
Abstract

Introduction
Dengue virus is a single-stranded RNA virus comprising four distinct serotypes. These closely related serotypes belong to the genus Flavivirus, family Flaviviridae. Dengue imposes a significant health, social, and economic burden in endemic areas. Dengue virus is transmitted through the bites of infected Aedes aegypti mosquitoes. Most of the resulting infections are asymptomatic or subclinical. The characteristic hemorrhagic manifestations of severe dengue are plasma leakage due to increased vascular permeability, thrombocytopenia, and hemoconcentration. These may present as petechiae, epistaxis, gingival bleeding, and only rarely, significant bleeding. Such bleeding, along with transient bone-marrow suppression seen in dengue fever, are the documented causes of anemia in dengue fever. Cold-agglutinin hemolytic anemia has not been reported in association with dengue fever. We present a rare case of a patient who developed hemolytic anemia following the formation of transient cold agglutinins secondary to dengue-virus infection.
Case report
A 52-year-old north Indian woman presented with complaints of high-grade continuous fever of 4 days duration and generalized rash in the winter season. Her medical problems included long-standing diabetes mellitus, well controlled on oral medications. There was no history of tobacco, alcohol, or illicit drug use.
Initial vital signs on admission included a temperature of 41.2℃, tachycardia (heart rate 112), blood pressure 100/60 mmHg, and respiratory rate of 16/min. Relevant physical examination revealed a lean-built woman with extensive petechiae all over the body. There was no evidence of lymphadenopathy, splenomegaly, or hepatomegaly. There was no evidence of any mucosal site bleeding or ulcerations. Systemic examination was normal.
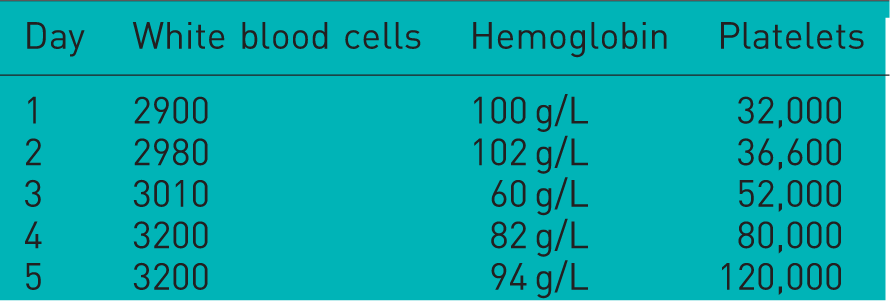
Hematological parameters during the acute phase of illness.
Workup for infectious etiology of cold agglutinins.

Workup for noninfectious etiology of cold agglutinins.

The patient was continued on conservative management. She was administered three units of packed red blood cell (RBC) transfusions over 3 days. Since she did not exhibit any serious hemorrhagic manifestations, platelet transfusion was not needed. She gradually experienced defervescence of fever and platelet counts returned to normal. She was discharged after 10 days of hospital stay in a hemodynamically stable condition.
Follow up of the patient after 1 month revealed a negative direct Coombs test and no evidence of cold agglutinins in the blood.
Discussion and conclusion
Cold agglutinins are antibodies directed at RBC carbohydrate antigens that are active at low temperatures, generally less than 37℃, with the majority of them being IgM antibodies [Stone, 2010]. Macroscopically visible clotting has been known to occur at room temperature in cases of very high cold-agglutinin titers [Heni and Saur, 2013]. IgM antibodies, which cause cold-agglutinin hemolytic anemia, may be polyclonal or monoclonal in nature. Polyclonal antibodies are generally postinfectious and the resulting hemolysis is generally self limiting, though at times may require transfusion support. Monoclonal antibodies causing cold-agglutinin hemolytic anemia are generally associated with underlying hematological malignancies such as non-Hodgkin’s lymphoma and Waldenstrom’s macroglobulinemia. Moreover, they persist indefinitely [Gertz, 2006].
Secondary cold agglutinins are associated with certain infections, notably Mycoplasma pneumoniae. They have also been infrequently reported in association with some viral infections such as EBV, CMV, HIV, and rubella [Khan and Ayassin, 2009; Shankar et al. 2009; Konig et al. 2001]. There has been no previous documentation of cold-agglutinin hemolytic anemia in association with dengue fever, where the hemorrhagic manifestations are characterized by increased vascular permeability, thrombocytopenia, and hemoconcentration [WHO/TDR, 2009]. Moreover, causes of anemia in dengue are generally secondary to transient depression of bone marrow and bleeding complications if any [Noisakran et al. 2012].
In view of the rising incidence of dengue fever and a greater understanding of the disease, atypical manifestations of dengue fever are increasingly being diagnosed. It is likely that dengue virus is capable of inciting the formation of transient polyclonal antibodies directed at RBC antigens resulting in complement-mediated hemolysis. Moreover, recovery from dengue fever results in the resolution of hemolysis.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare no conflicts of interest in preparing this article.