
Abstract
Introduction
It is estimated across a lifespan that 47% of women and 40% of men will develop symptomatic knee osteoarthritis. 1 Osteoarthritis (OA) is the most common form of arthritis, 2 which is a leading cause of disability globally. 3 At present, OA is not considered to be a curable disease, in part, because the pathophysiological mechanism is not yet comprehensively understood. 4 The goal of OA treatment is to slow the progression and alleviate the symptoms of the disease.
Traditionally, initial treatment consists of conservative options such as physiotherapy, orthotics and pharmacology. If all conservative options are exhausted, and the pathological indicators reach a threshold of severity, then surgical options are considered.5,6 Given the central role of psychosocial factors in the maintenance of chronic knee pain, 7 a prolonged period of poor treatment response can have serious implications for the entrenchment of chronic pain. Mild-to-moderate OA, resistant to nonsurgical options yet not severe enough to warrant join replacement, poses a significant management problem. Genicular artery embolisation (GAE) is an interventional radiological technique that is easier to deliver and less invasive than conventional surgical approaches, such as knee arthroplasty. GAE is designed to subvert neoangiogenesis within the joint, hypothesised to contribute to structural damage and pain in knee OA.8–11
Preliminary data for GAE indicates a subset of patients who do not respond to treatment, despite a technically successful procedure.8,12 These findings are also mirrored within more invasive surgical options such as total knee replacement (TKR), wherein 6–30% of patients continue to experience post-surgical chronic pain.13–15 It is clear that a strictly pathophysiological approach to the assessment of pain is ineffective 16 and that to understand the interpatient variability in outcomes we must complement these assessments with psychosocial insight. Moreover, optimising these assessments for prediction may facilitate earlier intervention, to help disrupt the negative progression of the chronic pain cycle.
Pain catastrophising (PC) is a cognitive-affective bias characterised by a negative interpretation of the consequences of pain.17,18 Catastrophising is regularly quantified using the Pain Catastrophising Scale, 19 comprising three main elements; rumination, magnification and helplessness. PC has been associated with lower pain thresholds 20 and poor longitudinal surgical response to a range of conditions,21,22 including knee osteoarthritis.15,23,24 Alongside its predictive capabilities, in instances where high PCS scores could facilitate worse outcomes, it has been shown to be modifiable by psychological intervention,25–27 potentially improving clinical outcomes.
Evidence suggests catastrophising is not directly associated with the sensory-discriminative dimensions of pain, but instead the unpleasantness of pain. 28 Attentional regulation plays a key role in catastrophising, with high catastrophisers often struggling to disengage attention from pain. 29 As such, neuroscientific investigation focuses on regions such as the dorsolateral prefrontal (DLPFC), anterior cingulate (ACC), insula and medial prefrontal cortices. These regions are associated with the emotional, and attentional modulation of pain, as well as pain salience, vigilance and awareness.30,31 Specifically, the dlPFC is thought to play a role in top-down modulation, underlying the facilitatory influence of PC on pain.31–35 Therefore, while PC is not directly associated with the sensory-discriminative response to pain, the processing and suppression of this sensory information may underlie the maladaptive influence of catastrophising.18,28 Furthermore, the manner in which individuals attend to pain involves an interaction between top-down and bottom-up influences and is likely to facilitate catastrophisation. 29
In the current study, we examined pre-surgical patient characteristics and tested our experimental hypothesis that higher pain catastrophising would predict worse clinical outcomes following GAE. Secondly, we investigated the influence of pain catastrophising on Intrinsic Attention to Pain(IAP), specifically, whether catastrophisers have a higher tendency to attend towards pain. Lastly, to better understand intrinsic neural mechanisms, we used resting-state fMRI (rs-fMRI) to examine dlPFC-to-whole brain neural connectivity at rest. We hypothesised that the neural mechanism underlying PC would be associated with variable connectivity of the dlPFC, as a key region in pain modulation and the suppression of pain intensity, 31 and regions of the brain associated with sensory processing of nociceptive signals, such as the motor and somatosensory cortices.36,37
Methods
Sample
Thirty-five patients with a diagnosis of mild-to-moderate knee OA volunteered for a collaborative research study (The GENESIS Study IRAS: 237676, CPMS: 37741) between the University of Reading and the Royal Berkshire NHS Foundation Trust. All patients consented to procedures approved by the Health Research Authority, the NHS London Bromley Research Committee and the University of Reading Research Ethics Committee. Two patients declined to participate in the study after the procedure was completed, two patients decided to pursue referrals for knee replacement and another patient discontinued their participation due to cumulative delays caused by COVID-19. Within this sample, a subset of 20 patients agreed to take part in a neuroimaging session, of which three patients did not complete the MRI scan due to claustrophobia. This left a final behavioural sample of 30 patients (Mage = 61.7, sd = 11.1years; 15 females) and a final neuroimaging sample of 17 patients (Mage = 58.7, sd = 9.5years; 10 females).
The inclusion criteria for the study were a minimum age of 45, a diagnosis of mild-to-moderate knee OA and knee pain for at least 6 months, which was resistant to conservative treatment methods. Patients were excluded if they had infectious or rheumatoid arthritis, severe knee OA, renal impairment, bleeding diathesis, irreversible coagulopathy or previous knee arthroplasty. Patients were also required to have acceptable comprehension of English and have no MRI contraindications.
Materials
Thermal stimulation
Noxious heat stimuli were generated using a MEDOC Pathway system (Ramat-Yishai, Israel), with a 30 × 30 cm Peltier thermode. The thermode was securely attached to the underside of the lower right arm, with the patient’s arm resting on their upper thigh for comfort and to keep the thermode stable.
Presurgical questionnaires
Prior to the embolisation, patients completed a series of questionnaires designed to quantify psychological dimensions that have been previously associated with poor surgical outcomes.23,38–40 Pain catastrophising was quantified using the Pain Catastrophising Scale (PCS, 19 ; a 13-item measure scored using a five-point Likert scale (0 = ‘not at all' to 4 = ‘all the time'). The PCS can be used as a unidimensional measure, or can be subdivided into three subscales; rumination, magnification or helplessness.
The other included measures were the Five Factor Mindfulness Questionnaire (FFMQ), 41 the State-Trait Anxiety Inventory (STAI) 42 ; and Becks Depression Inventory (BDI) 43 and the Pittsburgh Sleep Quality Index (PSQI). 44
Outcome questionnaire
Throughout participation in the study, patients completed three questionnaires to evaluate outcomes. The Knee Injury and Osteoarthritis Score (KOOS 45 ) is a 42-item knee-specific measurement tool frequently used to evaluate treatment response for knee OA by assessing patients opinions about their knee. The KOOS is a multi-dimensional tool with five distinct subfactors; Pain, function in daily life, other symptoms, function in sports & recreation and quality of life. Validation of the KOOS requires analysis to be restricted to its separate subscales, rather than an averaged composite score, and for this reason, the pain subscale (KOOS_Pain) was used as the primary outcome variable. Scores on the KOOS are calculated as a percentage of total score achieved (0–1), with lower scores signifying worse pain. The KOOS is the extension of another measure, the Western Ontario and McMaster Universities Arthritis Index (WOMAC 46 ), a 24-item measure which can be used unidimensionally. Lastly, patients were asked to provide a 0–100 pain intensity rating specifically for their knee, using a numeric rating scale (NRS; 0: ‘No pain at all’; 100: ‘The most intense pain imaginable’). All three outcome measures were collected at baseline, and post-surgically at 6-weeks, 3-months and 12-months.
Design
The current study forms part of the GENESIS study, the interim and full analyses of which provides a full description of the GAE assessment protocol and procedure.47,48 After the initial clinical assessment, patients attended a single-session assessment at the University of Reading. Patients firstly completed a sensory pain assessment. After this, patients either completed the presurgical questionnaires, or provided the questionnaires printed and completed from home within 7 days of the assessment. Lastly, patients then completed a neuroimaging session.
Procedure
Sensory pain assessment
Firstly, pain thresholds were calibrated using a dual method approach. Both methods utilised an NRS, anchored with 0 as ‘no pain’ and 10 as ‘most intense pain’. This dual-method approach utilised a method-of-limits and method-of-levels design, with the ultimate threshold being calculated as the average of these two tests. For a full description of the procedure, please refer to Harrison et al., 2019. 49
After the calculation of threshold, patients completed an intrinsic attention to pain (IAP) task, adapted from Kucyi et al., 2013. 50 An initial temperature calibration was completed with a dummy 20-s stimulus set at threshold+1°C. If patients provided a rating outside of 5–7/10, the stimulus temperature was raised or lowered by 0.5°C, and calibration was restarted. This process repeated until a rating between 5 and 7/10 was given. The IAP task was completed in silence and consisted of 10 consecutive 20-s stimuli with a 30-s interstimulus interval (ISI) at a baseline temperature of 32°C, and ramp rate of 8°C/s. After each stimulus, a rating was provided using a different NRS, wherein patients rated to what extent they had been thinking about pain or something else (−2: ‘Only something else', −1: ‘Mostly something else', 1: ‘Mostly pain', 2: ‘Only pain'). IAP score was calculated as an average of the 10 ratings, with a positive value indicating a proclivity for attention to pain.
fMRI acquisition
Functional images were acquired using a Siemens MAGNETOM Prisma 3T scanner (Siemens, Erlangen, Germany), using a 64-channel head and neck coil. The protocol consisted of an initial localiser, followed by a resting-state scan, in which patients were instructed to lie still, and keep their eyes open. Functional data were acquired using a blood-oxygen level-dependent (BOLD) protocol with a T2*-weighted gradient echo planar imaging sequence (TR = 1000ms, TE = 30s, FA = 90°, 256x256 matrix, voxel size = 2 × 2 × 2, FOV = 256 mm). To reduce the impact of field inhomogeneity, an initial five volumes were discarded, and subsequently 600 volumes were acquired, equally a total scan time of 10 min and 28-s. Following the resting-state, two field maps were collected, followed by a 5-minute T1-weighted inversion recovery fast gradient echo high-resolution anatomical scan (TR = 2300ms, TE = 2.29ms, slice thickness = 2.1 mm, FA = 8°, 256x256 matrix, voxel size = 0.9 × 0.9 × 0.9, FOV = 240 mm).
Behavioural analysis
To evaluate the efficacy of the surgical procedure, data were inspected for normal distribution and subsequently a repeated-measures ANOVA was performed to test for a difference in mean pain ratings across four time-points (baseline/6-weeks/3-months/12-months). In the case of a significant mean effect, paired t-tests were then performed as post-hoc tests evaluating the differences in KOOS_Pain ratings between baseline, and the three subsequent time-points (6-weeks, 3-months and 12-months). To assess the relationship between presurgical baseline measures, Pearson’s correlations were performed for catastrophising (PCS), mindfulness (FFMQ), sleep quality (PSQI), anxiety (STAI) and depression (BDI) scores, as well as their relationship with baseline pain (KOOS_Pain, NRS and WOMAC). Additionally, to investigate the predictive capabilities of PCS, linear regressions were conducted with PCS as the independent variable, and KOOS_Pain change as a dependent variable. For this analysis, change variables were coded by calculating the difference between 6-weeks/3-months/12-months and baseline, so that higher positive values represent stronger reductions in pain. Regarding the sensory pain assessment, to evaluate how catastrophising may be associated with a tendency to attend to pain, correlations were conducted between PCS and IAP scores. The significance level was set to p < .05 for all analyses, which were completed using IBM SPSS Statistics 23(IBM Corp. Version 23)
fMRI analysis
ROI selection
A DLPFC mask was identified using the Harvard–Oxford cortical 100% probabilistic structural atlases. Due to no specific hypotheses regarding lateralised neural mechanisms within resting-state, a bilateral mask was then created using this method (Figure 1). The DLPFC was selected as a seed due to its prominent role in top-down modulation of pain,28,34 as well as its association with pain catastrophising.32,35 Bilateral dorsolateral prefrontal cortex seed across axial (top) and sagittal (bottom) planes, with co-ordinates shown in mm.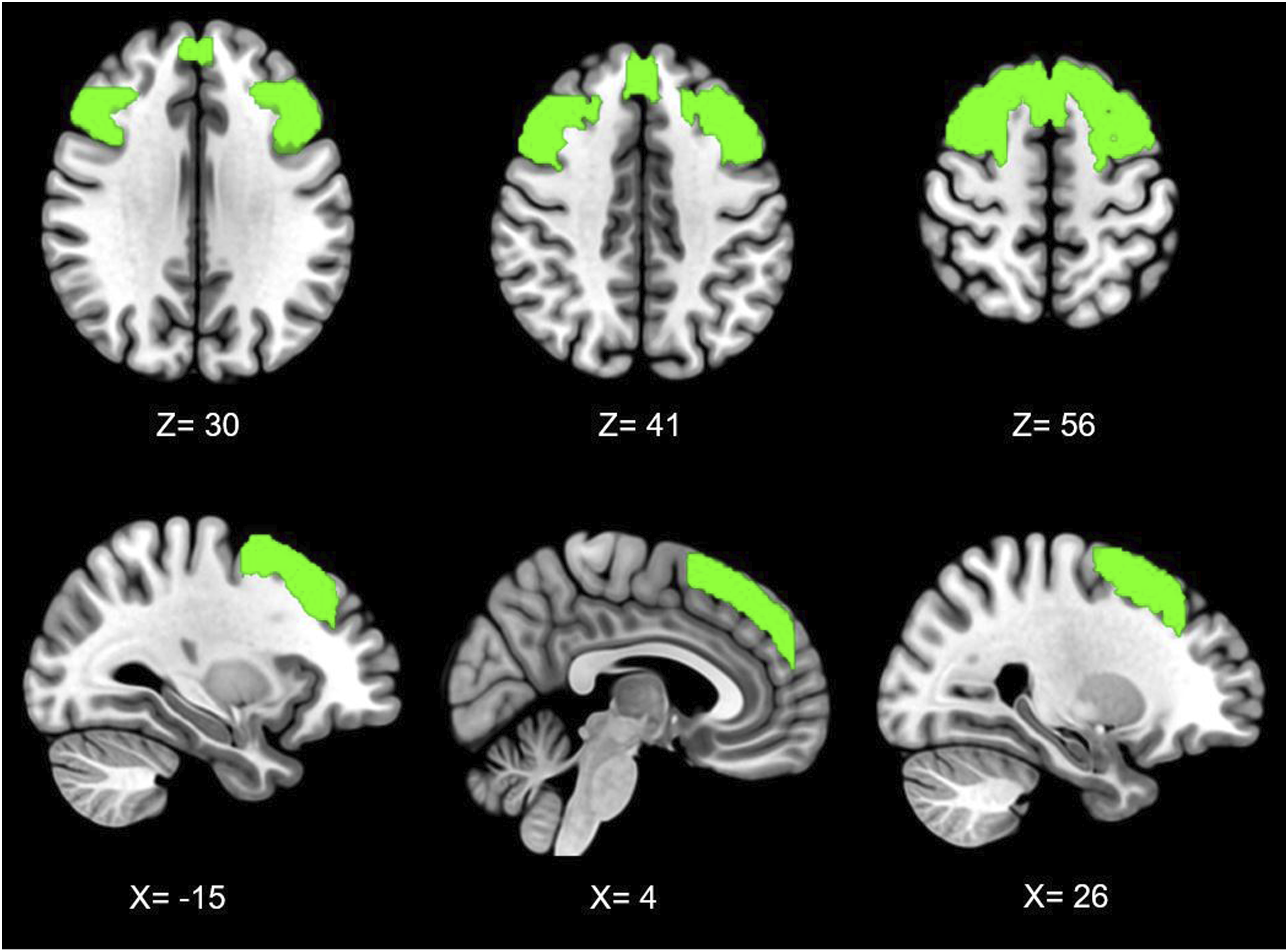
Pre-processing
All analysis was performed using FMRIB’s Software Library Package (FSL 6.0 51 ), following the Component Based Noise Correction Method (CompCor 52 ). During acquisition, the first five volumes were discarded to facilitate signal equilibration. Correction for interleaved acquisition was applied and data were spatially smoothed using a 5 mm full-width half-maximum Gaussian kernel. The Brain Extraction Tool (BET 53 ) was used for skull stripping. MCFLIRT 54 was used for the purposes of motion correction, and data were visually inspected to identify problems with registration, inadequate skull-stripping or uncorrected motion artefacts. To reduce the influence of non-neuronal activity, FAST 55 was then used to create segmented white matter and cerebrospinal fluid masks, which were then thresholded to 0.99. Time-series were then extracted for each participant and added to the GLM as nuisance variables. Residuals from pre-processing and nuisance removal were then normalised and band-pass filtered (0.1/0.001 Hz) to reduce the influence of high-frequency (i.e. cardiac/respiratory) and low-frequency (i.e. scanner drift) factors.
Resting-state connectivity analysis
The standardised DLPFC mask was registered to single-subject space, and a mean time series of all voxels within the ROI were extracted and added as an explanatory variable within a whole-brain functional connectivity analysis. Resulting contrast maps were then used as inputs within a higher-level analysis, alongside patient’s normalised pain catastrophising scores. The purpose of this analysis was to identify regions were connectivity to the DLPFC was associated with individual differences in PCS. Using FEATQuery, parameter estimates were extracted from resulting significant clusters for the purposes of the graphical representation of connectivity. Multiple comparisons corrections were applied using the Gaussian random field theory (Z <2.3; p < .05).
Results
Embolisation pain outcomes
At baseline, the mean NRS pain rating was 59.8/100 (sd = 19.6), which reduced to 33.8 (sd = 25.5) 6-weeks post-surgery (Figure 2). Pain ratings remained lower than baseline at 3-months (M = 37.9, sd = 23.6) and at 12-months (M = 43.3, sd = 26.4). Regarding the rating of osteoarthritis pain via KOOS, embolisation resulted in improvements in pain from baseline to 6-weeks (t(28) = −5.1, p < .001), 3-months (t(28) = −3.9, p = .001) and 12-months (t(26) = −2.6, p = .01). This data, alongside that previously published,8–10,12 indicates that embolisation is a suitable treatment for the management of mild/moderate osteoarthritis. Longitudinal outcomes in self-reported pain following successful completion of genicular arterial embolisation (standard error bars). | Higher KOOS values represent better pain outcomes (i.e. lower pain).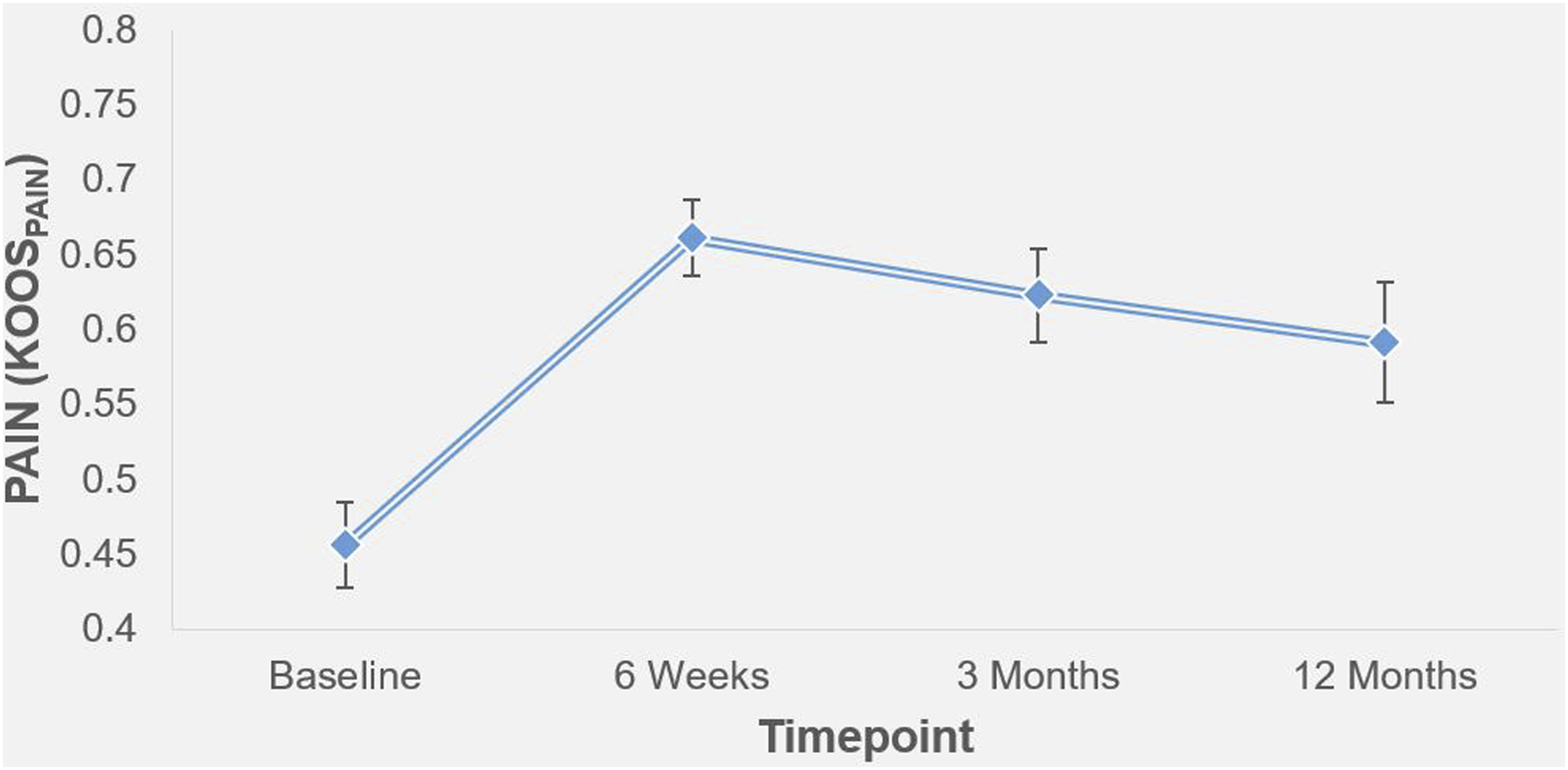
Presurgical baseline psychometrics
Association between presurgical baseline variables.
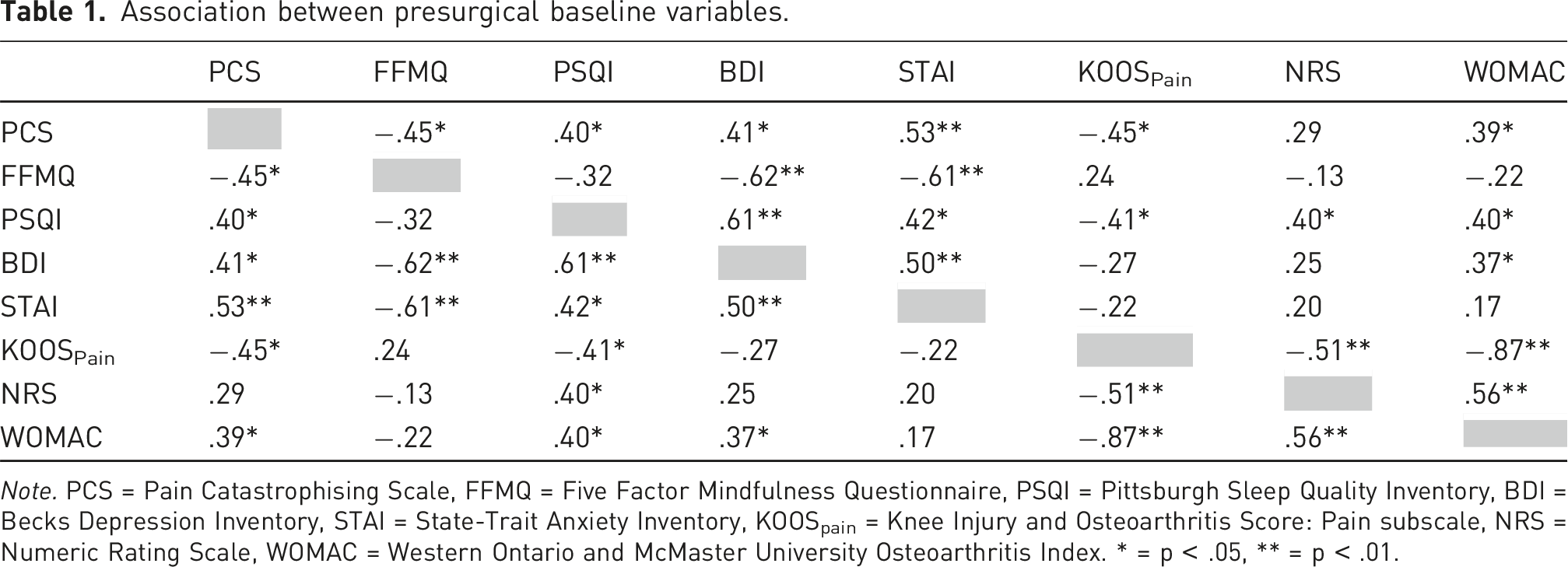
Note. PCS = Pain Catastrophising Scale, FFMQ = Five Factor Mindfulness Questionnaire, PSQI = Pittsburgh Sleep Quality Inventory, BDI = Becks Depression Inventory, STAI = State-Trait Anxiety Inventory, KOOSpain = Knee Injury and Osteoarthritis Score: Pain subscale, NRS = Numeric Rating Scale, WOMAC = Western Ontario and McMaster University Osteoarthritis Index. * = p < .05, ** = p < .01.
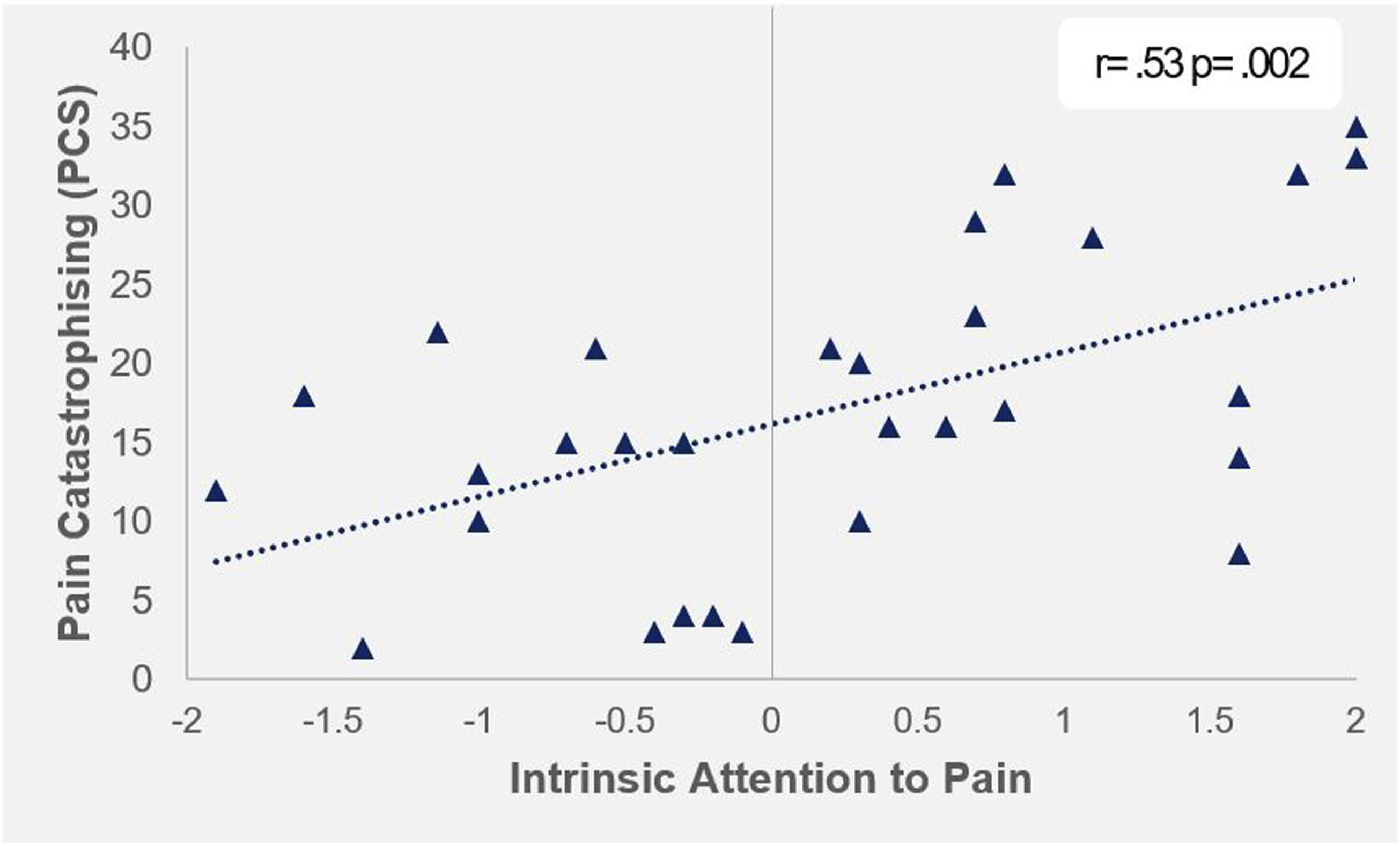
Association between pain catastrophising and intrinsic attention to pain | Positive values on IAP represent attention to 'pain', negative values represent attention to 'something else'.
Pain catastrophising and postsurgical outcomes
Pain catastrophising significantly predicted reductions in pain at 6-weeks (F (1,27) = 5.74, p = .024, R2 = .18, R2adjusted = .15, SE_β = .42), 3-months (F (1,28) = 16.32, p < .001, R2 = .37, R2adjusted = .35, SE_β = .61) and 12-months (F (1,25) = 5.49, p = .027, R2 = .18, R2adjusted = .15, SE_β = .42). Counter to a-priori hypotheses, this suggests that patients who are high catastrophisers stand to gain the most beneficial reductions in pain following embolisation (Figure 4). The association between baseline pain catastrophising, and reductions in pain at 6-weeks, 3-months and 12-months (clockwise). | KOOS ratings displayed are extracted from the KOOS_Pain subscale.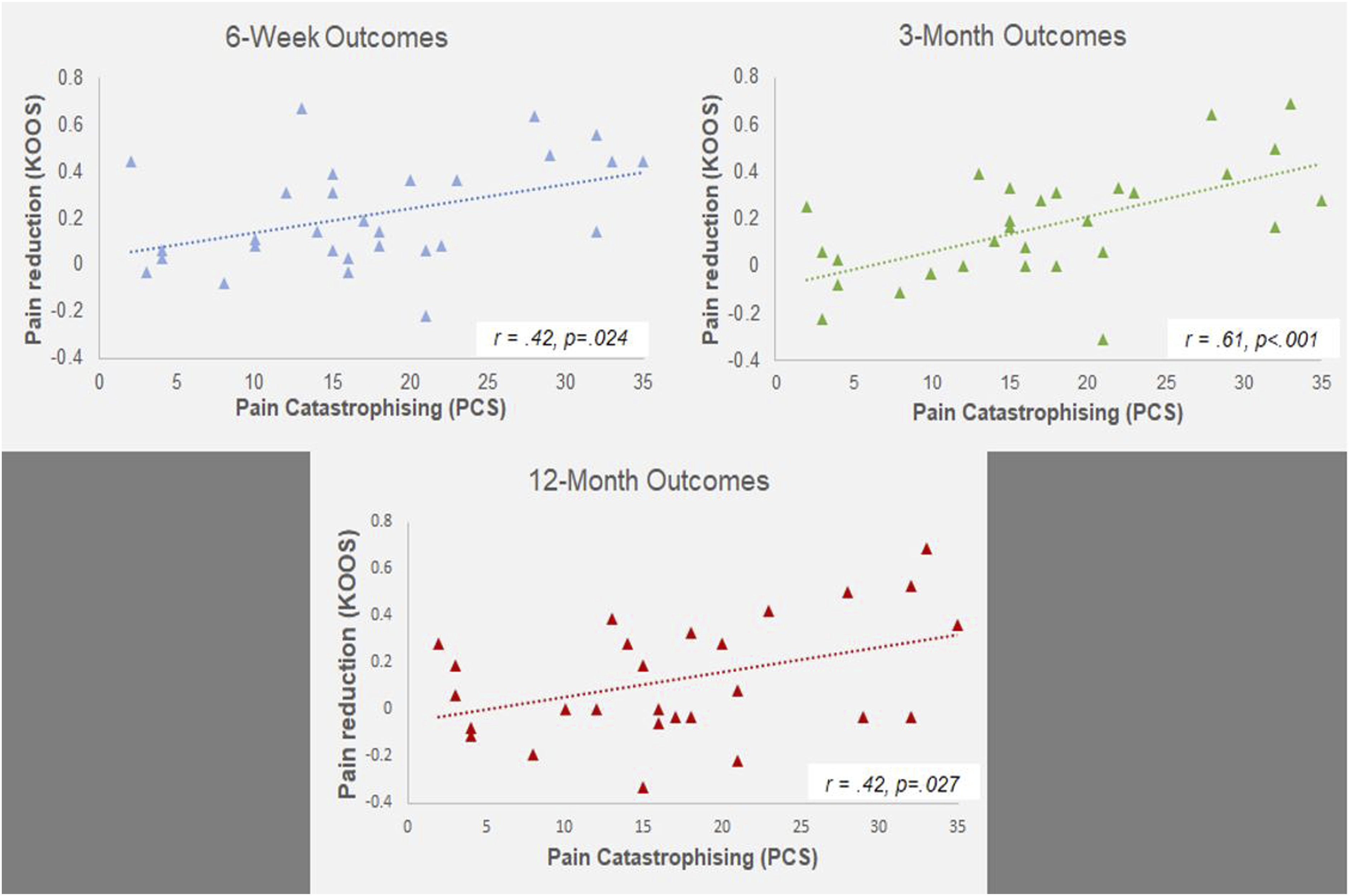
Association of pain catastrophising and functional connectivity of the dorsolateral frontal cortex
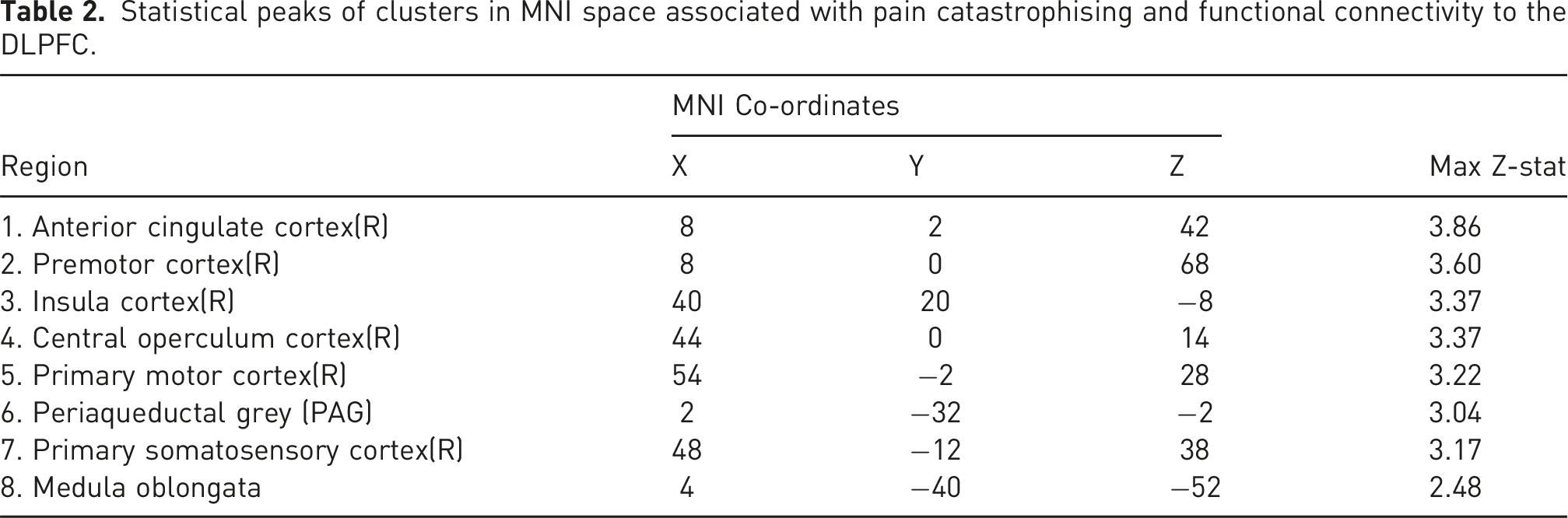
Analysis of rs-fMRI data revealed that patients with higher PCS scores were associated with higher connectivity between the dorsolateral prefrontal cortices and two clusters extending across the somatosensory, motor, premotor, insula, operculum, anterior cingulate cortices, as well as the periaqueductal grey and medulla (Figure 5; Table 2). Clusters associated with connectivity to the DLPFC and pain catastrophising in MNI space (z < 2.3) | Figure numbers relate to co-ordinates described in Table 2. Statistical peaks of clusters in MNI space associated with pain catastrophising and functional connectivity to the DLPFC.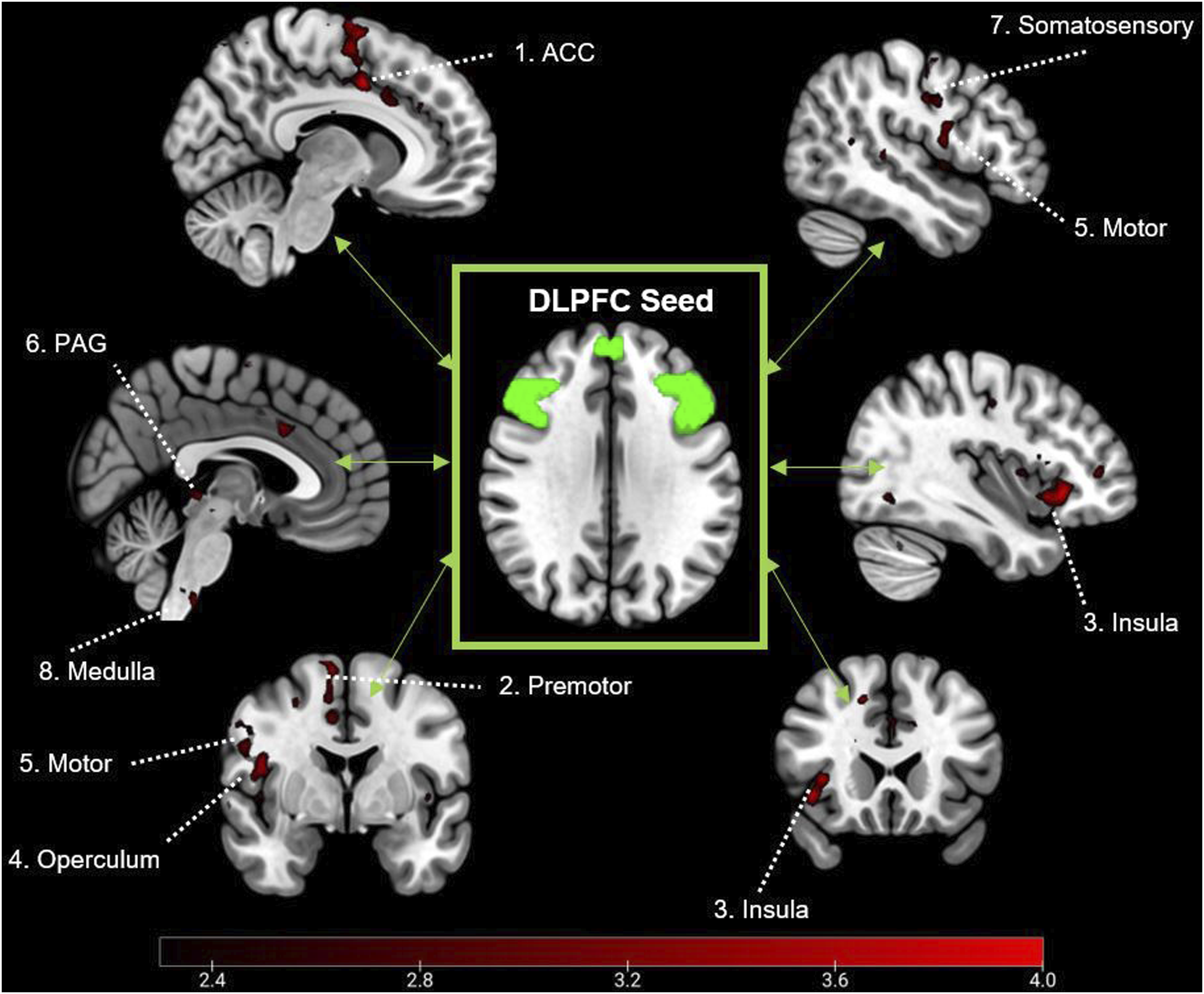
Discussion
This study investigated if pain catastrophising can be used to predict clinical outcomes following genicular embolisation for the treatment of mild-moderate osteoarthritis. We also investigated how individual differences in catastrophising were associated with variations in functional connectivity of the DLPFC, a key pain modulatory region frequently associated with the underlying mechanisms of pain catastrophising.28,31,32,35 We observed that, on average, patients experienced lasting reductions in pain as a result of the procedure. Unexpectedly, those who were high catastrophisers at baseline gained the most profound reductions in pain at all time-points (6-weeks, 3-months and 12-months). Further, individual differences in PCS scores at baseline were associated with worse pain and a myriad of negative psychological impacts at baseline, as well as variations in functional connectivity at rest. We showed that pain catastrophising was associated with higher connectivity between the DLPFC and the PAG, medulla and anterior cingulate, premotor, motor, insula, operculum and somatosensory cortices.
Pain catastrophising is described as a set of maladaptive cognitions characterised by heightened pain intensity and unpleasantness,17,56 as well as an inability to disengage from the experience of pain. 29 Interestingly, our data indicate that high catastrophisers gained the most substantial reductions in pain following embolisation. For catastrophisers, pain represents an irrepressible aversive influence which cannot be disengaged from, as supported by our finding that PCS correlates with IAP scores. At baseline, catastrophising was associated with higher osteoarthritis pain, as well as associative negative lifestyle and psychological influences, such as depression, anxiety and poor sleep. Potentially, GAE may elicit a bi-fold improvement. Firstly in a reduction in knee pain, which facilitates a reduction in catastrophic pain appraisal. Concisely, empirical literature suggests that ‘the very act of treating a disease with surgery may allow catastrophizing to decrease over time’. 25 Pain catastrophising is often described as a robust, cognitive bias, representing a stable individual difference, 17 although this position has been challenged more recently. It has been proposed that catastrophising may be a dynamic construct related to pain intensity, 57 supported by its high malleability across varying interventions for surgical patients. 25 Successful clinical treatment may theoretically alter responses to multiple items in the PCS such as ‘It’s terrible and I think it’s never going to get any better’ (item 3) or ‘there’s nothing I can do to reduce the intensity of pain’ (item 12). 19 In these instances, the entrenchment of pain may not yet have taken hold, and maladaptive cognitive biases can still be challenged via successful alleviation of pain. However, as we lack the data to investigate this mechanistically, this remains at the level of inference, and should be formally investigated.
Interestingly, catastrophising has previously been linked to poor long-term outcomes following surgical intervention for osteoarthritic pain.23,58 An important distinction between this experiment and similar previous studies, is that this study comprised solely of patients with mild-moderate osteoarthritis, not severe. Potentially representing patients with less intense and intrusive pain, or who have been living with pain for a shorter time period. Patients with severe OA, who have suffered for a longer duration from more intense and frequent pain, may be at risk of more robust and entrenched pain. Fundamentally, within a biopsychosocial framework, catastrophising is likely to represent the cognitive domain of fear-avoidance, within which, long-term exposure to this cycle facilitates pain amplification and disability based on the tendency to catastrophise. 59 Our sample, who received earlier treatment for mild-moderate OA, maybe more psychologically malleable and have more opportunity for impactful benefit, including adaptive improvements in the cognitive appraisal of pain.
Catastrophising has previously been shown to predict poor outcomes to invasive surgical procedures for knee osteoarthritis such as arthroplasty, often reserved for older patients with more severe or debilitating osteoarthritis, 6 who are especially vulnerable to catastrophising. 60 Despite this, multiple studies have reported no association and challenged this position, stating the PC may be less trait-like and robust than initially thought.15,61 One study investigating PC and recovery following total and unicompartmental joint replacement in 615 patients reported a similar finding to this study that high catastrophisers were associated with greater improvements on the Oxford Knee Score scale. 62 It should be noted that, as with our data, the higher catastrophisers had lower baseline function and higher pain at baseline, which may facilitate larger improvement potential, and contribute to the overall finding. For example, within our data, while all patients had pain at baseline, the lower catastrophisers less intense pain may have encountered a floor effect, with very little room for decrease within a 0–10 pain scale.
Another important consideration is the lack of a matched sham control alongside the experimental surgery group. The influence of placebo on pain intensity is well described and documented 63 and should temper assertive conclusions about pain reduction in GAE within a single-arm trial. This is further exacerbated due to the identification of intense placebo response for GAE specifically. 64 However, pain catastrophising itself also interacts with placebo, with high scores on the PCS facilitating greater pain reductions within placebo interventions. 65 Data collection within a trial utilising sham surgery as a placebo control is currently ongoing 48 and is required to ascertain whether the relationship between PCS and long-term outcomes remains after appropriately controlling for placebo effect.
Alongside the behavioural findings of PCS, this study also provides insight to the neural mechanisms underlying individual differences in catastrophising. Patients completed rs-fMRI scans, where no task was administered, to examine intrinsic functional connectivity. Evidence has frequently identified the DLPFC as a key region in the process of catastrophising, associated with the interpretation of pain and descending pain modulation.28,34,35 Our data indicates that catastrophising is associated with higher connectivity between the DLPFC, and multiple areas of the brain associated with sensory-discriminative processing of pain (motor, sensorimotor, premotor cortices), attentive-perception and salience of pain (insula and anterior cingulate cortices) and modulation of pain encoded within the brainstem (medulla and PAG).
The interpretation of rs-fMRI findings must be evaluated conservatively, as many direct explanations of pain processing would require event-related stimulation to empirically test. Additionally, this finding requires replication due to the relatively low sample size, 66 and this follow-up will be completed in the second phase of the study. 48 However, as catastrophising facilitates heightened salience and attentional focus towards pain, increased functional connectivity of the DLPFC with regions involved in processing of pain may represent an increased demand for endogenous modulation. These findings complement previous work by Seminowicz and Davis, 28 who found that during mild painful stimulation, PCS was associated with increases in activity in the DLPFC, as well as in the insula, motor and rostral anterior cingulate cortices, matching clusters identified from our analysis. Conversely, if the intensity of pain is increased, PCS was then associated with decreased activity in the DLPFC. The authors proposed that during intense pain, high catastrophisers may have difficulty disengaging from pain, via a lack of top-down control. This dynamic relationship between PCS and pain intensity may provide an explanation as to why PCS is associated with poor outcomes in severe OA, whereas when mild-moderate OA is treated successfully via embolisation, these patients experience a reduction in pain which they can then continue to effectively modulate.
The current study suggests that genicular arterial embolisation is an effective treatment for mild-moderate osteoarthritis pain, when evaluating longitudinal decreases in pain from baseline. Pre-surgically, pain catastrophising is associated with a range of negative co-morbidities, such as depression, anxiety and increased pain. However, our data suggests that patients who are high catastrophisers stand to gain the most benefit from successful intervention, and the PCS can predict outcomes up to 12-months post-surgically. Neural data suggests that catastrophisers have a higher functional integration of descending modulatory and pain processing regions in the brain, and that the DLPFC is a key region in this process. These results suggest that the increased attentional preoccupation with pain at baseline, facilitates a heightened requirement for pain modulation, which is supported by previous studies. 28 Importantly, these conclusions are limited by the lack of matched placebo-control, and a relatively small sample, and caution should be applied when interpreting these findings. An on-going trial aims to replicate these findings within a larger sample in a randomly controlled trial, alongside sham surgery, to evaluate embolisation alongside a suitable control. 48
Footnotes
Author note
RH has received honorarium from Crannmed. MWL is a paid consultant for Merit Medical, Crannmed, Boston Scientific, and Guerbet; has received support to attend meetings from Merit Medical and Guerbet; and is a member of the CIRSE Next Research Advisory Board. For the purpose of open access, the author has applied a Creative Commons Attribution (CC BY) licence to any arising Author Accepted Manuscript version
Ethical considerations
All procedures performed in studies involving human participants will be in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Author contributions
Funding
This study was funded by Merit Medical UK, who also provided the embolic agent used within the medical procedure. ML’s time on the grant was compensated via Merit Medical UK funding.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated by the research are available upon reasonable request to