contain the spread of MDR organisms and to support the decision-making of clinical staff. 50
AMS programmes, already understaffed in many countries in the pre-pandemic era, are now dealing with the diversion to COVID-19 patients and the difficulty of keeping pace with routine AMS topics. Funding from AMS programmes may be redirected to the needs of the pandemic. Face-to-face meetings are discouraged or hard to fit into the full working days of the pandemic. AMS programmes that quickly adapted to the pandemic context have proven to be able to reduce antibiotic prescription and the duration of therapy through modified protocols and the aid of computer systems and of non-clinical figures such as pharmacists.51–53 Solutions to new challenges offered by the pandemic, especially the extensive use of technology and web-based strategies (app software, emails and videoconferencing) may continue even in the post-pandemic period to improve AMS services. 54 An Italian survey showed that non-infectious disease specialists tend to prescribe more antibiotics, possibly due to a lack of knowledge of AMS principles. This should prompt the expansion of web-based educational programmes to all specialists due to the fact that many non-infectious disease specialists are involved in the management of COVID-19 patients. 55 Finally, AMS experts advocate for the development of updated local and national recommendations during the pandemic to standardize procedures from patient admission to the emergency room to discharge through the potential ICU stay (Tables 1 and 2).10,56
Possible AMS solutions for COVID-19 patients.

BAL, bronchoalveolar lavage; CAPA, COVID-19-associated pulmonary aspergillosis; CT, computed tomography; MDR, multidrug-resistant.
According to the criteria mentioned in local and national guidelines for CAP.
Misconceptions of agents use in COVID-19
Many drugs with known or putative antibacterial (azithromycin), antiviral
The epidemiology of bacterial infections in COVID-19
Bacterial coinfection are defined as bacterial infections that occur on presentation (⩽48–72 h after admission) whereas bacterial secondary infections or superinfections as bacterial infections that emerge during the course of illness or hospital stay (>48–72 h after admission) and are synonymous with nosocomial or hospital-acquired infection. Bacterial coinfections and superinfections are commonly identified in severe respiratory viral infections, mostly commonly in influenza in which they are a major cause of morbidity and mortality. 58 However, the overall number of coinfections/superinfections is lower in patients with COVID-19, and the associated pathogens differ from that reported in influenza and other coronaviruses.59–62 Most studies to date have been retrospective with small sample cohorts and have very limited microbiological and clinical detail and data on the presence of bacterial infections other than pneumonia.3,63,64
A systematic review and meta-analysis of 31 studies (> 6000 patients) reported a low prevalence of confirmed bacterial infection (8.6%, 95% CI 4.7–15.2%), with a higher prevalence of secondary infections (16.0%, 12.4–19.6%) than coinfections (4.9%, 2.6–7.1%).3,63,64 Most findings of this meta-analysis were confirmed by a recent prospective multicentre cohort study from the United Kingdom on 48,902 patients admitted to hospital with COVID-19 during the first wave. Overall, they found that microbiologically confirmed bacterial infections were infrequent (1107/8649: 12.7%), coinfections at hospital admission were rare and when infections were identified, most were secondary, especially in severely ill patients. 60
A recent multicentre study on critically ill patients with COVID-19 showed a high risk of hospital-acquired infections (46%, 359/774), in particular ventilator-associated pneumonia (VAP) (50%) and bloodstream infections (34%). Of note is that approximately one-third of all the infectious episodes were due to MDR organisms (35%). 65 In addition, it is reported that, despite 68% of patients receiving antibiotics at the time of ICU admission, after a routine diagnostic work-up, a documented secondary infection was observed in only 1% of subjects. These findings suggest that antibiotic therapy could be withheld with limited risks in a considerable fraction of patients with COVID-19, even when severely ill, if recently hospitalized and without septic shock or evidence of coinfection.10,66
Focusing on microbiological aetiology, Streptococcus pneumoniae, Staphylococcus aureus and Haemophilus influenzae have been described as the most common pathogens causing respiratory coinfections, with Enterobacterales, Pseudomonas aeruginosa and S. aureus as the most common in hospital-acquired respiratory superinfections. 60
A recent study on a large multinational cohort of 684 oncological and haematological cancer patients with COVID-19 found that coinfections were higher than in the general population (7.8%) and superinfections were documented in a similar proportion to that in the general population (19.1%), affecting mainly neutropaenic patients with high levels of C-reactive protein and ICU admission. In this cohort, lower respiratory tract infections were the most frequent infectious complications, most often caused by S. pneumoniae and P. aeruginosa, and only seven patients developed opportunistic infections. 67
Although azithromycin has been extensively used, large retrospective studies have shown a low incidence of atypical pathogen superinfections.6,68
Coinfection and secondary infection have shown variable inpatient mortality among patients admitted to hospital and to ICU.60,69 However, coinfection and secondary infection have been associated with significantly severe disease and poor outcomes in patients complicated by septic shock and those who are immunocompromised.60,67
Antibiotic utilization in COVID-19 patients
The frequency and nature of antimicrobial use are concerning, since 75–85% of COVID-19 patients have been shown to receive one or more antimicrobials at some point during their hospital admission. The highest rates of prescription have been described in the ICU setting, especially for patients requiring mechanical ventilation and for older patients.3,60,63,70
Studies infrequently report the drug classes used, and prescribing has been observed to be very heterogeneous depending on geographical area. A recent systematic review found that, overall, the most common antibiotic classes prescribed were fluoroquinolones (20.0%), macrolides (18.9%), β-lactam/β-lactamase inhibitors (15.0%) and cephalosporins (15.0%). 63 Russell et al. 60 described frequent use of broad-spectrum agents for empirical therapy (β-lactam–β-lactamase inhibitors) for lower respiratory tract infections, empirical escalation from piperacillin–tazobactam to carbapenems in the ICU, and preferential use of carbapenems rather than carbapenem-sparing alternatives has been identified.
Improving AMS of bacterial infections in patients with COVID-19
Aetiological confirmation remains a diagnostic problem in CAP, especially in the context of COVID-19 there is no well-established list of pathogens. Diagnosis of bacterial coinfections or superinfections should always be pursued with adequate respiratory sampling from the admission of the patient prior to the initiation of antimicrobial therapy. In case of blurred clinical presentations, international protocols recommend testing other aetiologies according to local guidelines. 71 Low rates of microbiological sampling in patients with COVID-19 have been reported (around 20%), lower than those reported for CAP. 60 This may be the result of overwork due to the pandemic and concerns regarding healthcare worker safety, especially for aerosol-generating procedures such as bronchoalveolar lavage (BAL), despite recent evidence supporting the fact that it can be safely carried out in COVID-19 patients. 72 Moreover, low rates of aetiological confirmation might be due to receiving antimicrobials before sampling, decreasing the yield of bacterial cultures and the lack of sensitivity of conventional culture-based methods.
Molecular-based bacterial diagnosis is associated with greater detection of pathogens than culture-based methods but new molecular technology is far from being utilized universally as of this writing. Moreover, in patients with a positive bacterial culture or molecular result from respiratory material, most studies do not report how this result is related to a clinically or otherwise confirmed diagnosis of bacterial coinfection. 73
The infrequency of confirmed coinfection and timing supports restrictive empirical antimicrobial usage, especially at hospital admission. 60 Current international guidelines recommend against the routine use of antibiotics, unless there is a high level of clinical suspicion, and vary in their recommendations on empirical antimicrobial therapy, since some recommend empirical antimicrobial therapy in severe disease, whereas others do not.71,74
Distinguishing severe viral pneumonia from bacterial coinfection and secondary infection upon admission and during hospitalization is challenging. 53 Although clinical criteria alone may be the mainstay of the decision, clinicians should always assess the risk of a bacterial infection in patients with COVID-19, based on a combination of the clinical course of the disease and results obtained from laboratory tests and imaging.75,76
Incorporating trends in inflammatory markers into decision-making could support judicious use of antimicrobials. Raised inflammatory biomarkers are the hallmark of the inflammatory phase of COVID-19, and starting an antibiotic therapy should be carefully considered.77,78 The absence of an elevated white cell count at baseline and antimicrobial-associated C-reactive protein (CRP) and procalcitonin (PCT) (threshold ⩽ 0.25 ng/ml) might be an additional decision-making adjunct to exclude coinfection.77,79 However, the evidence base for such a strategy is currently limited, and the dynamic trajectories of PCT, CRP and neutrophil may show a downwards trend after tocilizumab or steroid treatment. 80 In addition, the radiographical features of bacterial infections (lobar consolidation, air bronchogram) could be useful to assist the diagnosis.
Antimicrobials should be restricted to (1) individuals with severe–critical respiratory disease, or (2) tailored to patients with atypical features of COVID-19 (clinical presentation or radiological imaging suggestive of bacterial infection) and (3) severely immunocompromised patients (use of chemotherapy for cancer, bone marrow or organ transplantation, immune deficiencies, poorly controlled HIV or AIDS, or prolonged use of corticosteroids or other immunosuppressive medications) and (4) confirmation of evidence of respiratory or distinct non-respiratory coinfection. 81
Diagnostic microbiological work-up should always be performed at hospital admission before starting empirical antimicrobial treatment, including at least blood and sputum cultures as well as S. pneumoniae urinary antigen to support or refute the diagnosis of bacterial coinfection. Legionella urinary antigen testing should be performed according to the criteria mentioned in local and national guidelines for CAP.
If empiric antibiotic treatment is administered for suspected coinfections, the choice of antimicrobial should be tailored to likely pathogens and resistance patterns based on local and national guidelines for the treatment of CAP, but routine empirical treatment of atypical pathogens is not suggested. In COVID-19 patients with suspected secondary bacterial infections, including hospital-acquired pneumonia (HAP) and VAP, it is recommended to start empirical treatment after obtaining cultures, based on previous patient microbiological history, risk of MDR, immunocompetence level and local epidemiological data and in line with local recommendations on antibacterial treatment.42,50,82
When antimicrobials are started, patients should be re-evaluated daily to promptly de-escalate or stop antibiotics if there is no evidence of bacterial infection; when antimicrobials are required, treatment duration should be limited to 5–7 days if lower respiratory tract infection is suspected, upon improvement of signs, symptoms and inflammatory markers.77,83,84
The epidemiology of invasive fungal infection in COVID-19
Invasive fungal infections (IFI) are usually acquired nosocomially and in the ICU setting, with a higher risk of community-acquired IFI, especially from moulds, in the immunocompromised patients. In patients at advanced stages of COVID-19, in which nosocomial risk factors add up to immunoparalysis, IFI have been reported. The epidemiology of invasive fungal infections (IFI) in critically ill, mechanically ventilated COVID-19 patients has been recently described in a comprehensive multicentre prospective cohort study performed in the United Kingdom. 85 In this study, the overall incidence of IFI was 26.7%, with COVID-19-associated pulmonary aspergillosis (CAPA) accounting for the bulk of IFI (14.1%), followed by yeast infection in 12.6% of the cases. 85
Regarding invasive candidiasis, several studies have reported variable incidence rates ranging from 0.4% to 12.6% of COVID-19 cases.59,64,65,70,86–89 Patients usually develop invasive candidiasis late in the course of their hospitalization (on average, > 7 days after hospital admission), 70 with many of them showing common factors associated with either invasive candidiasis or severe COVID-19 (e.g. broad-spectrum antibiotics, diabetes, older age, central venous catheter and corticosteroid therapy).63,90
As for CAPA incidence, it varies extensively among the published literature, ranging from 2% to 34%.91–99 Reasons that may contribute to the wide variability in incidence rates include (1) differences in the diagnostic criteria applied,91–100 (2) a lack of sensitivity of blood tests 101 and (3) discrepancies in sampling of the primary site of the infection. Overall, most patients developed CAPA on average between Day 4 and Day 11 after ICU admission. 102 However, clinicians should be aware that in the only study involving routine bronchoscopy, up to 13% of the patients showed a positive galactomannan (GM) result (GM index > 1) in fluid at the time of ICU admission. 100
As we are now gathering more data regarding fungal superinfections in COVID-19 patients, less frequent opportunistic fungal pathogens are increasingly reported, including Mucorales, Histoplasma spp., Cryptococcus spp. and Pneumocystis jirovecii. 103 Regarding mucormycosis, although it is a rare fungal infection, there have been about 15,000 cases reported among COVID-19 patients as of 28 May 2021 in India, 104 where the prevalence of the disease is 80 times higher than in the rest of the world. 105 The possible reasons for the high prevalence is the abundant presence of Mucorales in the community and hospital environment, the improper use of steroid therapy to treat COVID-19 patients, the large number of susceptible hosts (especially diabetics with late diagnosis or underdiagnosed obese patients) and the possible improper use or contamination of oxygen or nebulizer devices. 106
Antifungal utilization in COVID-19 patients
While awareness regarding IFI in patients with COVID-19 has increased, there are few reliable and systematically reported data on antifungal consumption in COVID-19 patients.107,108 In terms of benchmarking data, a single-centre study at Virginia Commonwealth University Hospital (865 beds) found no significant increase in the overall number of days of therapy per 1000 patient days for either April 2020 or May 2020 when compared to April 2019–March 2020. 107 In another study consisting of a point-prevalence survey of prescribing treatment across acute hospitals in Scotland, systemic antifungals were prescribed in about one in ten critically ill patients (12/122), and in half of cases, therapy was considered as targeted treatment. 108
Although gathering baseline data is of paramount importance for defining prescribing trends and identifying areas of improvement, 109 none of the aforementioned studies assessed the prescribing quality of antifungals in terms of indications, dosage or length of treatment. 36 Accordingly, it is not possible to evaluate what proportion of COVID-19 patients have been given antifungal treatment deemed unnecessary.
Improving AFS of fungal infections in patients with COVID-19
An area of great interest in terms of AFS is represented by CAPA, as it has been associated with a mortality rate of up to 90%. 85 Because diagnosis of CAPA is a challenge, we suggest maintaining a high index of suspicion in order to reach an accurate diagnosis. 110 In our opinion, CAPA should be always suspected and ruled out in patients with (1) refractory fever for more than 3 days despite appropriate antibiotic therapy and in the absence of any other plausible causes; (2) worsening respiratory status; (3) chest pain, haemoptysis or pleural friction rub; and (4) nodules or cavitation in chest computed tomography (CT). 111 The recommendation to perform bronchoscopy with fungal cultures and non-culture-based methods would apply even if a positive culture result might have been achieved accidentally or if other agents had already been isolated but clinical suspicion remains high. 110
Classic risk factors for invasive pulmonary aspergillosis (IPA) include prolonged neutropaenia, receipt of high doses of corticosteroids and impaired cellular immunity.110,112,113 However, several case series of patients with CAPA indicate that most COVID-19 patients have no traditional predisposing host factors for developing IPA.88,91,111 It is still unclear if SARS-CoV-2 infection itself represents the main risk factor for developing CAPA or whether additional predisposing conditions, such as intubation, older age, corticosteroids or treatment with IL-6 antagonist receptor further increase the risk for disease progression.111,114 In the study by Bartoletti et al., corticosteroid treatment was more common in patients with CAPA and corticosteroid use was more frequently associated with in-hospital mortality. 100
Further complicating the diagnosis of CAPA is the hesitancy in performing diagnostic bronchoscopy with BAL, as it requires prolonged patient contact, with a theoretical increase in aerosol exposure of healthcare workers.115,116 However, because bronchoscopy is of paramount importance in disease work-up for IPA and because recent evidence supports the fact that it can be safely carried out in COVID-19 patients, 72 we suggest performing lower respiratory tract sampling whenever a clinical suspicion of CAPA exists. In this sense, mycological diagnosis usually relies on the detection of GM from BAL fluid, with the likelihood of the infection increasing if serum circulating GM is also detected. 100 However, the diagnostic yields of serum GM in CAPA are very low, with a sensitivity of only 20–50%, that significantly decreases its value for ruling out the disease in daily clinical practice. 102 Due to the restricted availability of BAL, alternative specimens have also been proposed including sputum, bronchial aspirates and tracheal aspirates. 102 However, these specimens lack validation of Aspergillus biomarkers.
Another test that may be applied is the (1,3)-β-D-glucan; while it is more sensitive than GM, its specificity is limited by the fact that (1,3)-β-d-glucan is a polysaccharide component of the cell wall of many pathogenic fungi other than Mucorales and Cryptococcus.102,110 Performance of Aspergillus molecular testing for the diagnosis of CAPA is yet unknown. 102
Another major difficulty regarding CAPA diagnosis is the specificity of CT patterns as many signs of COVID-19 pneumonia can mimic those of CAPA and vice versa and many lesions, suggesting CAPA may be hidden. As suggested by recent consensus criteria for CAPA diagnosis, 72 the evidence of multiple pulmonary nodules or lung cavitation should prompt a thorough investigation for IPA as they are rarely observed in patients with COVID-19 alone. 85 Moreover, CT may continue to identify other reasons for respiratory deterioration. 102
Considering the inherent difficulties in diagnosing CAPA, an expert panel recently published a consensus definition that defined CAPA as IPA in temporal proximity to a preceding SARS-CoV-2 infection (positive real-time PCR for SARS-CoV-2 any time during 2 weeks between hospital admission and ICU admission). 111 In particular, the consensus proposed three different grades, categorizing patients as possible, probable or proven CAPA 111 (Table 3).
Proposed case definition for CAPA (adapted from Kohler et al.). 97
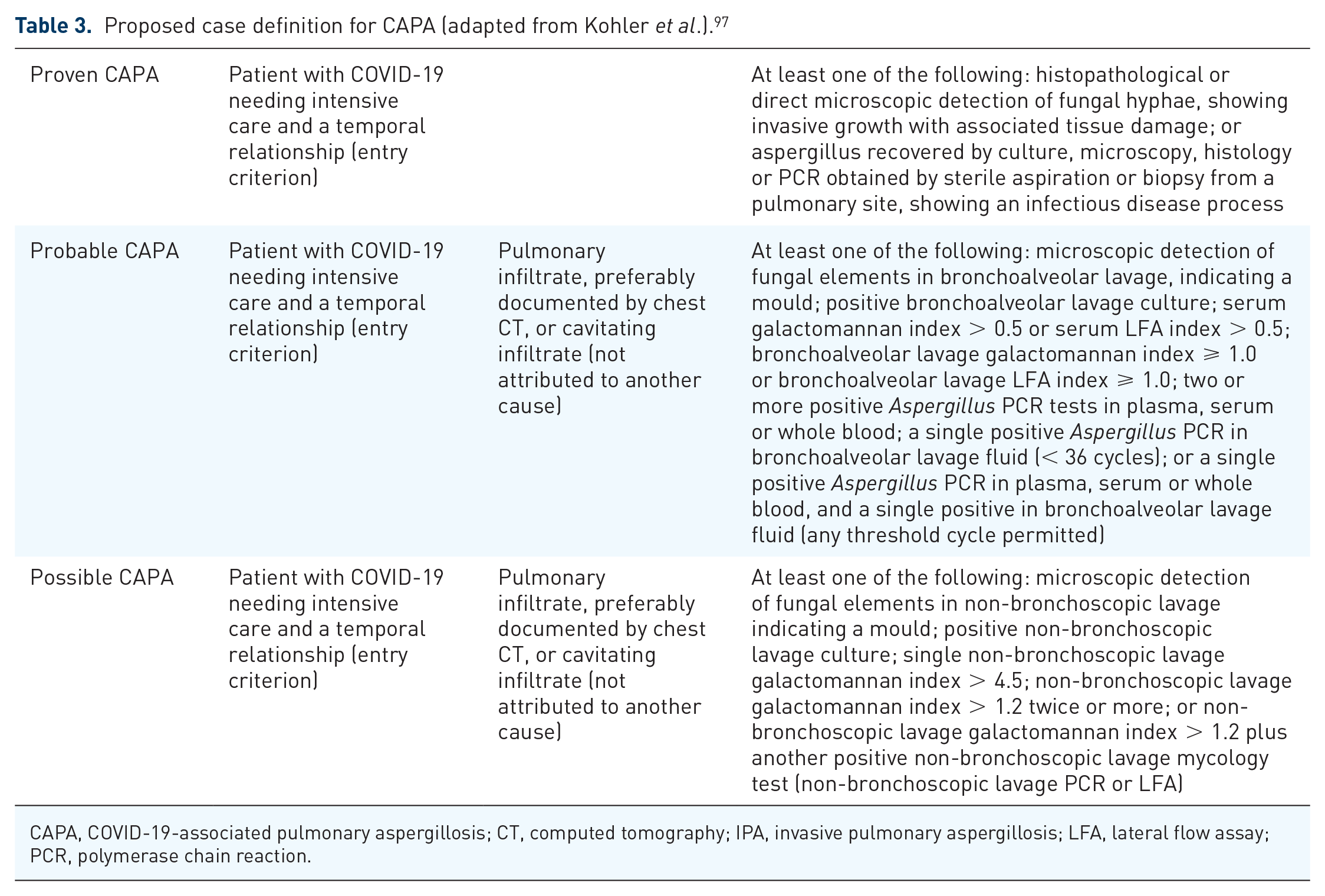
CAPA, COVID-19-associated pulmonary aspergillosis; CT, computed tomography; IPA, invasive pulmonary aspergillosis; LFA, lateral flow assay; PCR, polymerase chain reaction.
As for treatment, voriconazole currently represents the first-line treatment for IPA.102,110,111 However, there are many drawbacks associated with voriconazole treatment including major drug–drug interactions, 109 the requirement for therapeutic drug monitoring 117 and the limited spectrum of activity. Although there are few data outside the haematological setting, isavuconazole goes beyond these limits, offering a wider spectrum of antifungal activity than voriconazole, fewer toxicities and fewer drug–drug interactions as well as a lack of cyclodextrin, which is a solubilizing agent used in some other azoles (e.g. voriconazole), that can accumulate in renal failure after intravenous administration and potentially cause nephrotoxicity. 118 Finally, clinicians should be aware that case reports of azole-resistant CAPA are progressively being published.98,119 In this circumstance, treating CAPA patients with liposomal amphotericin B might be a reasonable alternative.118,120,121
Conclusion and future perspective
As the global pandemic continues, there is an urgent need to characterize bacterial and fungal infections in patients admitted to hospital with COVID-19 to determine optimal empirical antimicrobial management strategies and identify targets for AMS to prevent the vicious circle of antibiotic misuse, with deleterious consequences on individual patients and global ecology. Research priorities for strengthening AMS in COVID-19 include identification of the pathophysiological pathway of disease in the different phases, the description of infection biomarker dynamics and the role of imaging in COVID-19 patients with and without superinfection and investigation of the impact of rapid molecular tests for bacterial, fungal and viral coinfection.
Footnotes
Ethics approval and consent to participate
Ethics approval was not required as this is a narrative review.
Author contribution(s)
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Availability of data and materials
Data supporting the reveiw are in the published articles of the bibliograpy