
Abstract
Background:
Serratia is an opportunistic pathogen known to cause an array of infectious presentations. Aside from case reports, intravenous (IV) drug use has not been adequately quantified as a major risk factor for Serratia infection.
Methods:
A retrospective cohort study of 103 adult patients admitted to four community hospitals in Ohio from January 2014 to December 2018 with a positive blood culture for Serratia species. A complete data set of 103 patients was analyzed for demographics, comorbidities, initial diagnosis, treatment, and outcomes. Outcomes were recurrence of infection, in hospital mortality, 90-day mortality, length of hospital stay (LOS), complications (endocarditis, osteomyelitis, abscess), and evaluation for resistance to third-generation cephalosporins and extended-spectrum beta-lactamase (ESBL) activity. Descriptive statistics were performed using frequencies for discrete variables and median [interquartile range (IQR)] for continuous variables.
Results:
Serratia marcescens was the predominate species 94 (91%). Demographics were White 88 (85%) and male 63 (62%); 42 (42%) were IV drug users. IV drug users were younger than non-IV drug users with a median (IQR) age of 40 [33–50] versus 71 years [41–72] and likely to have hepatitis C virus (HCV) infection 37 (88%) versus 3 (5%), p < 0.0001. Culture and susceptibility analysis revealed 36% of isolates with possible or confirmed ESBL production. The most common complications were endocarditis (12%) and osteomyelitis (10%). In-hospital mortality was 2%, 90-day mortality (2%), with 90-day readmission (21%). The median (IQR) LOS is 7 [3.25–14.75].
Conclusion:
This is the largest study to our knowledge evaluating non-nosocomial Serratia bacteremia. Our study shows that a high proportion of patients hospitalized with a positive Serratia culture are IV drug users and have HCV co-infection. There is significant ceftriaxone resistance and ESBL activity noted in our population. Based on this, we suggest empiric treatment with cefepime or consider carbapenem therapy for Serratia bloodstream isolates pending full susceptibility data. Focus should be on proper antibiotic treatment as the readmission rate and LOS are high.
Background
Serratia species are opportunistic pathogens and are classified as facultative anaerobic oxidase-negative, non-lactose fermenting, gram-negative bacilli of the Enterobacteriaceae family. 1 Initially thought to be non-pathogenic, the US government released S. marcescens over both civilian and military areas from 1940 to 1960 with the goal of gathering data on the potential spread of bioterrorism agents. This was due to strains of S. marcescens having red pigment. These experiments, unearthed by investigative journalism in the 1970s, prompted a congressional investigation that studied US government testing on the public. 2
Since then, we have come to know of at least 20 species of Serratia, 8 of which are known to cause infection in humans. The primary pathogen is S. marcescens. Although Serratia is not part of the human normal flora, it is found in common environments, including water, soil, plants, and animals. They are known to cause an array of infectious presentations including urinary tract infections (UTIs), pneumonia, wound infections, soft tissue infections, surgical site infections, and although considered rare, endocarditis and bacteremia. 3
There have been over 200 reported hospital-based outbreaks of Serratia; however, hospital onset infections due to Serratia that occur outside of an outbreak scenario are documented as infrequent. 2 European surveillance data put Serratia as the primary pathogen in less than 3.3% of bacteremia cases and 5.4% of pneumonia cases. 4 Data from North and Latin America have numbers even lower with bacteremia cases at 1.6% and pneumonias between 2% and 4%. 5 Given the infrequent number of infections caused by Serratia outside of an outbreak, it is recommended that any cluster of Serratia occurring within the health care setting be evaluated for possible common source outbreak. 6
There are publications that establish a link between Serratia infections causing infective endocarditis and intravenous (IV) drug use. The link is highlighted in two reports published in 1976 and 1980 describing clusters of infective endocarditis due to S. marcescens within the San Francisco Bay Area. They describe a cluster of infective endocarditis due to S. marcescens in 36 cases, 89% with a history of IV drug use. 7 However, from 1980 to 2016, only 20 case reports of Serratia endocarditis have been reported in the literature. All these patients had chronic medical conditions or cardiovascular abnormalities and only three cases were associated with IV drug use. There are two isolated case reports since 2016, both of endocarditis in patients with a history of IV drug use. 8
Only about 0.14% of endocarditis cases are suspected to be caused by Serratia species according to one study based on observations from the International Collaboration on Infective Endocarditis Prospective Cohort Study database. 9 As the previous reports in the literature have contradicting findings surrounding the link between IV drug use and Serratia endocarditis, our study attempts to examine the degree at which IV drug use is associated with Serratia blood stream infections in our hospitalized patient population and evaluate outcomes associated with the infection.
Methods
This is a retrospective cohort study of all adult patients with positive blood cultures for Serratia species during the timeframe of January 2014 to December 2018 and hospitalized within the TriHealth organization hospitals in Cincinnati, Ohio, including Good Samaritan, Bethesda North, Bethesda Butler, and McCullough Hyde Hospitals. TriHealth laboratory provided the list of patients with positive blood cultures for Serratia.
Manual chart review provided patient demographics, comorbidities, initial diagnosis, treatment, and outcomes. Outcomes were recurrence of infection, in-hospital mortality, 90-day mortality, length of hospital stay (LOS), complications (endocarditis, osteomyelitis, abscess) and evaluation for extended-spectrum beta-lactamase (ESBL) activity, and resistance to third-generation cephalosporins (ceftriaxone).
Serratia was initially detected in the laboratory through incubated blood cultures on the Biomerieux BacT Alert System. After detection of growth, an aliquot was sent to Preferred Lab Partners and plated for colony growth. Once a culture was grown, it was identified via matrix-assisted laser desorption/ionization – time of flight (MALDI-TOF). The susceptibilities of the isolates were determined through Microscan AST MIC pre-made 96 well panels. Definitions of ‘confirmed’ ESBL production is based on wells at concentrations designed to detect a threefold dilution difference (confirmatory for ESBL production). When the detected growth falls outside of those dilution and cannot be determined, we consider this a ‘possible’ ESBL. There was no specific testing for AmpC.
Statistical analysis performed using descriptive statistics such as percentages, means, standard deviations, and difference in groups was obtained through chi-square, student t-test. Analysis was conducted using Statistical Package for the Social Sciences (SPSS) version 22.
Results
Population characteristics
In all, 103 patients were infected with Serratia during the 5-year timeframe evaluated by our study. Patients admitted with a positive Serratia culture were 40 (38%) females with a median interquartile range (IQR) age of 57 years [41–72]. The predominant ethnicity was Caucasian 88 (85%), African American 12 (12%), and Other/Unspecified 3 (3%) (Table 1). The predominant comorbid conditions include IV drug use 42 (42%), hepatitis C virus (HCV) infection 40 (39.6%), diabetes mellitus 26 (25.2%), immunosuppression 20 (20%), chronic kidney disease 13 (12.6%), and surgical procedure within the last 30 days 13 (13%) (Table 1). IV drug users infected with Serratia were significantly younger than non-IV drug users with a median (IQR) age of 40 [33–50] versus 71 years [41–72] and more likely to have HCV infection 37 (88%) versus 3 (5%) (p < 0.0001) and less likely to have chronic comorbidities such as diabetes mellitus 4 (9.5%) versus 22 (36%) (p = 0.002), chronic obstructive pulmonary disease 1 (2%) versus 9 (15%) (p = 0.035), immunosuppression 1 (2%) versus 19 (31%) (p < 0.0001), and surgical procedures within the last 30 days 0 (0%) versus 13 (21%) (p = 0.001) (Table 1). Most patients were living at home 79 (77%) or in long-term care facility or hospital 20 (19%) (Table 1).
Patient characteristics on admission.

GU, genitourinary tract; IQR, interquartile range.
n = 101.
Culture results
The overwhelming majority 94 (91%) of the patients were infected with S. marcescens (Table 2). Other Serratia species identified included S. plymuthica 4(4%), S. liquefaciens 3 (3%), S. odorifera 2 (2%) (Table 2). A total of 103 isolates from 103 patients were obtained and analyzed. Analysis of cultures were for the possibility of ESBL activity and confirmed resistance to third-generation cephalosporin (ceftriaxone) activity. Eleven (11%) of the specimens were confirmed positive with 26 (25%) identified as having possible ESBL activity. Fifteen (15%) had confirmed resistance to third-generation cephalosporins (ceftriaxone). Nine (8.7%) of positive Serratia blood cultures were positive for other organisms as well as Serratia. Other organisms present included Enterbacter cloacae 2 (1.942%), Escherichia Coli 2 (1.942%), Enterococcus faecalis 2 (1.942%), Methicillin-resistant Staphylococcus aureus (MRSA) 2 (1.942%), and Streptococcus anginosus 1 (0.970%). There were no positive blood cultures for more than two organisms present. The incidence of the presence of other bacteria as well as Serratia spp. was higher in IV drug users 7 (17%) versus 2 (3%) (p = 0.023) (Table 2). In all, 98 of the 103 cases (95%) were treated with antibiotics at admission (Table 2).
Blood cultures in patients hospitalized with Serratia bacteremia.

ESBL, extended-spectrum beta-lactamase.
Contamination
The identified sources of contamination were evaluated, and the most common source was indwelling catheter 32 (31%), skin and soft tissue 15 (15%), and urine 14 (14%). In 61 (59%) patients who were non-IV drug users, the most frequent source of contamination was indwelling catheters 29 (47.5%) versus 3 (7%) (p < 0.001) and urine 13 (21%) versus 1 (2%) (p = 0.006). In those with a history of IV drug use, the presumed cause of contamination was direct inoculation which included 42 (40%) (Table 1).
Complications in hospitalized patients with Serratia
Complications defined as endocarditis, osteomyelitis, septic emboli, and epidural abscess occurred in 24 (24%) cases. The most common complication was endocarditis alone in 7 (7%) patients, and osteomyelitis alone in 5 (5%), septic emboli in 3 (3%), and epidural abscesses in 2 (2%) patients. Seven (7%) patients had multiple complications (Figure 1). There was a significantly higher number of patients with complications among the IV drug users, 22 (52%) versus 5 (8%) (p < 0.0001), and additional bacteremia was found in 7 (17%) IV drug users versus 1 (2%) in non-users (p = 0.018) (Figure 2).
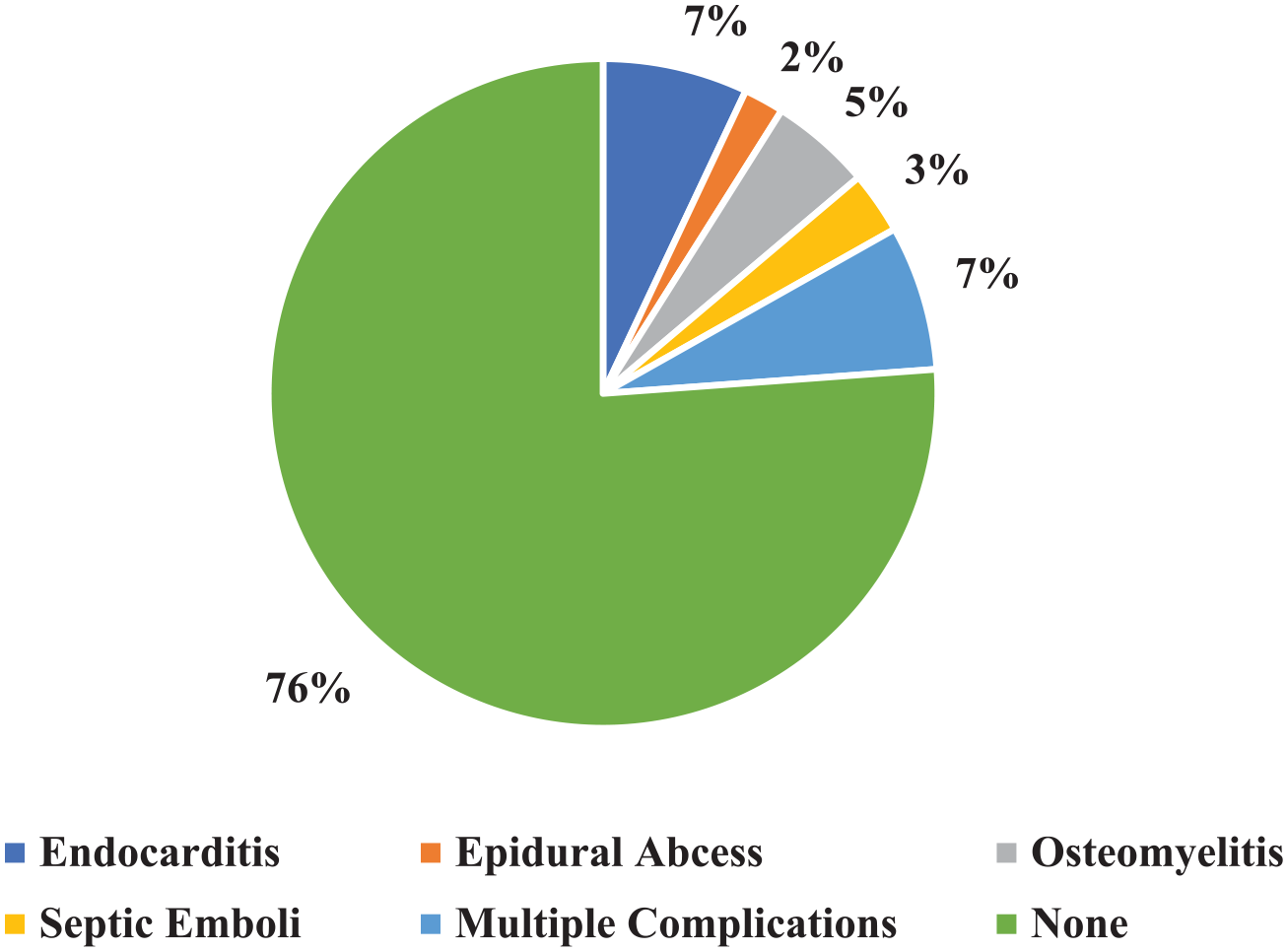
Complications in hospitalized patients with Serratia bacteremia.

In-hospital outcomes in patients hospitalized with Serratia bacteremia.
Readmission, recurrence, and mortality
In non-IV drug users, inpatient mortality occurred in two cases and was not related to Serratia bacteremia, and no mortality due to Serratia infection was observed during the 90 days follow-up. Ninety-day readmission occurred in 22 (21%) cases, not related to recurrence of Serratia bacteremia. There was a total of 19 ICU admissions, 10 (24%) of IV drug users versus 9 (15%) of non-IV drug users (p = 0.182) and septic shock requiring vasopressors occurred in 10 patients [6 (14%) of IV drug users versus 4 (7%)] (p = 0.168) (Figure 2).
Recurrence of Serratia infection within 90 days occurred in 3 (7.1%) IV drug users versus 3 (4.9%) non-IV drug users (p = 0.472) (Figure 3).

Ninety-day recurrence of Serratia infection.
Overall median (IQR) LOS was 7 days [3.25–14.75]. It was slightly higher in IV drug users, 8 [2.75–11.25] versus 6 [4–16] (p = 0.591).
Discussion
To our knowledge, this is the largest study ever published evaluating non-nosocomial or contamination-related Serratia bacteremia cases. The literature on Serratia prior to this study includes outbreaks of contaminated magnesium sulfate, propofol, and the most recent involving pre-filled heparin and isotonic sodium chloride solution syringes, in 2009.10 –12 There are also case reports of failures in sterile technique leading to Serratia bacteremia and sequelae highlighted in the literature review performed in 1974 by Farhoudi et al. 13 Our results challenge Serratia as predominately a nosocomial infection.
We aim to reintroduce IV drug use as a major risk factor for Serratia as the Californian physicians first described. The initial cases of endocarditis described in the literature from IV drug abuse in the San Francisco area highlight that direct inoculation can lead to severe outcomes. 7 Mirroring the regional effect felt in the 1970s, 42 (43%) cases in our study are attributed to IV drug use. The most common complications in all Serratia patients were endocarditis (12%) and osteomyelitis (10%). Co-infection with HCV was significant in IV drug users. The case report in 2018, provided by Ho-Man Yeung et al., 8 describes the injection drug user of the current age and devastating effects of Serratia to the IV drug user. We suspect the likely risk factor within IV drug users is lack of sterile technique, use of tap water, along with reusing of needles and frequency of IV access. Given the steady rise in IV drug use, owed in large part to the opioid epidemic facing the United States, we suspect that we will continue to see an increase in Serratia bacteremia infections.
In non-IV drug users, indwelling catheters contribute heavily to the inoculation of the infection accounting for 29 (47%) Serratia bacteremia cases seen. The second most common source of contamination included UTIs outside of indwelling catheters. These data suggest the urinary system to be the predominate source of Serratia infection outside of direct bloodstream inoculation.
The mortality of our patients was low compared with other types of opportunistic infections. We attribute this to the antibiotic regimens available to clinicians currently in medicine. The average hospital LOS for our patients was high at 7 days, with ICU admission rates at 19 (18%). Serratia isolates in our study show 15 (15%) resistance to third-generation cephalosporins (ceftriaxone), and over 37 (35%) being possible or confirmed ESBL activity.
Serratia spp. can confer resistance through AmpC β-lactamase (AmpC BL) or ESBL although the latter is rarer. Understanding the differences between AmpC BL and ESBL can be relevant as although they can have clinically similar responses to antibiotics, some important differences do exist. AmpC BL are considered class C enzymes under the Ambler classification scheme. 14 Organisms that have developed AmpC BLs are usually resistant to penicillins, cephalosporins, cephamycins, and monobactams, and they can develop resistance to beta-lactamase/beta-lactamase inhibitor combinations but are usually sensitive to carbapenems. 15 Serratia spp. usually confer inducible resistance through chromosomally encoded ampC genes as the mechanism of AmpC BL resistance, although other pathways to AmpC resistance do exist.14,16 The hallmark phenotypic pattern of AmpC BL producers is that they appear susceptible to third-generation cephalosporins if AmpC production is not induced, but resistance can develop upon β-lactam exposure as early as a single day after drug initiation.14,17 This AmpC BL pattern is inherent to S. marcescens and allows for resistance to a range of narrow-spectrum penicillins and several narrow-spectrum cephalosporins due to the chromosomal AmpC BL enzyme. 18 The inducibility of the ampC gene allows for inducible resistance to beta-lactam agents.
What makes it difficult to broadly state susceptibilities based on ampC gene presence is the variable mutations that can occur leading to β-lactamase over-production in the wild. These hyper-producing mutants confer constitutively high levels of β-lactamase production independent of inducers and demonstrate clinically significant cross-resistance to most beta-lactam agents including broad-spectrum cephalosporins, monobactams, and the beta-lactam/beta-lactamase inhibitor combinations. 18 Unfortunately, because of complexity of species resistance patterns including concomitant ESBL and limitations in molecular approaches to identifying ampC genes, there are no Clinical and Laboratory Standards Institute–endorsed criteria for AmpC detection in clinical isolates.14,19,20
ESBLs are enzymes that are typically inhibitor-susceptible β-lactamases encoded through plasmid-mediated genes and are resistant to extended-spectrum cephalosporins (third-generation cephalosporins, including ceftriaxone) and monobactams (aztreonam), but do not affect cefamycins (cefoxitin, cefotetan, cefmetazole, flomoxef) or carbapenems (imipenem, meropenem, ertapenem, doripenem).15,21 The lack of inhibition by cephamycins and β-lactamase inhibitors differentiates AmpC BL producers from ESBL producers. 15 Over the 30 years since ESBLs first emerged, their production has predominated in Klebsiella pneumoniae and Escherichia coli with incidences in the United States from 5.3% and 2.8%, respectively.18,22 However, ESBLs have been occasionally reported in other enterobacteria including Serratia spp.18,23,24
With this understanding of variable resistance mechanisms, we acknowledge the significance of our retrospective analysis of antibiotic resistance patterns is difficult to assess. The significant limitation in the lack of availability of specific isolates within our population for further analysis ad hoc leaves us with a variable gray area termed ‘possible ESBL’ which could include induced AmpC BL producers, possible ampC genetic mutant hyper-producers, or ESBL producers. This limitation is significant when evaluating the generalizability of treatment option recommendations. Further limitation can be applied to extrapolating treatment recommendations from our study given our population study was limited to one city, albeit a multi-center study. We acknowledge the potential for significant variance in local hospital and regional antibiograms for Serratia infections, even within the IV drug user population.
Currently, the Infectious Disease Society of America (IDSA) recommends cefepime as empiric therapy for Serratia spp. given some studies concluded that cefepime may be a reasonable option for treatment of invasive infections due to AmpC BL organisms, particularly when source control is achieved.25,26 The rationale for cefepime stems from its ability to have the advantage of both being a weak inducer of AmpC production and withstanding hydrolysis by AmpC β-lactamases because of the formation of stable acyl enzymes complexes.26 –28 IDSA treatment of choice for ESBL organisms is currently carbapenems. 26 Given our study findings and current guidelines, we recommend empiric therapy for Serratia spp. with cefepime or carbapenems pending full isolate susceptibility data. Aggressive and IDSA-aligned empiric therapy may help shorten LOS and readmission rates.
In conclusion, our study shows that a high proportion of patients hospitalized within our population with blood cultures positive for Serratia spp. are IV drug users and have concomitant HCV infection contradicting the previous understanding that infection is primarily attributed to nosocomial and contamination outbreaks. Understanding and curtailing the opioid epidemic in the United States will be an effective primary prevention strategy to curtailing Serratia infection incidence rates. For those cases that continue to arise, focus should be on proper antibiotic treatment as readmission rate and LOS are high. Empiric treatment should align with the current IDSA guidelines using cefepime and consideration of carbapenem use in cases of severe infection or inadequate source control.
Footnotes
Acknowledgements
The authors acknowledge the TriHealth Hatton Research Institute for their efforts. They thank Anjuli Eagleston, MD, for presenting the preliminary data at ID week 2020.
Authors’ Note
Author contributions
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research project was self-funded.
Ethics and consent
All information was obtained ethically after approval of TriHealth Institutional Review Board (IRB). Informed Consent was not required. A waiver of Informed Consent (dated 5 June 2019) was approved by the TriHealth Hatton Research Institute (IRB number 19-029).