
Abstract
Introduction:
Acute myeloid leukemia (AML) is the commonest leukemia in adults. Mortality in thew first 30-days ranges from 6% to 43%, while infections account for 30–66% of early deaths. We aim to present our experience of infections in newly-diagnosed AML.
Method:
This prospective, observational study, was undertaken at a tertiary care hospital in Northern India. Patients with confirmed AML (bone marrow morphology and flow cytometry) and who had developed febrile neutropenia (FN), were included.
Result:
A total of fifty-five patients were included in the study. The median age of the patients was 47.1 years (12–71) and 28 (50.9%) were males. Fever (33, 60%) was the commonest presentation at the time of diagnosis. One or more comorbid conditions were present in 20 patients (36.36%). Infection at presentation was detected in 17 patients (30.9%). The mean duration to develop febrile neutropenia since the start of therapy was 11.24 days. With each ten-thousand increase in white blood cell (WBC) count, the mean number of days of FN development decreased by 0.35 days (p = 0.029). Clinical and/or radiological localization was possible in 23 patients (41.81%). Thirty-four blood samples (34/242, 14.04%) from 26 patients (26/55, 47.3%) isolated one or more organisms. Gram negative bacilli (GNB) were isolated in 24 (70.58%) samples. Burkholderia cepacia (8/34, 23.52%) was the commonest organism. The number of days required to develop febrile neutropenia was inversely associated with overall survival (OS). However, when compared, there was no statistically significant difference in OS between patients developing fever on day-10 and day-25 (p = 0.063). Thirteen patients (23.63%) died during the study period.
Discussion:
Low percentage of blood culture positivity and high incidence of MDR organisms are a matter of concern. Days to develop febrile neutropenia were inversely associated with overall survival (OS), emphasizing the importance of preventive measures against infections.
Conclusion:
Infections continues to be a major cause of morbidity and mortality among AML patients.
Introduction
Acute myeloid leukemia (AML) is the commonest leukemia among adults, accounting for approximately one-third of all leukemia cases. 1 Despite decades of improvement in the management and supportive care associated with this disease, the outcomes in the real-world continue to be poor with AML induction chemotherapy. Therapy-related mortality ranges from 6% to 43% and age-wise 5-year survival is dismal (2–54%).2–4 Infections at the time of diagnosis are documented in 42–72% AML patients, accounting for up to 66% of deaths during induction.2,5–7 Delayed diagnosis of AML due to non-specific clinical features, underlying immunocompromised state and comorbidities, results in a predisposition to acquire infections and inferior outcomes with standard induction therapy.8–10
Acute leukemia management is more challenging in the developing world. Delays in presentation, due to a lack of awareness, sparsity of evaluation facilities, and the cost constraints of therapy are some of the challenges that clinicians come across in resource-constraint settings. The use of newer, targeted therapies is restricted by limited availability and cost constraints associated with a lack of universal healthcare insurance. 11 A high prevalence of infections in the community and antibiotic resistance due to the unrestricted and rampant use of broad-spectrum antibiotics further complicates disease management.12–14
The literature on infections in AML patients in the developing world is gradually evolving.2,5–7,15 These studies are very important from the clinician’s point of view, as they may improve our understanding regarding induction-related complications. Such efforts may help in designing management strategies focused on improving disease outcomes in future. We aim to present our experience of infections in newly-diagnosed AML patients who were admitted and treated at our center.
Method
This prospective, observational study was undertaken at a tertiary care hospital in Northern India. Approval from the Institutional Ethical committee of Army Hospital (Research and Referral), New Delhi, India (AHRR IEC113/2020) was obtained and patients were enrolled from January 2019 to June 2020. The study was performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments as well as local national guidelines. The patients and the family were provided with explanatory details of the study. Following this, written, informed consent was taken from the patients or their parents (if less than 18 years of age) or next of kin (if not fit for giving consent or sign consent due to the disease). After taking consent, AML patients aged 12 years or older who reported to our Hematology Outpatient Clinic or admitted for inpatient care were included in the study. The demographic details, baseline laboratory parameters, and the details of febrile neutropenia and its management, including outcomes, were entered in a predefined, password-protected excel sheet.
Eligibility criteria for the study
The inclusion criteria for the study were: (1) Patients who were confirmed to have AML (on bone marrow examination and flow cytometry) and who had developed febrile neutropenia (FN) and were evaluated and managed as inpatients.
The exclusion criteria were: (1) Patients with AML, for whom consent could not be obtained for participation in this study; (2) Children <12 years of age; and (3) Patients who had FN and were managed on an outpatient basis.
Study design
Following the diagnosis of AML, the patients were admitted or transferred to the hematology ward for further evaluation [computed tomography (CT) scan of the chest and paranasal sinuses, 2D echocardiogram, viral markers (Hepatitis B, C, and human immunodeficiency virus (HIV))] before chemotherapy. Patients with fever were also evaluated with blood culture, routine urine and microscopic examination, serum procalcitonin, and serum galactomannan. Evaluation for tropical infections was conducted depending upon the clinical presentation. Further evaluation (e.g. bronchoscopy and bronchoalveolar lavage) was conducted depending upon clinical or radiological findings. As a result, they received chemotherapy and were closely followed up during their entire stay in the hospital for any chemotherapy-related complications. The Hematology Ward has a mix of separate neutropenic cubicles and general cubicles. Patients were preferably kept in the neutropenic cubicles, subject to availability. These rooms have portable HEPA filters. All patients received acyclovir and voriconazole prophylaxis. Standard definitions for the concomitant presence of FN, sepsis, and septic shock were used.16,17 As per the departmental policy, the combination of cefoperazone-sulbactam and teicoplanin was empirically started in any patient on meeting the criteria of FN. If fever persisted for more than 48 hours, antibiotics were upgraded to piperacillin-tazobactam (2nd line) and subsequently, meropenem (3rd line). Regular clinical assessment, radiological imaging, and cultures were sought to further optimize the antimicrobials. Any patient having persistent fever beyond 72 hours was started on a therapeutic dose of amphotericin. Fungal infections were classified into possible, probable, and proven fungal disease, based on guidelines from European Organization for Research and Treatment of Cancer (EORTC). 18 The data were collected and analyzed for all patients for up to 30 days from the start of therapy for AML.
Sample collection and analysis
For culture, paired samples (8–10 ml of the blood from periphery as well central line) were taken in each BACTEC bottle and sent to the laboratory. The BACTEC bottles were incubated in the bactalert automated blood culture system (Biomerieux, France) and continuous monitoring was performed. After an organism was identified, the antibiotic sensitivity or resistance was assessed using Vitek 2 compact (Biomerieux, France) in accordance with the Clinical and Laboratory Standards Institute (CLSI) guidelines for designating an organism as sensitive, intermediate, and resistant.
Statistical analysis
The data were stored in csv format in Microsoft Excel and was analyzed with statistical software R version 3.6.3. 19 The continuous variables were summarized using mean, median, standard deviation (SD) and interquartile range (IQR); quantitative variables were summarized using proportion. All AML patients developed FN. The duration (in days) from the chemotherapy administration to the onset of FN was the primary outcomes of the study. This was summarized using mean and SD. The association of day to FN onset was assessed with various covariates using linear regression models. Induction mortality was analyzed as a secondary outcome using time to event analysis (survival analysis). This was summarized using a Kaplan–Meier Curve fitting and its association was assessed with various covariates using cox proportional hazard regression models. 95% confidence intervals (CIs) were used to assess the variation in parameter estimation and a p-value of less than 0.05 was used as evidence against acceptance of the null hypothesis.
Result
A total of 77 AML cases were diagnosed during the study period. Sixteen patients choose to get treatment from other hospitals, while one refused to give consent for the study. During follow-up, five patients were excluded from the study, as they got treatment for FN as an outpatient. Finally, 55 patients were included in the outcome analyses. The median age of the patients was 47.1 years (IQR 36–58 years); 28 patients (50.9%) were males.
The mean duration of symptoms at the presentation in our study was 2.5 (±0.93) weeks. Fever (33, 60%) was the commonest presenting complaint, followed by fatigue (13 patients: 23.63%) and bleeding manifestations (5 patients, 9%). One patient had an unusual presentation in the form of acute coronary syndrome (CAD-STEMI). One or more comorbid conditions were present in 20 patients (36.36%), including 1 patient each with history of breast and thyroid carcinoma. The majority of the patients (35; 63.63%) had good ECOG (Eastern Cooperative Oncology Group) performance status (PS) at presentation (ECOG 0 or 1), while only 2 patients (3.63%) had ECOG PS 4 (ECOG). Infections at presentation were detected in 17 patients (30.9%) and the lung was the most common focus of infection (11 patients; 20%). The baseline demographic and hematological parameters are summarized in (Table 1).
Baseline demographic and hematological parameters of the patients.

Others included, cough, 2 asymptomatic 1 acute coronary syndrome (CAD-STEMI), 1 Cervical Lymphadenopathy, 1 and pain abdomen. 1
Others included, pulmonary tuberculosis, 1 primary hypothyroidism, 1 and chronic hepatitis B (HBV) infection.
Hypomethylating agents (5-azacytidine and decitabine).
COPD, chronic obstructive pulmonary disease; ECOG, Eastern Cooperative Oncology Group; HMA, hypomethylating agent; IQR, interquartile range; PBS, phosphate-buffered saline; PICC, peripherally inserted central catheter; SD, standard deviation; WBC, white blood cells.
The mean duration from treatment initiation to FN onset was 11.24 (±0.99) days. With each ten-thousand increase in WBC count, the mean duration to FN onset decreased by 0.35 days (p = 0.029) (Figure 1). Clinical and/or radiological localization was detected in 23 patients (41.81%). The lung was the most affected organ (19/23 patients; 82.6%) followed by the gastrointestinal (GI) tract (2/23 patients; 8.69%) (Table 2). Thirty-four blood samples (34/242, 14.04%) from 26 patients (47.3%) were found to be positive for one or more organisms (Table 3).
Febrile neutropenia and subsequent localization.
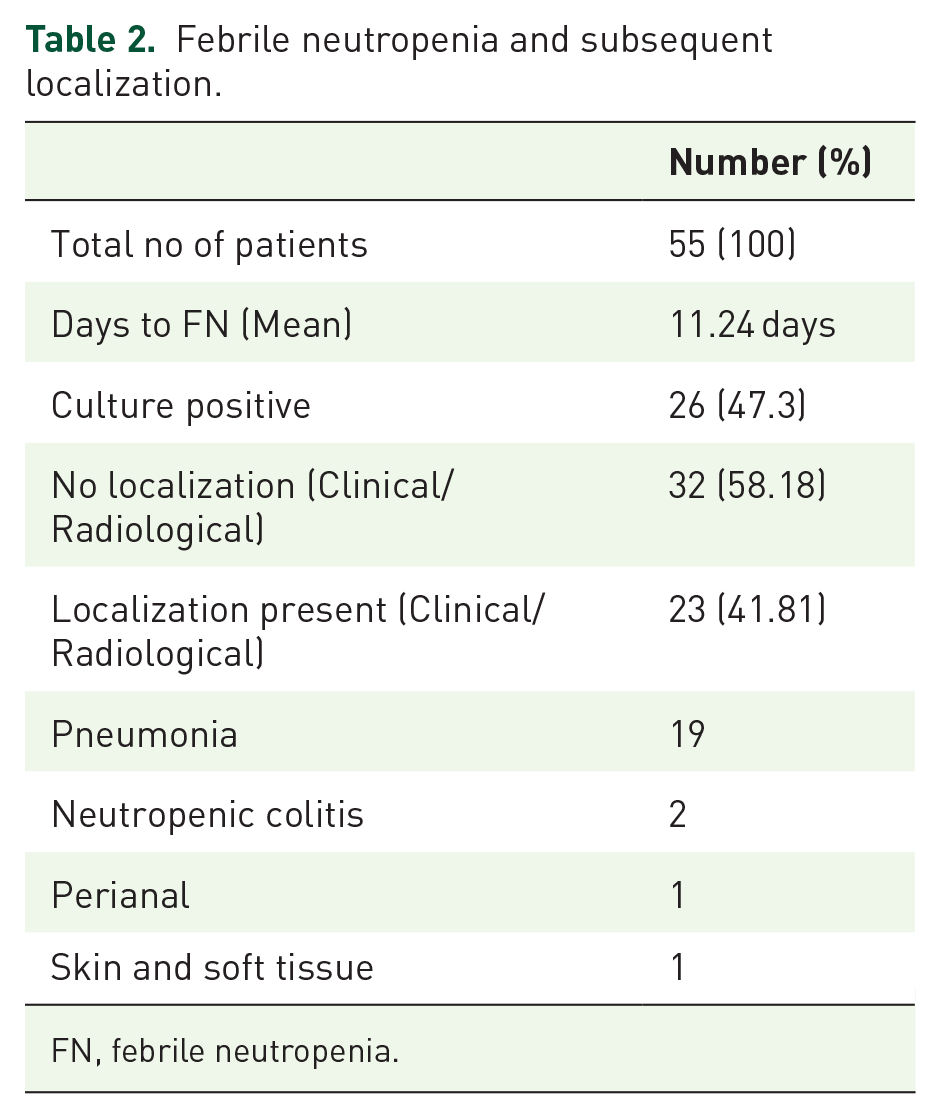
FN, febrile neutropenia.
Various samples collected and the result.

GPCc, gram-positive cocci in clusters; GNBs, gram-positive bacteria.
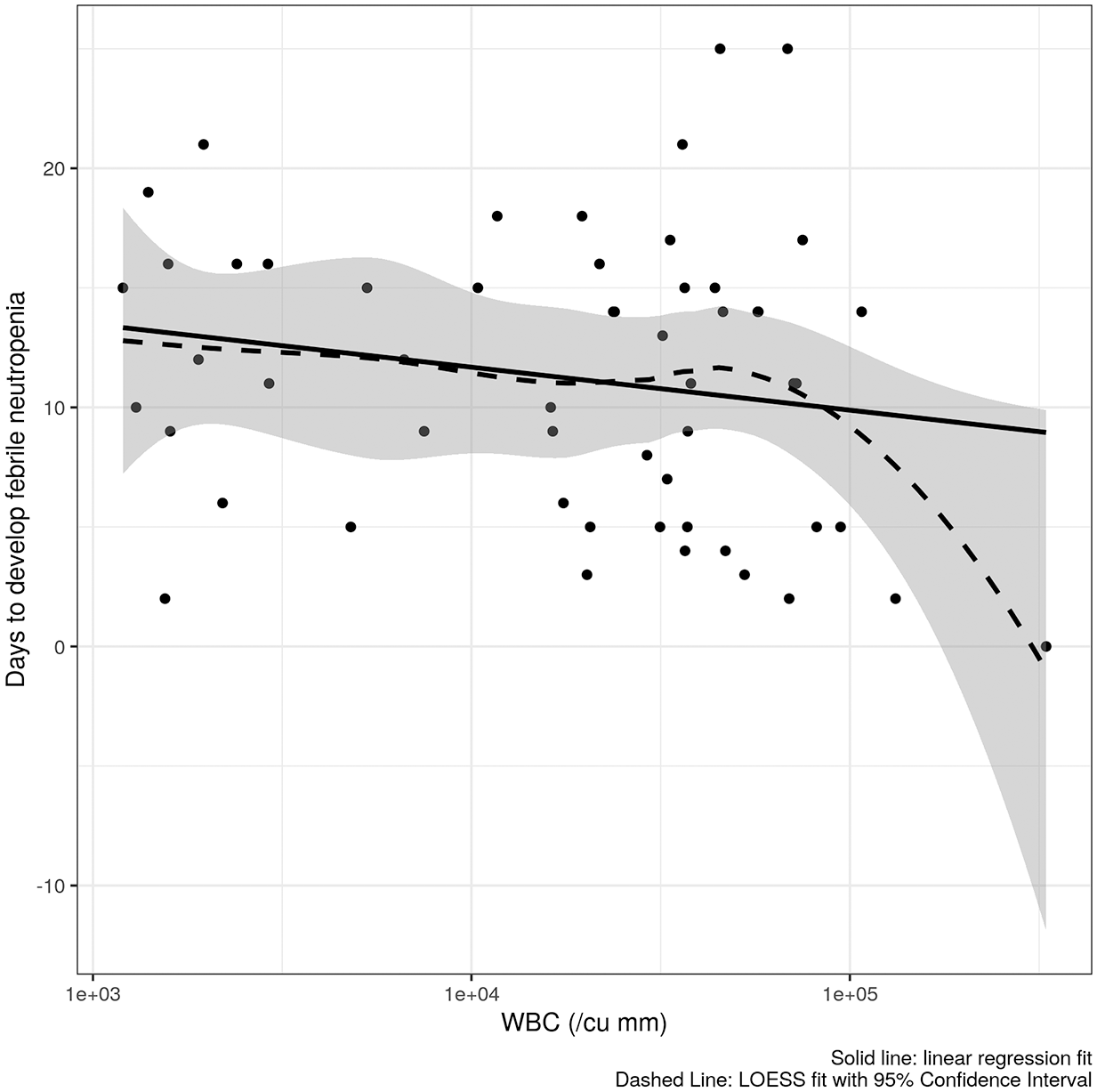
The figure depicts relationship between baseline WBC count (in/cu mm, log scale) and days to develop febrile neutropenia. The solid line represents linear regression fit and the dashed line with shade region represents the LOESS fit with 95% confidence interval.
The majority of the positive blood cultures grew gram-negative bacilli (GNB) (24/34, 70.58%) followed by gram-positive cocci (GPC) (10, 29.4%) (Table 3). Burkholderia cepacia (8/34, 23.52%) was the commonest organism, followed by Acinetobacter baumannii (A baumannii) (7/34, 20.58%). E. coli, Staphylococcus hominis, and Staphylococcus haemolyticus were isolated in 4 samples (11.76%) each. Klebsiella pnemoniae (K pneumoniae) and Psedomonas aeroginosa (P aeroginosa) were isolated in 2 samples (5.88%) each. Six of the 7 isolates (85.71%) with A baumannii were carbepenem resistant. All K pneumoniae isolates (2/2, 100%) and half of the E. coli and P aeroginosa (1/2, 50%) were carbepenem-resistant. Only one isolate on blood culture (P aeroginosa) was found to be colistin-resistant (Table 4).
Organisms on blood cultures and their resistance pattern.

All patients received a combination of cefoperazone-sulbactam and teicoplanin as empirical therapy within one hour of diagnosis of FN. The antibiotics were subsequently changed depending upon radiological or microbiological findings or clinical response to the ongoing antimicrobial therapy. Meropenem was administered for the longest duration amongst the patients included in the study. All patients received one or two antifungals (caspofungin and/or amphotericin B) for suspected fungal infection during their hospital stay. Thirty-five patients were categorized into possible fungal infection and 22 into probable fungal infection.
The duration from treatment initiation to FN onset was inversely associated with overall survival (OS) (Figure 2). However, when compared, there was no statistically significant difference in OS between patients developing fever on day-10 and day-25 (p = 0.063) (Figure 3). Out of all the AML patients included in the study, 13 (23.63%) died, and 42 (76.36%) patients were on follow up at the end of day 30 (Figure 4).

The figure depicts the relationship between days to febrile neutropenia with estimated 30-day survival probability, with shaded region representing 95% CI.
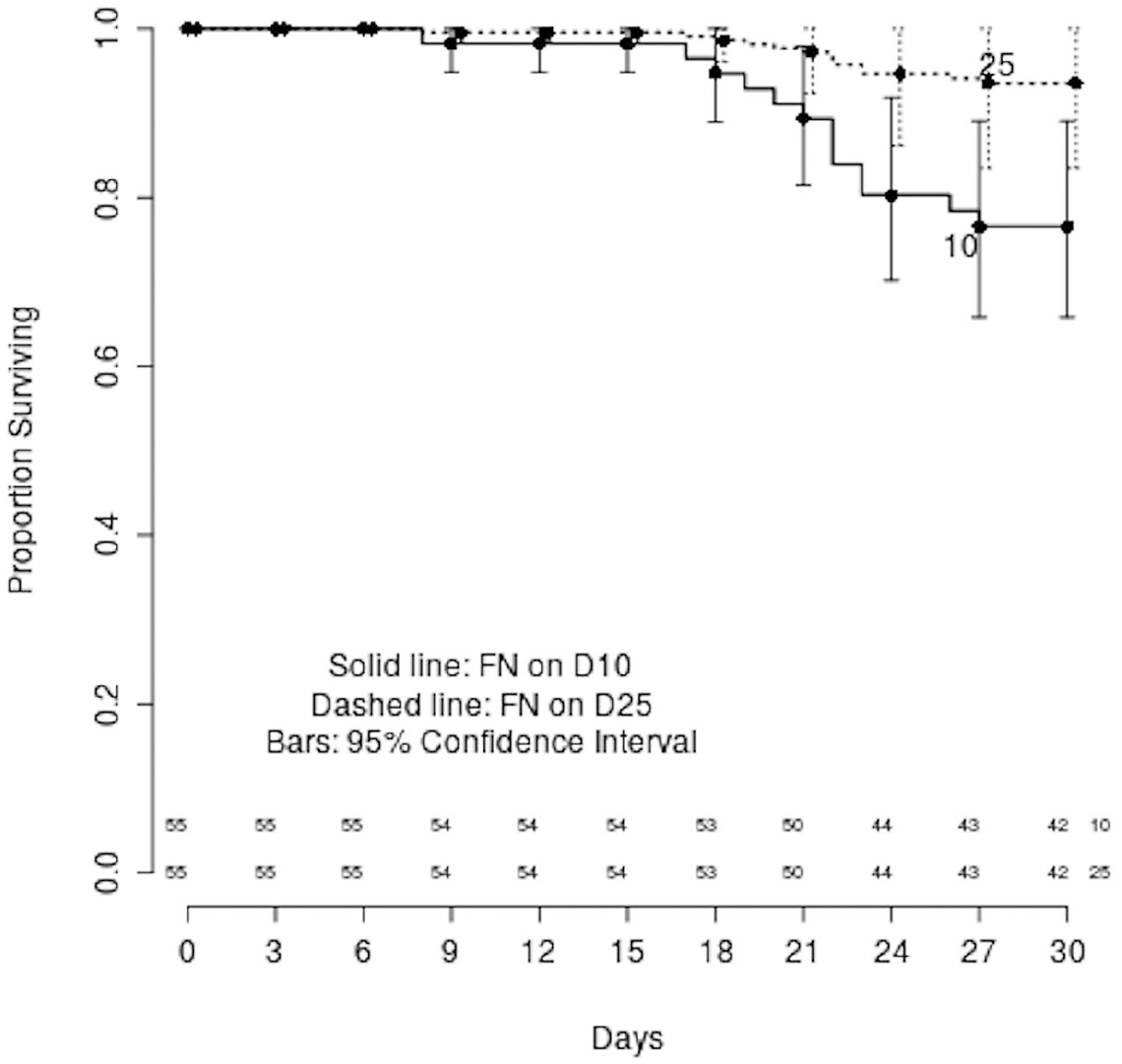
The figure depicts estimated survival curves from cox proportional hazard regression model of induction mortality with follow up time (in days) in cohort of patients who develop febrile neutropenia after 10 days (solid line) and those who develop febrile neutropenia after 25 days (dashed line). The bars depict 95% CIs at each time points. The numbers along the x-axis represent the number of patients at risk at that time point (depicted in x-axis).

The figure depicts Kaplan–Meier Curve of induction mortality with follow up time (in days). The bars depict 95% CIs at each time points. The numbers along the x-axis represent the number of patients at risk at that time point (depicted in x-axis).
Discussion
The median age of patients in our study was 47 years. This is lower than the published studies from the developed world, which suggest that the median age of AML patients is 68 years and it is uncommonly in seen in adults younger than 45 years of age. 20 However, previous studies published from India suggest that AML patients are younger than their western counterparts, with their age ranging from 30 to 36 years.2,9 One of the reasons for this may be the lower life expectancy in India, while there may be other selection biases in the study. Another reason for the lower median age in our cohort may be due to enrolment at a lower age (>12-year) in our study compared with many western world reports (>18-year).
The mean duration of symptoms at the presentation in our study was 2.5 weeks. This is lower than the published data ranging from 4 to 7 weeks.21,22 Twenty patients (36.36%) had one or more comorbidities in our study. Essential hypertension was the most common (16/55 patients; 29%), followed by diabetes mellitus (5/55 patients; 9%). Diabetes mellitus is found to be associated with an increased risk of induction mortality in AML patients. 23 In our study, 17 patients (30.9%) had evidence of infection at presentation. This is higher than what has been published from the developed world, which ranges from 20% to 30%. 24 However, it is in congruence with the published data from India, which ranges between 30% and 60%.5,6,10,22
All our patients developed infections during the study period. On univariate analysis, factors such as age, sex, symptom duration, ECOG performance status, and comorbidity, were not statistically significant for the development of fever or acquiring infection during induction therapy. Prior studies in AML patients have also noted that FN develops in 90–100% of patients during induction. 25 After meticulous clinical, radiological, and microbiological assessment, we could localize the source of infection in 23 patients (41.81%). The lung (19/23, 82.6%) was the organ most commonly involved. The incidence of lung infection at baseline ranges from 21% to 47% in published studies.10,26,27 Twenty-six patients (47.3%) with fever had blood culture positivity in our study. In published reports, blood culture positivity ranges from 22% to 56%.6,10,28,29 In our study, GNBs were isolated more often (70.58%) than GPC (29.4%). The real-world and clinical trials data from developed countries suggests a predominance of GPBs among the positive isolates.29,30 Our findings of lower incidence of GPB isolates are similar to the previously published data of 20–25% GPB isolates from the Indian subcontinent.10,31 The probable explanation for this is a lack of fluoroquinolone prophylaxis and breach in the gut barrier following anthracycline-based chemotherapy.32–35 B cepacia and A baumannii were the most common organisms in our study. While all B cepacia isolates were carbapenem-sensitive, most of the A baumannii isolates (6/7, 85.71%) were carbapenem-resistant, which is indeed a matter of concern. The incidence of multi-drug resistant (MDR) organisms has been reported to be between 25% and 55% from the Indian subcontinent.2,10
Thirteen patients (23.63%) succumbed to their illness during the 30-day follow up of our study. Induction-related mortality in AML has been reported to vary from 6.1% to 43% from different centres across India.2,10 Comparatively, the mortality is higher in our cohort, which may be due to lack of selection bias in our patients. In our study, all consecutive AML patients were admitted to hospital irrespective of affordability. Age, multidrug resistant (MDR) organism, time to chemotherapy initiation, and comorbidities have variable effect on mortality in AML induction.20,36–38 In our study, on the univariate analyses, age, sex, symptoms duration, performance status, comorbidity, blood culture positivity, or organ localization had no significant effect on outcome. Days to develop FN were inversely associated with OS, though there was no statistically significant difference in OS. This finding emphasizes the importance of continued preventive measures against infections.
The small study size and single center experience are the major limitations of our study. We did not report the pattern and outcome of infections during further treatment (consolidation) among the patients included in the study.
The major strength of our study was the homogeneity of the study population. The pattern of infections observed in our study may be helpful to transplant centres located in similar settings for designing their management protocol. By contributing to existing knowledge base, the findings of our study shall be helpful in designing future studies (including randomized controlled trials) on antimicrobial prophylaxis and treatment in resource-constraint settings.
ConclusionInfections continue to be a major cause of morbidity and mortality in AML patients receiving standard induction therapy. There is a lot of scope for improvement in infection-related outcomes among AML patients, particularly in resource constraint settings. In addition to improvements in hygiene control measures, there is a need to adapt protocols to local microbiological epidemiology on a time-to-time basis for the prevention and treatment of infections.
Footnotes
Acknowledgements
The authors acknowledge the help of Nand Kishor and Ankit Tewari during data collection. Our sincere thanks to all our patients, without whom, the study was not possible.
Author contributions
KM, SK, AJ, KKS, and RS conceptualized the study design. KM, SK, AJ, KKS, RS, SN, and KJS wrote the manuscript. All authors were involved in the patient management and vetted the manuscript.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.