
Abstract
Background
Chronic pain is common and associated with disruptions in quality of life (QoL) and psychosocial functioning. These issues are particularly pronounced in veterans, although data in this regard primarily come from the United States Veterans Affairs System, meaning less is known regarding veterans of other countries and regions. The present study evaluated veterans living in Northern Ireland (NI), a region with historic high rates of both chronic pain and psychosocial difficulties associated with the decades-long period of civil and military conflict preceding the 1999 armistice (the Good Friday Agreement). Unique to the Northern Ireland military operation was the initiation of Home Service battalions comprised of local recruits, a role with increased risk due to the conflict’s nature and the fact that they were serving as a military and security presence in their home region.
Methods
A cross-sectional assessment of veterans living in Northern Ireland (N = 722) provided details of service type (Home Service vs other service), current health conditions (including chronic pain), and current psychosocial functioning (including physical and mental health QoL, anxiety, depression, and post-traumatic stress disorder [PTSD] symptoms).
Results
Findings indicated that those with chronic pain had worse QoL, anxiety, depression, and PTSD. Those with chronic pain were also more likely to have served in the Home Services, be unemployed, and be receiving disability payment. Contrary to hypotheses, there was no interaction between chronic pain and service type.
Conclusions
These results extend previous work with veterans to the unique circumstances of a post-conflict military that engaged in operations within its own country and underscore the need for coordinated, efficacious interventions for co-morbid chronic pain and anxiety, depression, and PTSD.
Introduction
Chronic pain is a common and well established healthcare issue in military veterans. 1 A review of studies published between 1996 and 2013 indicated a prevalence rate from 25% to 72%, with 27% experiencing moderate or severe chronic pain. 2 More recent studies have noted that rates of high severity, high impact, or mobility affecting chronic pain range from 9% to 34% in veterans.3–7 While chronic pain is regularly co-morbid with several healthcare concerns, 8 its co-morbidity with post-traumatic stress disorder (PTSD) is of particular relevance in veterans. 1 For example, in veterans of the recent United States’ (US) conflicts, there is substantial level of co-morbidity between chronic pain and PTSD, alongside other problems such as post-concussive symptoms.9,10 In US veterans diagnosed with a diagnosed medical condition, individuals with chronic pain are at greater risk of PTSD, alcohol use disorders, and sleep problems. 11 In fact, amongst veterans with blast injuries, chronic pain was the most common condition with a prevalence of 83%, exceeding prevalence of conditions involving mental health, balance, and motor functioning. 12 Thus, the co-morbidity profile of chronic pain is substantial and involves a wide range of mental and physical health conditions.
A limitation in the veterans’ literature is that most of the available information regarding chronic pain and co-morbidity comes from a specific country and healthcare organisation, the US Veterans Affairs Healthcare System, therefore, less in known regarding veterans from other countries. 13 In the United Kingdom (UK), for example, it is not clear whether military service is a general risk factor for the commonly documented health conditions in veterans, nor is it clear whether specific military experiences such as combat and combat-related injuries represent more specific risk factors with regard to health.14,15 A recent large cohort survey of male UK veterans previously deployed to the Afghanistan conflict found that the presence of moderate or severe average weekly pain intensity was associated with a threefold increase in screening positive for post-traumatic stress, anxiety, and depression. 7 Thus, while the UK data are more limited, there is evidence suggesting that the experience of persistently significant pain represents a risk to psychological wellbeing.
Less still is known of the experiences of those who served in the UK Armed Forces during the period of civil unrest and armed conflict in Northern Ireland (NI). This conflict, commonly referred to as ‘The Troubles’, began in the 1960s when the UK military was deployed to Northern Ireland for what remains the longest operation in their history, Operation Banner, lasting just under 38 years. 16 The operation was unique in its initiation of Home Service battalions comprising individuals who were local to Northern Ireland and residing in local communities during their service-period. Thus, these individuals were deployed to their home country, where the communities within which they lived were at times hostile or threatening to military personnel. 17 This service experience may be argued to constitute prolonged and continuous exposure to potentially traumatic stressors, an experience that has been linked to increased risk of reporting PTSD symptomology and chronic pain. 18 Indeed, veterans living in Northern Ireland who served in the Home Services have been found to report a greater burden of mental ill-health relative to those who served in other conflicts, 19 highlighting the relative risk for wellbeing issues in this group.
The current study involved a secondary analysis of data collected from veterans living in Northern Ireland to investigate the experience of chronic pain, co-morbid symptoms, and to examine whether Home Service during the Troubles was associated with severity of symptoms. We used a large survey of veterans living in Northern Ireland to estimate rates of chronic pain, investigate differences in health and wellbeing based on chronic pain status and Home Service experience, and to evaluate if there was an interaction amongst these groups based on chronic pain and service type.
Methods
The study used data from the Northern Ireland Veterans’ Health and Wellbeing Study (NIVHWS), a cross-sectional survey administered to a community sample of UK veterans residing in Northern Ireland. 20 Data were collected between 2017 and 2019 and the survey consisted of self-reported functioning on standardised measures of health and wellbeing, supplemented by specific items in relation to demographic characteristics, health status, and service history. The survey was made available in online and print formats, advertised through media, local engagement events (e.g. Armed Forces Day), and veteran’s organisations. Participation was incentivised through a lottery draw awarding one of 18 vouchers valued at £150 each. All participants provided informed consent as part of participation in this study with research procedures approved by the Research Ethics Committees of Ulster University (Ref: REC/17/0031) and Queen’s University Belfast (Ref: EPS 19_156).
Measures
Chronic pain status
The NIVHWS included a section asking about the presence of current and historical health conditions. These items were answered in a dichotomous, yes/no format. The presence of chronic pain was identified by participant endorsement of one or more of the following conditions: (a) arthritis or rheumatism, (b) chronic back or neck pain, or (c) any other chronic pain.
To assess the accuracy of chronic pain classification, we examined differences in pain interference between the chronic pain classification groups using a further two items included in the survey. The first was drawn from the Veterans RAND Survey (VR-12), 21 which asked, ‘During the past 4 weeks, how much did pain interfere with your normal work (including both work outside the home and housework)?’ This question was answered using a scale ranging from 1 (not at all) to 5 (extremely). The second item was taken from the Pittsburgh Sleep Quality Index, 22 which asked, ‘How often pain had interfered with sleep in the past month’ on a 0 (not during the past month) to 3 (three or more times during the past month) scale. We hypothesised that those classified as having chronic pain would have significantly higher scores on both items in comparison to those without chronic pain, which would provide a degree of support for our method of classification.
Type of service
Experience of Home Service during Operation Banner was assessed using a dichotomous (yes/no) item: ‘Did you serve in the Ulster Defence Regiment (UDR) or the Royal Irish Home Service?’ Responses were used to assign participants to the two deployment types of Home Service deployment in Northern Ireland and all other service deployments.
Quality of life
Health-related quality of life (QoL) was assessed using the VR-12, 21 a 12-item measure of mental and physical QoL across 7 domains, including general health, physical functioning, role limitations due to physical and emotional problems, bodily pain, energy/fatigue levels, social functioning, and mental health. Responses are coded on a 5-point numerical rating scale (NRS), which are then summed and transformed using population data 23 to produce a standardised Physical Component (PCS) and Mental Component Scores (MCS) with greater scores indicative of better health. Internal consistency was high for both the PCS and MCS in the present sample (Cronbach’s α = 0.91 and 0.92, respectively)
Anxiety
Anxiety symptoms were assessed using the Generalised Anxiety Disorder Scale (GAD-7). 24 Response options are scored on a 4-point NRS, from 0 (not at all) to 4 (nearly every day), which yield a summed total score ranging from 0 to 21, with higher scores indicative of greater distress. Internal consistency was found to be high for the GAD-7 in this sample (Cronbach’s α = 0.96).
Depression
Symptoms of depression were assessed using the Patient Health Questionnaire (PHQ-9), 25 which includes nine items relating to the frequency of symptoms with responses ranging from 0 (not at all) to 3 (nearly every day). Total scores range from 0 to 27, with high score indicative of greater symptom frequency. Internal reliability was found to be high in the current sample for this measure (Cronbach’s α = 0.95).
PTSD
The PTSD Checklist for DSM-5 (PCL-5) 26 was used to assess PTSD symptoms. It consists of 20-items evaluating symptom severity over the preceding month on a five-point NRS, ranging from 0 (not at all) to 5 (extremely). Responses are summed to provide a score ranging from 0 to 80, with greater scores indicating greater symptom severity. Scale internal consistency was high in the current sample (Cronbach’s α = 0.98).
Analytic approach
First, we examined the NIVHWS response rate to examine differences between those who provided complete survey information and those who did not (i.e. provided only demographic and military service). Next, we calculated rates of chronic pain and examined differences in these same demographic and military service details between those with and without chronic pain.
We then examined our primary aim to evaluate differences in physical and psychosocial health in veterans based on chronic pain and deployment status. We hypothesised that (a) chronic pain would be associated with poorer functioning in comparison to no chronic pain and (b) military service in the Home Service battalions would be associated with worse functioning in comparison to other service. We also hypothesised that there would be an interaction effect between military service type and chronic pain status, based on an assumption of synergistic impacts between the two. These differences were initially examined via a Multivariate Analysis of Variance (MANOVA) with two independent variables, chronic pain (present/absent) and service type (Home Service/other service) and five dependent measures of physical and psychosocial health, including physical and mental health QoL, anxiety, depression, and PTSD symptoms.
Following examination of the data in relation to MANOVA’s assumptions of data distribution and homogeneity of covariance matrices, we performed the MANOVA. We planned to follow-up a significant omnibus effect with univariate ANOVAs for individual variables. We also planned effect size calculations using omega-squared (ω2), as it is increasingly clear that the more commonly used partial eta-squared (ηp2) has substantial risk of bias, particularly with the use of small samples and with small effect sizes.27–29 Omega-squared is interpreted in an equivalent manner as eta-squared: with a range of 0 to 1 and greater values indicative of more substantive effect.
As a post-hoc sensitivity analysis, we performed the same 2 (chronic pain: present/absent) × 2 MANOVA (service type: Home service/other) on the five dependent measures separately for each of the three pain conditions used to identify chronic pain. Thus, separate MANOVAs were performed for arthritis or rheumatism, chronic back or neck pain, and any other chronic pain. This analysis sought to investigate whether the pattern of results was similar to results when they were collapsed into one overarching chronic pain category.
We used the Statistical Package for Social Sciences (version 29.0; IBM Corp, 2022) for data management, calculation of descriptives, and completer/non-completer comparisons. For MANOVA analyses, we used R Studio (Build 524, RStudio Team, 2023) and ω2 effect size calculations used the formula of Troncoso-Skidmore & Thompson.29–31
Results
Demographic details
In total, 1329 individuals began the survey. Just under half (45.7%) discontinued it after providing the initial demographic and military service questions, while the remaining 722 individuals (54.3%) provided information on study measures and thus were eligible for inclusion in the current study. Comparisons between these two groups did not indicate any statistically significant differences across any of the variables tested. Specifically, there were no statistically significant differences between groups for age when joining the Armed Forces, age at discharge, or years of active service, all F < 3.3, all p > .07. Further, there were no differences in the proportions between these two groups for gender, working status, relationship status, ethnicity, highest level of education, disability registration, or service type (HS vs other). The only between group difference that approached significance was for age, F (1, 1305) = 4.0, p = .055. Descriptively, this difference was modest, as average age was 55.6 years (SD = 10.7) for the group providing chronic pain information and 54.4 years (SD = 11.8) for the group not providing this information.
Demographic details for the 722 participants who provided data were as follows. The majority were male (89.7%, 10.2% female, and 0.1% preferred not to say), White European (99.4% and 0.6% mixed ethnicity), and employed (58.0%, 29.1% retired, and 12.9% unemployed). Average age was 55.6 (SD = 10.7) at the time of survey completion. Most were married or cohabitating (72.5%, 17.3% separated/ divorced, 5.9% single/never married, 4.0% widowed, and 0.3% other). Overall, 20.8% were registered as disabled. On average, respondents were 18.6 (SD = 3.1) years old when they had first joined the Armed Forces. Approximately half of respondents served in Home Service during Operation Banner (46.1%).
Chronic pain classification
Almost three-quarters of respondents endorsed the presence of chronic pain (n = 520; 72.1%) with 391 (54.2%) reporting chronic back or neck pain, 321 (44.5%) reporting arthritis or rheumatism, and 195 (27.0%) reporting ‘any other’ chronic pain. The mean number of chronic pain types was 1.7 (SD = 0.8) with a median of 2 (range: 1 – 3). The cross-validation of the pain classification indicated significant between group differences in pain interference with work, F (1, 720) = 202.6, p
Descriptive information and group comparisons for military service and demographic details [Mean (SD) or percentage].
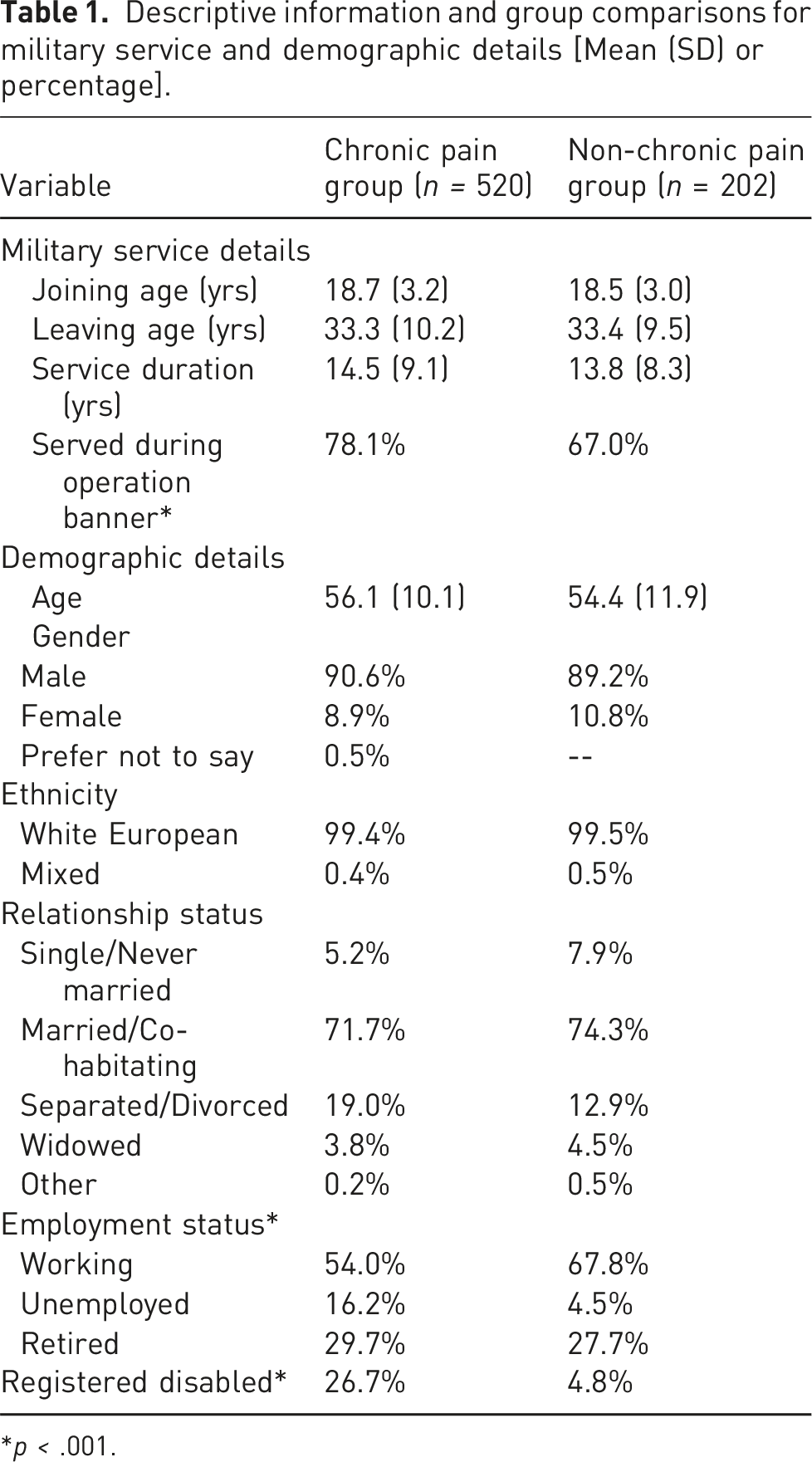
*p < .001.
There were significant differences between the chronic pain and non-chronic pain groups regarding service type (Home Service vs other), x2 (1) = 10.9, p < .001, employment status, x2 (2) = 20.6, p < .001, and disability registration, x2 (1) = 39.5, p < .001. As shown in Table 1, chronic pain was reported by approximately three-quarters, 78.1%, of those who served in the Home Service and approximately two-thirds, 67.0%, of those in other service. Rates of unemployment in those with chronic pain were almost four times higher than in those without chronic pain, 16.2% versus 4.5%, with correspondingly lower rates of current employment as well, 54.0% versus 67.8%. Rates of those in retirement were similar across the two groups, 29.7% and 27.7% for those with and without chronic pain, respectively. The proportion of those with disability registration was over five times greater in the chronic pain group, 26.7% versus 4.8%.
Between group differences
Prior to conducting the MANOVA, a number of data integrity and quality checks were performed. These analyses did not indicate any univariate or multivariate outliers. There was no indication of significant skewness or kurtosis in dependent measures, absolute values for all skewness statistics
The MANOVA results indicated significant main effects for both chronic pain, Pillai’s = 1.14, F (5, 619) = 167.3, p
Descriptive information [Mean (SD)] for measures of physical and psychosocial functioning by chronic pain status.
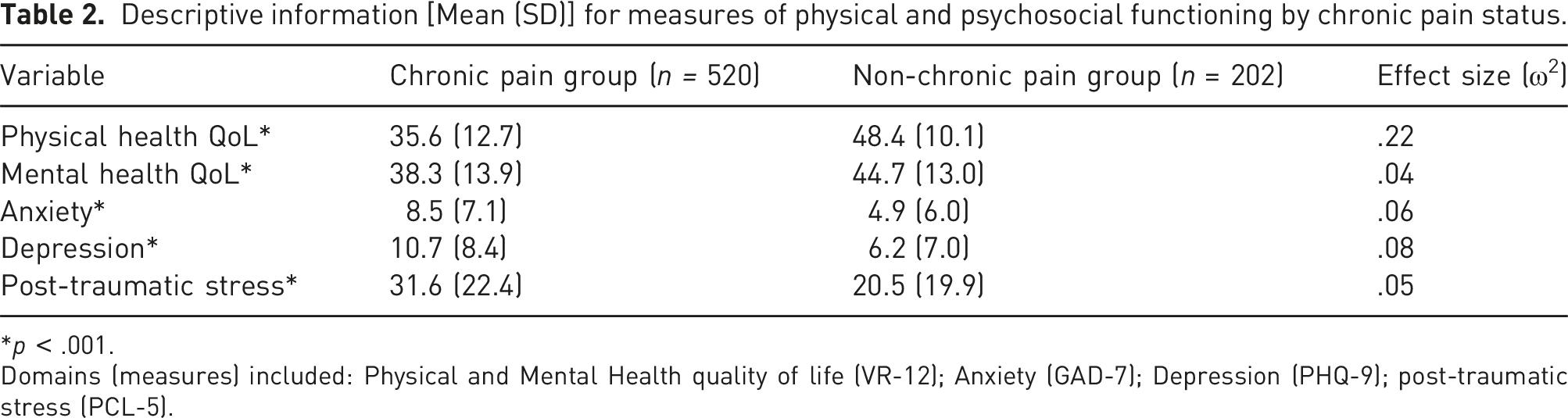
*p < .001.
Domains (measures) included: Physical and Mental Health quality of life (VR-12); Anxiety (GAD-7); Depression (PHQ-9); post-traumatic stress (PCL-5).
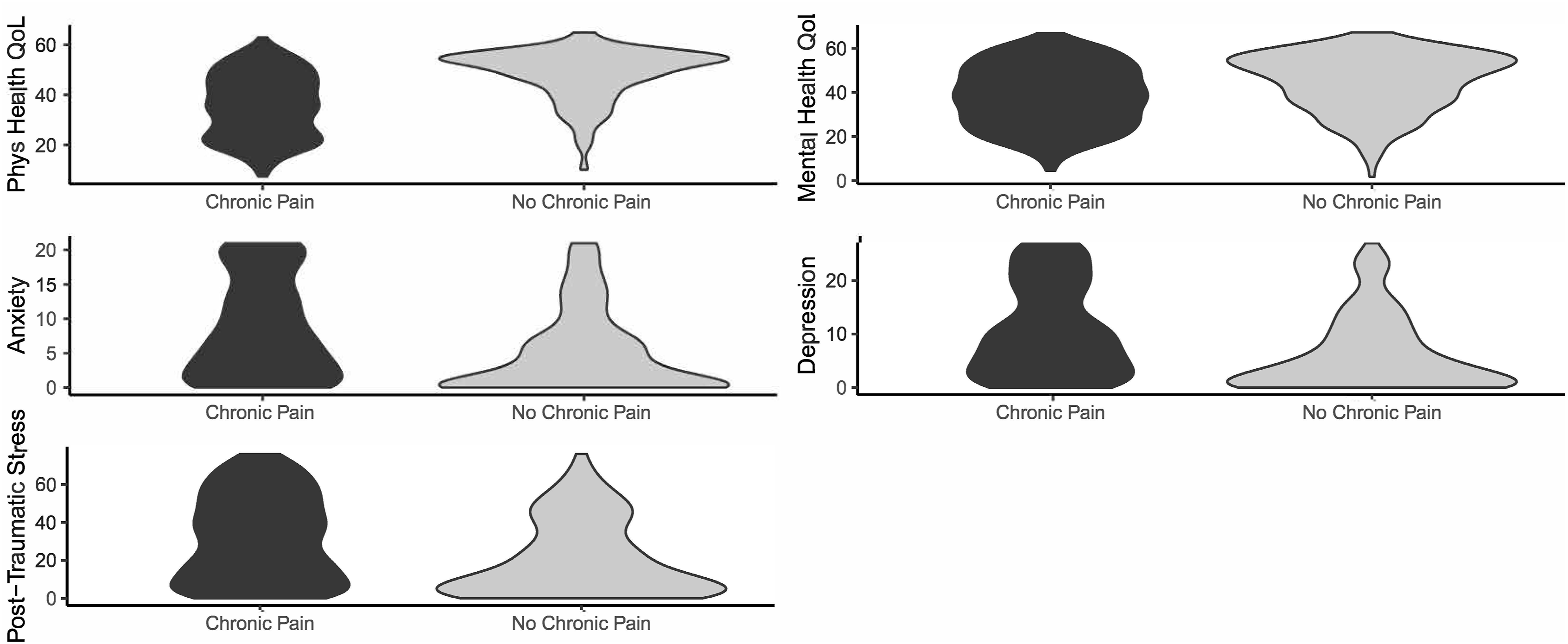
Violin plats for physical and psychosocial functioning by chronic pain status.
Descriptive information [Mean (SD)] for measures of physical and psychosocial functioning by service era.
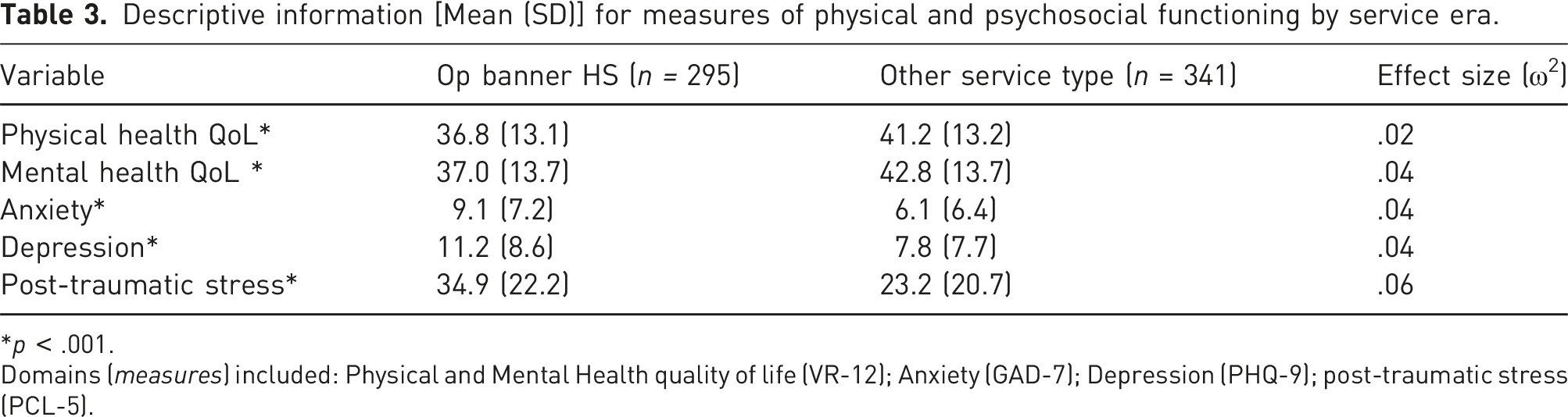
*p < .001.
Domains (measures) included: Physical and Mental Health quality of life (VR-12); Anxiety (GAD-7); Depression (PHQ-9); post-traumatic stress (PCL-5).
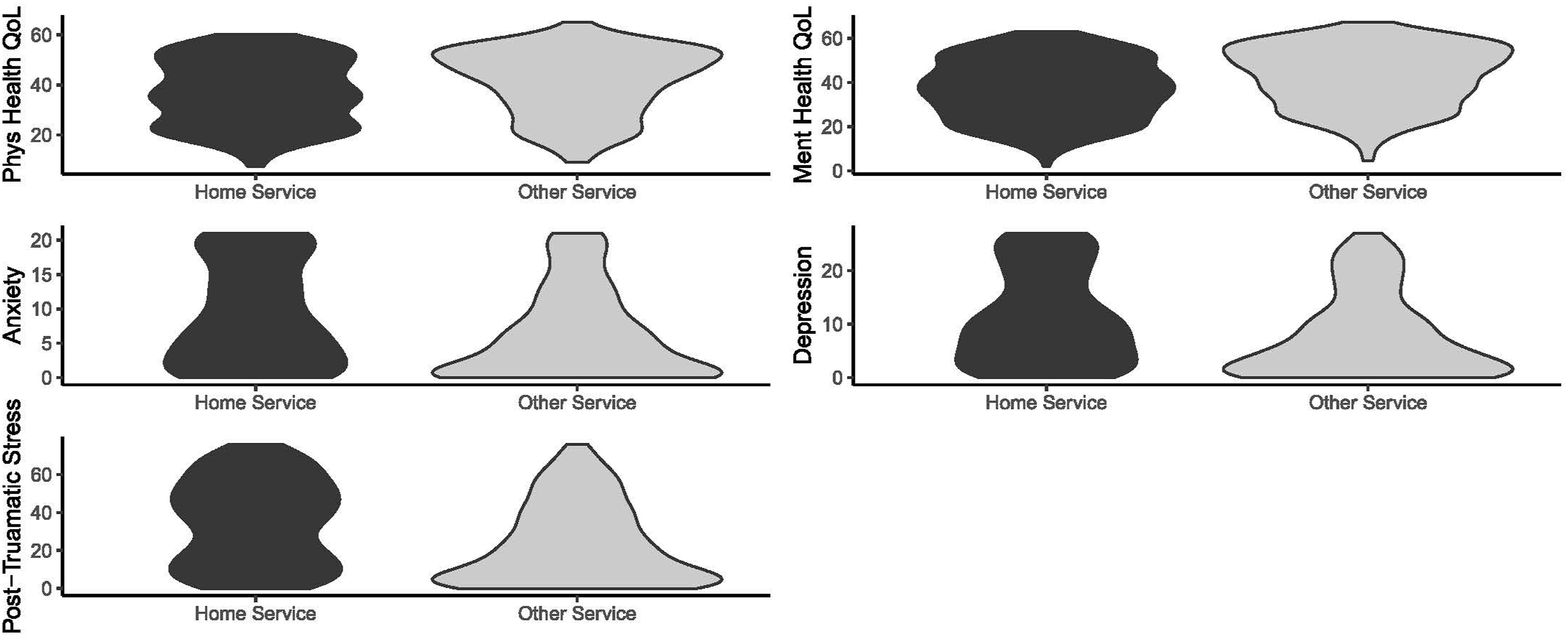
Violin plots for physical and psychosocial functioning by service.
Sensitivity analysis
When the three pain conditions used to identify chronic pain were evaluated in separate MANOVAs, the pattern of the main analysis was replicated. Specifically, main effects were present across all three analyses for pain status, range Pillai’s = 1.13 – 1.17, range F = 160.6 – 173.6, all p < .001 and service type, range Pillai’s = 0.06 – 0.07, range F = 8.1 – 9.5, all p < .001. The interaction remained not statistically significant, range Pillai’s = 0.003 – 0.01, range F = 0.4 – 1.8, all p < .11. One-way follow-up ANOVA results were also replicated in terms of the direction of difference. Full results are available upon request.
Discussion
This study investigated the association between chronic pain, deployment location, and psychosocial functioning in a sample of UK Armed Forces veterans living in Northern Ireland. Results showed that those with chronic pain were more likely to report serving as part of Operation Banner Home Service battalions, had more frequent retirement and disablement, and experienced poorer health and wellbeing across all included measures. It was further found that those who had served as part of Operation Banner Home Service reported greater physical health issues and mental ill-health relative to those who did not. The sum of this evidence highlights the importance of chronic pain and service type on the wellbeing of Northern Ireland resident veterans – particularly those who were engaged in the Home Service battalions.
These findings complement existing evidence regarding chronic pain and mental health conditions in veterans, as chronic pain prevalence rate (72%) is consistent with extant work. 2 In their review, Gauntlett-Gilbert and Wilson 13 emphasise the importance of considering service characteristics in assessment of veterans’ healthcare. For instance, it is suggested that a minimum standard should be assessment of veterans’ pain status and a determination of the relation between pain presentation and military service experiences. In the context of Northern Ireland specifically, many former service personnel may be reluctant to disclose their veterans status due to security concerns, particularly where they were part of the Home Service. 20 The current results suggest that healthcare providers need to determine not only veteran status but also gain a more nuanced picture of service type regarding engagement with the Home Service or otherwise.
These analyses highlight the importance of considering co-morbid health and wellbeing presentations, suggesting that respondents with chronic pain reported poorer functioning across all other included psychological measures in comparison to those who do not. Specifically, they reported poorer health-related QoL for physical and mental health functioning (PCS and MCS, respectively), more severe symptoms of anxiety (GAD-7), depression (PHQ-9), and PTSD (PCL-5). The finding of strong associations between chronic pain, distress, and disability is both longstanding and well established. 34 While there are a variety of theoretical perspectives that may illuminate the nature of these relations,35,36 it is clear that they are bidirectional, biopsychosocial, and multifaceted in nature, and fairly robust across time, situation, and population in the absence of intervention for both veteran and non-veteran populations.37–40
Within the study context of Northern Ireland, mental health difficulties are highly prevalent and co-morbid, 41 with over one-third of the population meeting criteria for at least one condition. 42 Of note is the relative burden of PTSD in the region, as Northern Ireland has the highest estimated prevalence in the WHO mental health surveys at 8.8%. 43 It is thought this heightened prevalence may be attributed to the widespread experience of conflict-related stressors as a result of the Troubles, 41 thus it is reasoned that those in the armed services who were necessarily exposed to such conflict-related stressors are at heightened risk as well. The frequent co-occurrence of chronic pain conditions and PTSD suggests the need for integrated and efficacious treatments that can address the key issues of both in a coordinated fashion. 9 This conclusion is also supported by a recently published survey of deployed male UK veterans, where pain severity was found to be greater in those who experienced a post-combat injury and that pain experience itself was associated with greater post-traumatic stress, anxiety, and depression symptoms. 7
The results of this study should be considered in light of the following limitations. Firstly, the survey was cross-sectional, as such temporal ordering of outcomes cannot be determined. Effectively assessing the temporal and causal links between chronic pain and mental health in veteran populations will require longitudinal data. 44 Second, it is not possible to currently establish the total population size or normative data relating to veterans of the UK Armed Forces living in NI; thus, it is impossible to know if these data are representative of the whole veteran population residing in Northern Ireland or of the experiences more broadly of the UK Armed Forces, including those who were not in the Home Service. In spite of this, the sample size of this study was fairly large and the NIVHWS survey data more broadly are concordant with veteran data from those residing in the UK,20,45 which bolsters argument for generalisability of findings. Third, it was not the original objective of the NIVHWS to conduct a specific and comprehensive measurement of chronic pain prevalence in this group. These analyses therefore made use of a composite measure comprised of endorsement of experiencing arthritis or rheumatism, chronic back or neck pain, or any other chronic pain. Responses to these questions were cross-checked with responses in relation to endorsement of functional impairment in daily tasks and sleep disturbance due to pain, which bolsters confidence in the validity of the chronic pain group membership. These results may be complimented by future investigations with use of standardised measurement of chronic pain.
Veterans of the UK Armed Forces residing in Northern Ireland have a unique history related to their military service, as the sociopolitical environment of a post-conflict society which has inhabitants from both sides of the conflict living in close proximity to one another, can contribute to fears regarding personal and familial harm. Research has reported that this situation, in addition to an increased level of exposure to traumatic events, has impacted on the physical and psychological health of this population.17,20
These results add to the body of literature substantiating the link between chronic pain and poor wellbeing among military veterans. It extends previous work, primarily from the US VA system, to a different country and its military veteran population. That being said, these data are unique in terms of the context of post-conflict Northern Ireland and indicate a strong relation between Home Service experience, the presence or absence of chronic pain, and psychological health. Future work is needed to determine adequate treatment pathways, interventions, and needs of both this unique population and veterans of other Armed Services that experience prolonged conflict in similar situations.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Forces in Mind Trust (FiMT15/0624UL/NIMH).