
Abstract
Acute postsurgical pain (APSP) is an important risk factor for pain chronification, with reports of being more intense after total knee arthroplasty (TKA) than after total hip arthroplasty (THA). Psychological variables have been associated with differences in postsurgical pain experience. This study aimed to analyse the longitudinal reciprocal association between pain and anxiety levels in patients undergoing TKA or THA, to investigate the moderator role of the type of surgery and to explore psychological mediators in the anxiety – pain association.
Patients undergoing TKA (n = 120) or THA (n = 109) were evaluated before surgery and in the acute postsurgical period (48 h postsurgery). Presurgical assessment comprised sociodemographic, pain-related and psychological variables (anxiety, depression, pain catastrophizing, self-efficacy, optimism and satisfaction with life). Postsurgical assessment focused on pain frequency, pain intensity and anxiety. Longitudinal associations were explored using cross-lagged panel models that included the indirect effect paths through possible mediators (pain catastrophizing and depression). Multigroup analyses compared TKA and THA.
In the global sample, higher APSP was predicted by higher presurgical pain and worse presurgical anxiety. Multigroup analyses revealed that worse APSP was predicted by higher presurgical anxiety in patients undergoing TKA and by higher presurgical pain in patients undergoing THA. Furthermore, there was a positive significant indirect effect of pain catastrophizing, but not depressive symptoms, in the relationship between presurgical anxiety and APSP in THA. Anxiety and APSP are differently interrelated in TKA and THA. Psychological characteristics could be managed before surgery to favour better APSP control and potentially prevent pain chronification after total joint arthroplasty.
Introduction
Total joint arthroplasties are most commonly performed due to severe osteoarthritis, aiming to restore structural integrity and functionality of an affected joint. 1 Acute postsurgical pain (APSP) is common after these interventions due to local injury and inflammation, 2 being an expected and adaptive response. However, high levels of APSP are associated with increased suffering, perioperative complications, functional impairment, recovery delay and increased morbidity, making its effective control of paramount importance.3–5 Higher acute pain levels hinder active involvement in rehabilitation activities and may lead to poorer surgical outcomes. 6 APSP has also been extensively associated with future pain chronification and is thus a relevant therapeutic target to prevent chronic postsurgical pain. 5 Over the last decades, there have been considerable advances in understanding pain pathophysiology, developing modern analgesic techniques and publishing updated guidelines. However, effective acute pain control after surgery is still a challenge, with different surveys showing that a significant proportion of patients experience severe pain in the postoperative period.7–9 One plausible explanation for insufficient pain control is the variability in patient characteristics that may impact APSP, 10 such as presurgical pain or psychological characteristics.11,12 Thus, a biopsychosocial perspective of pain is crucial to optimise APSP control, 13 underlining the relevance of investigating factors that may influence it, namely, potentially modifiable characteristics such as psychological variables. In fact, variables such as anxiety, depression, pain catastrophizing and optimism can modulate (exacerbate or inhibit) pain perception14,15 and have been identified as relevant predictors of APSP after different types of surgery.11,12,16
In this scope, anxiety has been pointed as a relevant symptom to consider both before and after surgery. Indeed, clinical guidelines target anxiety as a potentially modifiable risk factor for worst surgical outcomes.17,18 Moreover, heightened levels of presurgical anxiety can progress to postsurgical anxiety. 19 After surgery, anxiety is associated with APSP intensity, analgesia requirements, quality of recovery and wound healing20–22 Nonetheless, the potentially bidirectional relationship between these variables should be kept in mind. While anxiety may influence pain, it is also possible that higher pain intensity leads to increased anxiety. 23
The relevance of psychological factors has also been shown specifically in orthopaedic surgeries, with pain catastrophizing, negative mood and optimism being recognised as predictors of APSP after total knee arthroplasty (TKA)24–27 and total hip arthroplasty (THA). 28 Interestingly, one study even identified optimism as the most relevant predictor of APSP in a mixed TKA/THA sample, hinting at the relevance of positive psychological variables in this field. 29 However, most studies of psychological predictors of acute post arthroplasty pain focus on TKA, with few reporting data separately for THA.30,31 This is a significant literature gap since there are well-documented differences in the outcomes of TKA and THA. During the acute postsurgical period, TKA patients experience more pain than THA patients,32–34 though the reasons for this are not well-understood. 34 It is conceivable that psychological variables, along with other demographic, surgical and clinical factors, may help explain this variability. 30
There is a need to further understand APSP after arthroplasty and to explore if conclusions derived from TKA can be generalised to other types of arthroplasties (e.g. THA). This study resorts to a cross-lagged panel model approach to describe the bidirectional relationships between variables at pre and postsurgical time points. 35 Thus, the aims of this work were: (a) to analyse the longitudinal reciprocal association between pain and anxiety levels in patients undergoing TKA or THA, (b) to investigate if there is a moderator role of the type of surgery and (c) to explore psychological mediators in the anxiety – pain association.
Methods
Participants and procedure
Recruitment took place at the Orthopedics Unit of Hospital de Braga (Portugal), from June 2021 to December 2022. Patients were approached during a presurgical appointment with a specialist nurse and consecutively invited to participate if they met the inclusion criteria: (a) age ≥ 50 years old; (b) scheduled unilateral total joint arthroplasty due to osteoarthritis of the knee or hip; and (c) ability to understand written information and give informed consent. Exclusion criteria were: (a) revision surgery; (b) severe neurologic, psychiatric or organic diseases; and (c) contralateral knee or hip arthroplasty in the previous 6 months. In case of acceptance, the participants gave written informed consent before baseline assessment (T0, presurgical). Postsurgical assessment was conducted during the hospital stay, at 48 h postsurgery (T1).
Two hundred and 49 patients accepted to participate and were assessed before surgery. From the initial sample, six patients had their surgery postponed and 14 were excluded from the analyses (10 could not be assessed at 48 h, one had a subtrochanteric osteotomy and three had unicompartmental knee arthroplasty). Thus, the final sample included 229 participants.
All surgeries were performed by orthopaedic surgeons from the Orthopedics Unit of Hospital de Braga, who determined the appropriate surgical procedures for each patient. There were no research-related changes introduced to routine surgical or anaesthetic practices. Details concerning these procedures can be found in Supplemental Material 1.
Ethical approval was granted by the Ethics Committee from Hospital de Braga and Ethics Committee for Research in Life and Health Sciences from the University of Minho. All procedures followed international ethical guidelines for clinical studies involving humans.
Measures
Presurgical assessment (T0)
- Sociodemographic and clinical questionnaire: sociodemographic information included data concerning age, sex, education, marital status and employment. The clinical section evaluated weight, height, comorbidities and pain characteristics (e.g. duration, other painful sites). - American Society of Anesthesiologists physical status classification (ASA score)
36
: this information was retrieved from the clinical records to inform about pre-anaesthesia medical comorbidities. Each patient’s score is classified as ASA I (normal healthy patient), ASA II (patient with mild systemic disease), ASA III (severe systemic disease), ASA IV (life-threatening severe systemic disease), ASA V (moribund patient) or ASA VI (brain-dead patient). - Brief Pain Inventory (BPI)
37
: evaluates pain intensity on an 11-point numerical rating scale (NRS; 0 = No pain; 10 = Worst pain imaginable). In this study, pre and postsurgical pain intensity at the affected joint were calculated by computing the mean score of pain ‘at its worst’ and ‘on the average’. At baseline, patients were asked about worst and average pain in the previous week. At 48h, the recall period was altered to encompass the acute period. - Western Ontario and McMaster Osteoarthritis Index (WOMAC)
38
: disability was evaluated using a specific subscale from WOMAC (17 items). The subscale score is the sum of all items, with higher scores indicating more disability (range: 0-68). - Coping Strategies Questionnaire-Revised (CSQ-R)
39
: pain catastrophizing was assessed with the corresponding six item subscale from the CSQ-R. The total score is the mean value of all answers (range: 1-5),
29
with higher values indicating greater pain catastrophizing. - Hospital Anxiety and Depression Scale (HADS)
40
: evaluates symptoms of general anxiety and depression in patients with medical illnesses.
41
The questionnaire is comprised of two subscales (anxiety and depression) with seven items each, answered according to the previous week. When administered 48h after surgery, the anxiety items were answered considering the acute period. Each subscale scores range from 0 to 21, with higher scores representing higher symptomatology. - Pain Self-Efficacy Questionnaire (PSEQ)
42
: evaluates confidence to engage in various activities of daily living, despite pain. The total score is the sum of the 10 items and varies from 0 to 60, with higher scores translating stronger self-efficacy beliefs. - Life Orientation Test-Revised (LOT-R)
43
: derives an optimism score that is the sum of six items. The score may range from 0 to 24, with higher values translating more optimistic views. - Satisfaction with Life Scale (SWLS)
44
: indicates the level of satisfaction with life through five items that derive a total score (range: 1-25). Higher scores indicate higher life satisfaction.
Postsurgical assessment (T1)
The assessment 48 h after surgery included pain frequency, pain intensity (BPI) and anxiety (HADS subscale). Pain frequency was assessed using the McGill Pain Questionnaire (MPQ), 45 which groups pain as continuous (steady, constant), rhythmic (periodic, intermittent) or brief (momentary, transient). Additional surgical information was retrieved from medical records, namely, the type of anaesthesia, surgical approach, intra and postoperative analgesics.
Statistical analyses
Participants’ characteristics are expressed as absolute and relative frequencies for categorical data (n, %) or mean and standard deviation for continuous variables (M ± SD). Only participants with complete data were included in the analyses (missing cases deleted listwise). The distribution properties of continuous variables were analysed through skewness (Sk) and kurtosis (Ku). Normality was assumed if Sk ± 2 and Ku ± 7 46 and was guaranteed for all variables. Differences between patients undergoing TKA and THA were explored through independent samples t-tests or chi-square (χ2) tests, as appropriate. Paired samples t-tests analysed the pre to postsurgery differences in pain and anxiety levels. Effect size measures (Cohen’s d and Phy coefficient, ϕ) were computed to illustrate the meaningfulness of the results. The association of baseline (sociodemographic and psychological) variables with pain and anxiety levels was analysed through Pearson’s correlation coefficient. The analyses were performed using the IBM Statistical Package for the Social Sciences (SPSS), version 26 (Chicago, IL, USA). Statistical significance was set at p < .05.
The longitudinal reciprocal relationship between anxiety levels and pain was explored through autoregressive cross-lagged panel models (CLPM). CLPM allows for simultaneous analysis of the multiple relationships specified in the models. A depiction of CLPM for this study can be seen in Figure 1. The model includes two constructs (anxiety and pain), assessed at two time points (before and after surgery), and the cross-lagged relationships between constructs and time points (solid lines in Figure 1). CLPM also controls for same-moment correlations (dotted lines) and autoregressive effects (stability over time, dashed lines).
35
Age and sex were included as covariates in all models. The strength of the relationships was compared through standardised beta coefficients (β) and associated 95% confidence intervals (CI). Firstly, a CLPM was fit to the global study sample. Then, multigroup analysis was used to explore the moderator role of the type of surgery on the established relationships. Specific differences between groups were analysed through the associated critical ratios (CR). This calculation assumes a normal distribution of data, with a value of 1.96 indicating two-sided significance at the 5% level. When CR >1.96 for a given path, we can assume statistically significant differences. Illustration of the cross-lagged panel model used in this study. The solid lines represent the cross-lagged relationships between constructs and time points. Cross-sectional correlations are represented by dotted lines and autoregressive effects by dashed lines.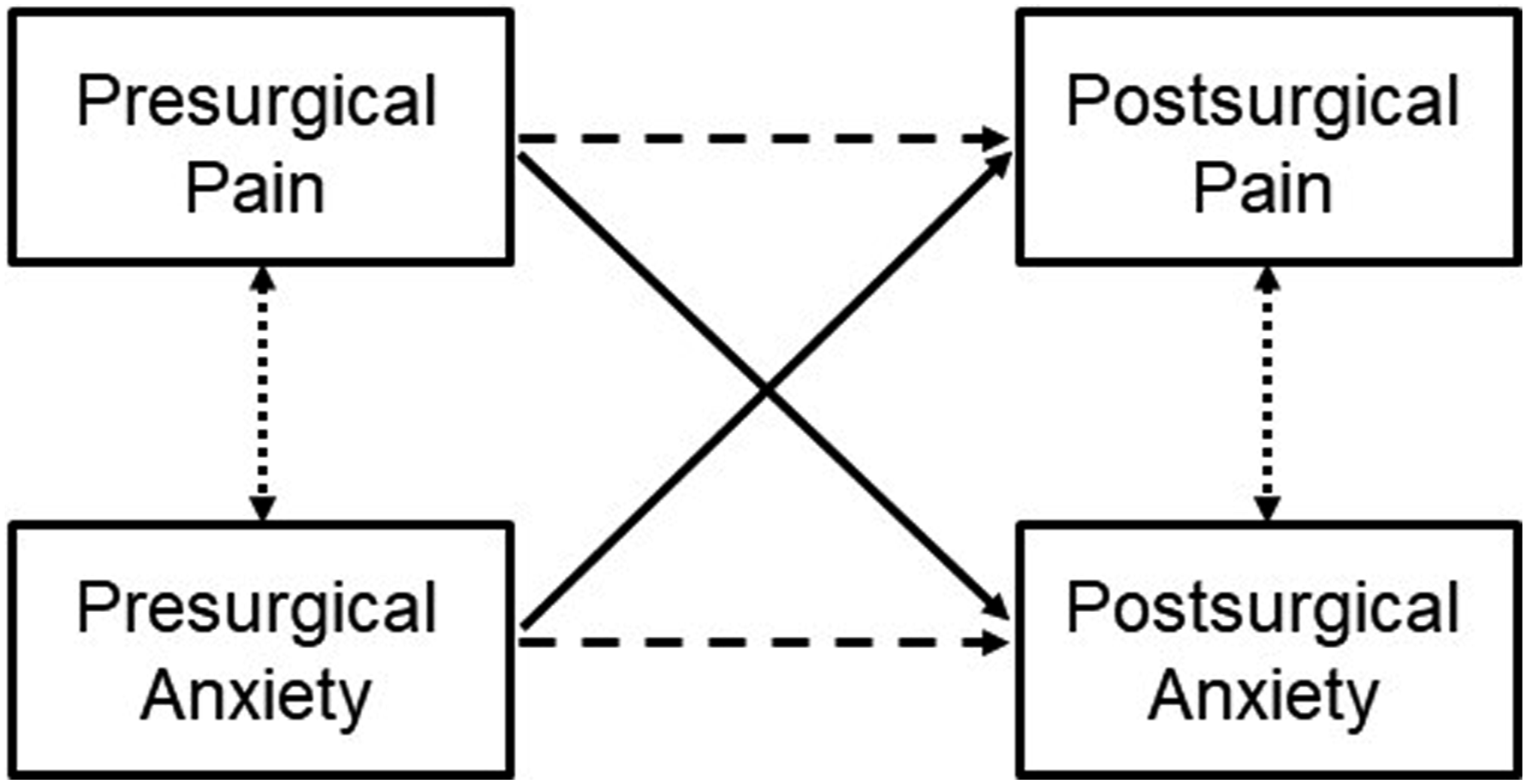
Considering the association of psychological characteristics with anxiety and pain, we explored if they could mediate the association between presurgical anxiety and postsurgical pain that was revealed by the initial CLPM. Through mediation, it is possible to analyse if a given intervening variable (mediator, M) explains the mechanisms through which an independent variable (antecedent, X) causes an effect on a dependent variable (outcome, Y). A mediation model illustrates the different paths through which X can influence Y. This can happen through a direct effect, without intervention from M (path c’) or through an indirect effect from X to Y, passing through M (paths a x b).
47
The combination of direct and indirect effects results in the total effects (path c). An illustration of mediation is shown in Figure 2. The indirect effect paths were added to the CLPM previously run without the mediator, for analysis purposes. The variables selected as potential mediators were those significantly associated with presurgical anxiety and postsurgical pain in previous correlation analyses (Pearson’s coefficient). Mediation tests were conducted based on 10 000 bootstrap samples to reduce sample variation.
47
The results are reported for a 95% bias-corrected CI. Multigroup analyses by type of surgery were again used to investigate their role in the mediation results. CLPM and mediation models were fitted using maximum likelihood estimation in IBM SPSS AMOS, version 25. Illustration of a mediation model depicting the paths through which a mediator (M) influences the effect of the independent variable (X) on the outcome (Y). The arrows represent relationships between variables. Path c’ is the direct effect from X to Y, path axb is the indirect effect from X to Y, passing through M and path c accounts for both the direct and indirect effects.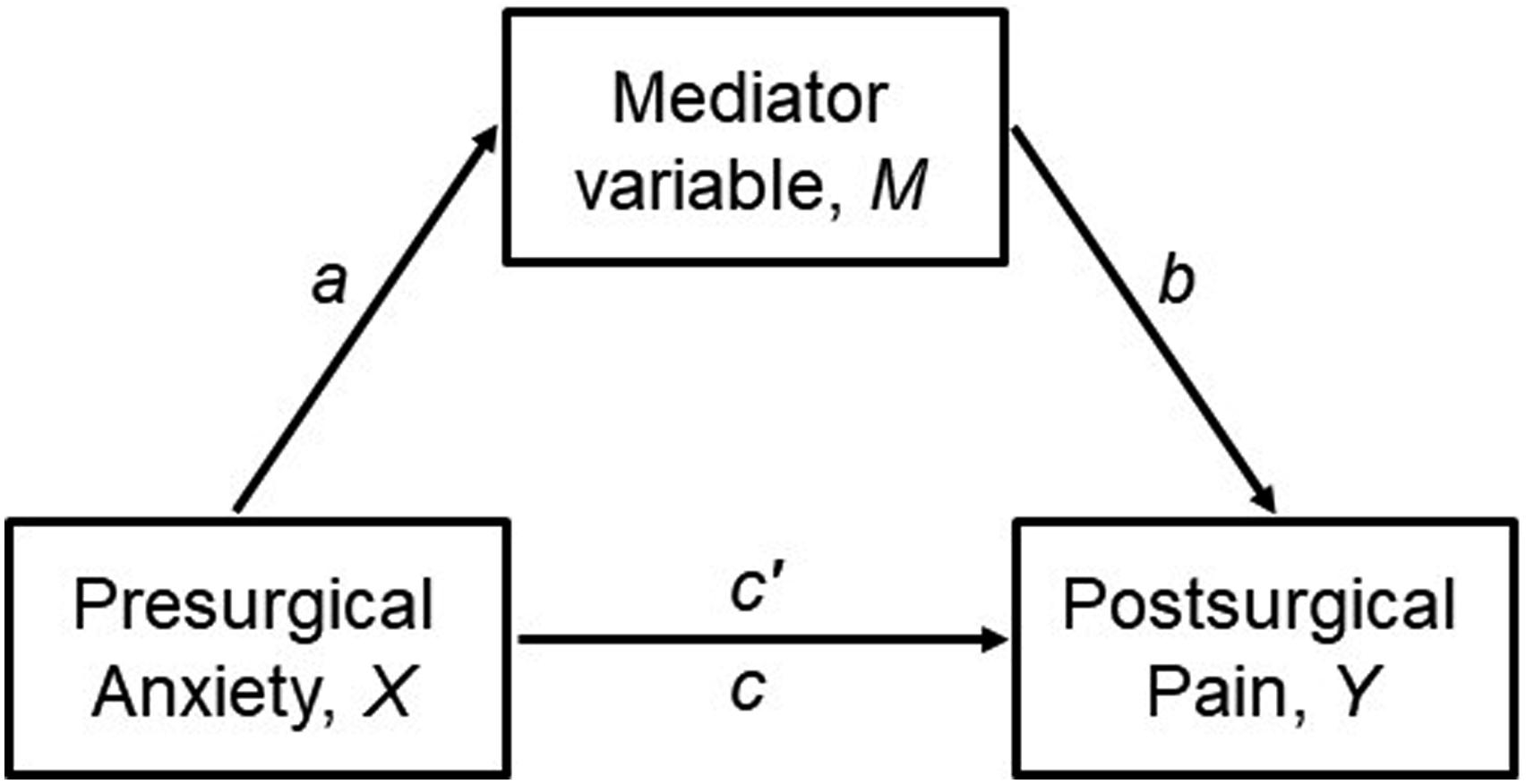
The overall goodness-of-fit for the models was evaluated considering the following indices and thresholds: chi-square (p > .05), root mean square error of approximation (RMSEA <0.06) and comparative fit index (CFI >0.95). 48 Sample size is within the recommended 10:1 ratio of cases to parameters. 49 For the CLPM with indirect effect paths (20 parameters), 200 participants would be required. Thus, the study was well-powered to detect statistically significant effects.
To evaluate the longitudinal invariance of the anxiety assessment (HADS subscale), we used IBM SPSS AMOS v. 25 to specify two latent variables that correspond to anxiety assessment at T0 (baseline) and T1 (acute postsurgical period) (Supplemental Material 2). The model was estimated without any constraints to test if the factor structure is similar between time points (configural invariance). The analysis of the model’s fit indices, particularly CFI and RMSEA, shows that anxiety assessment has adequate longitudinal measurement invariance (χ2 (134) = 221.4, p < .001, CFI = 0.912, RMSEA = 0.054).
Results
Comparison of pre and postsurgical characteristics of TKA and THA patients
Description of pre and postsurgical characteristics and between-group differences.
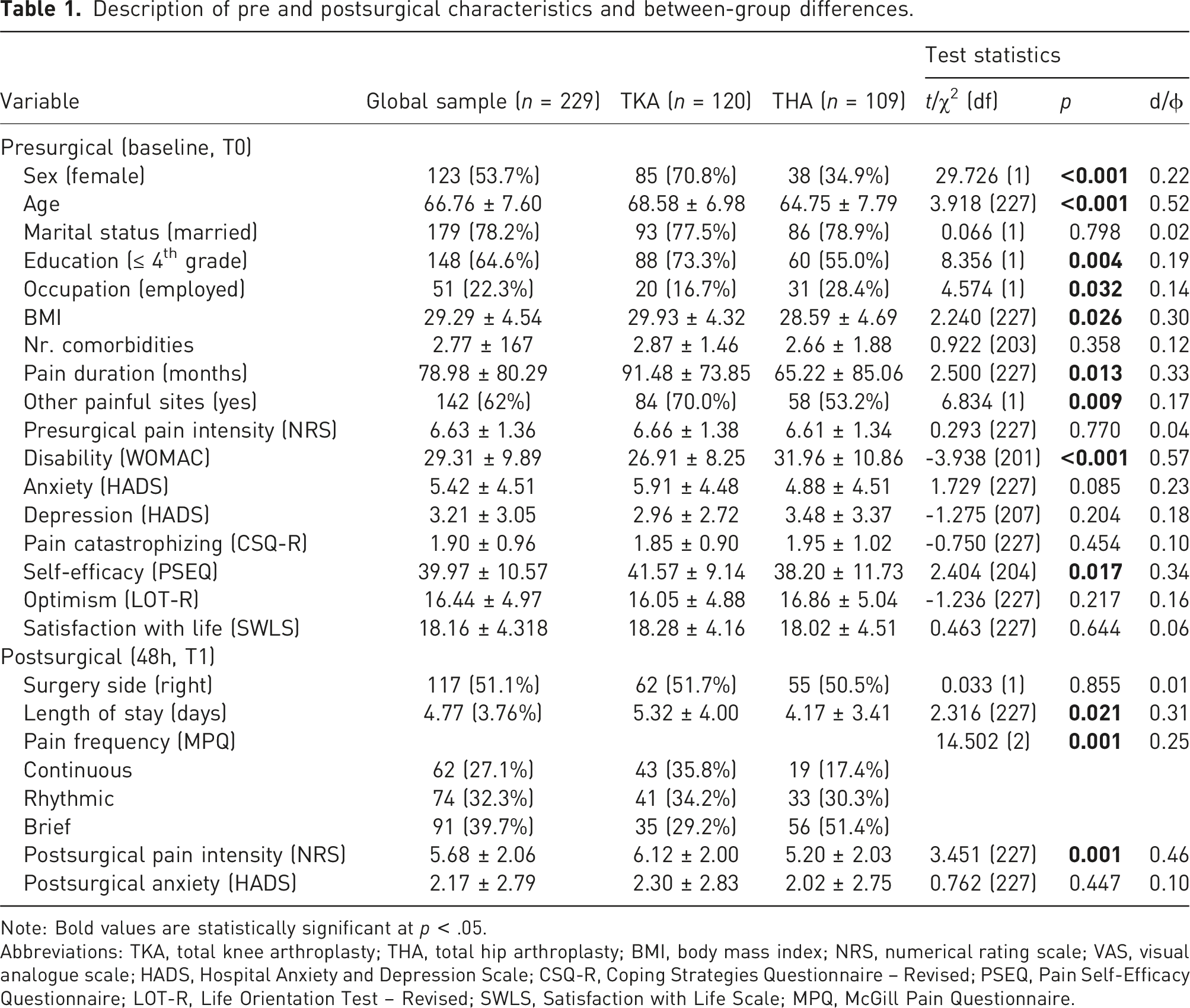
Note: Bold values are statistically significant at p < .05.
Abbreviations: TKA, total knee arthroplasty; THA, total hip arthroplasty; BMI, body mass index; NRS, numerical rating scale; VAS, visual analogue scale; HADS, Hospital Anxiety and Depression Scale; CSQ-R, Coping Strategies Questionnaire – Revised; PSEQ, Pain Self-Efficacy Questionnaire; LOT-R, Life Orientation Test – Revised; SWLS, Satisfaction with Life Scale; MPQ, McGill Pain Questionnaire.
There were statistically significant differences between patients undergoing TKA and THA in terms of sex (χ2 (1) = 29.7, p < .001), age (t (227) = 3.9, p < .001), education (χ2 (1) = 8.4, p = .004), occupation (χ2 (1) = 4.6, p = .032), body mass index (BMI) (t (227) = 2.2, p = .026), presurgical pain duration (t (227) = 2.5, p = .013), presence of other painful sites (χ2 (1) = 6.8, p = .009), disability (t (201) = -3.9, p < .001), self-efficacy (t (204) = 2.4, p = .017), length of stay (t (227) = 2.3, p = .021), postsurgical pain frequency (χ2 (2) = 14.5, p = .001) and intensity (t (227) = 3.5, p = .001. More women than men underwent knee surgery. TKA patients were older, with lower education levels, less often employed and had higher BMI. More patients with gonarthrosis than coxarthrosis reported other painful sites, they had longer pain duration, lower disability and higher pain self-efficacy levels. Patients who had TKA stayed more days at the hospital on average than THA, reported more continuous pain and had higher acute pain intensity. Paired samples t-tests (not shown) confirmed that pain and anxiety levels were significantly higher at baseline than at 48h (pain intensity: t (228) = 6.5, p < .011; anxiety: t (228) = 11.2, p < .001).
Relationship of sex, age and baseline psychological characteristics with pre and postsurgical pain and anxiety levels
Relationship of baseline variables with pre and postsurgical pain and anxiety levels (global sample).
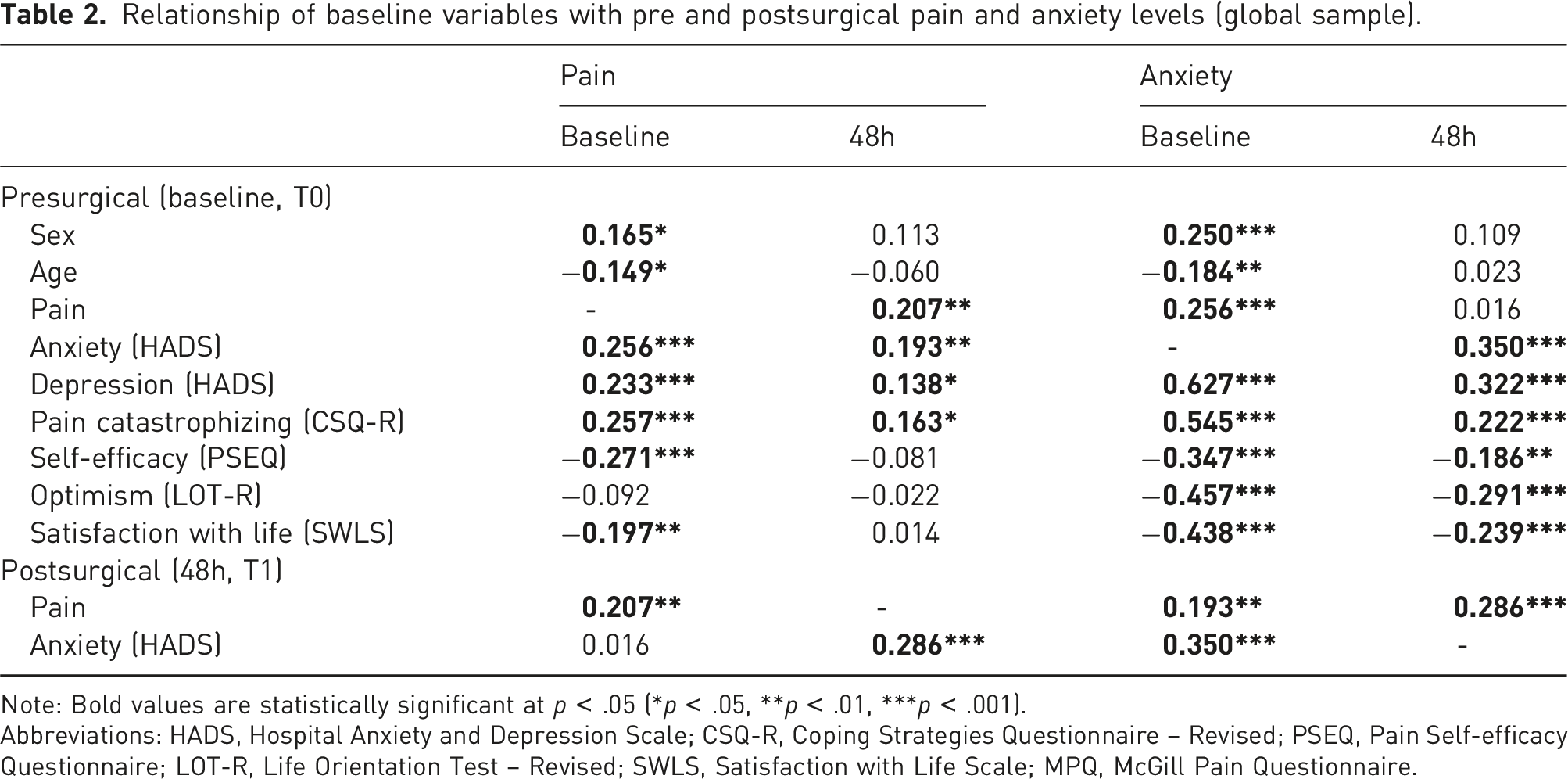
Note: Bold values are statistically significant at p < .05 (*p < .05, **p < .01, ***p < .001).
Abbreviations: HADS, Hospital Anxiety and Depression Scale; CSQ-R, Coping Strategies Questionnaire – Revised; PSEQ, Pain Self-efficacy Questionnaire; LOT-R, Life Orientation Test – Revised; SWLS, Satisfaction with Life Scale; MPQ, McGill Pain Questionnaire.
All baseline psychological variables were significantly associated with presurgical anxiety levels (depression: r = 0.627, p < .001; pain catastrophizing: r = 0.545, p < .001; pain self-efficacy: r = −0.374, p < .001; optimism: r = −0.457, p < .001 and satisfaction with life: r = −0.438, p < .001) and with postsurgical anxiety levels (depression: r = 0.322, p < .001; pain catastrophizing: r = 0.222, p < .001, pain self-efficacy: r = −0.186, p = .005; optimism: r = −0.291, p < .001 and satisfaction with life: r = −0.239, p < .001). Higher depression symptomatology and pain catastrophizing, and lower pain self-efficacy, optimism and satisfaction with life were associated with more anxiety symptomatology at both time points.
Longitudinal reciprocal relationships between anxiety and pain
Standardised estimates for CLPM of relationships between anxiety levels and surgical pain, and multigroup comparisons.
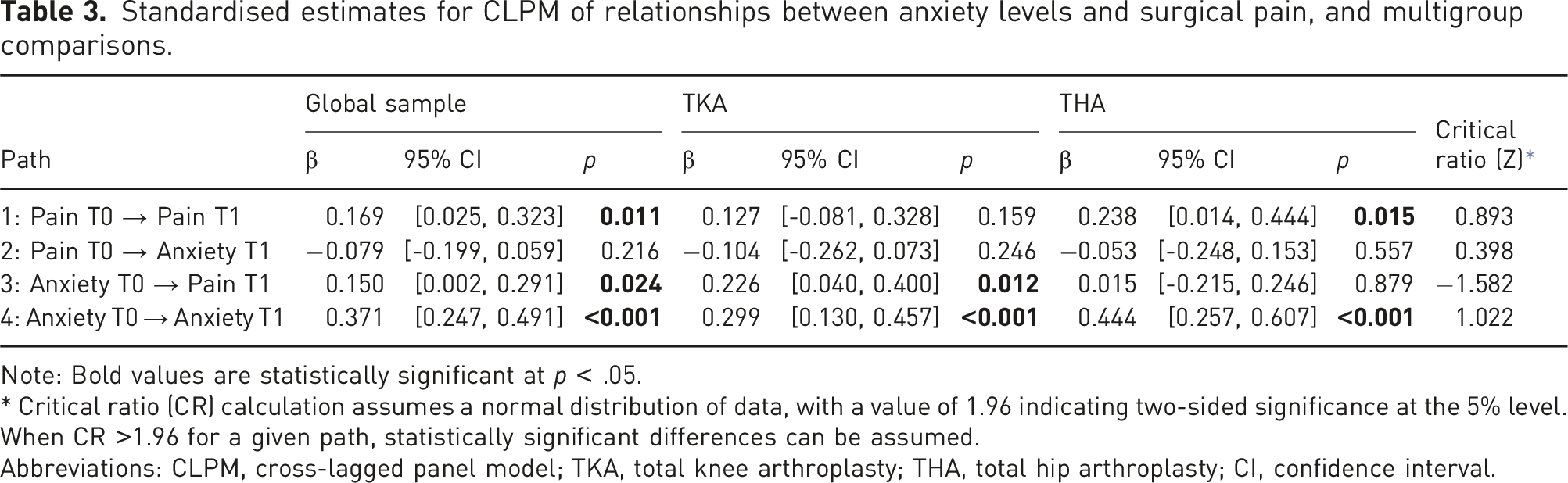
Note: Bold values are statistically significant at p < .05.
* Critical ratio (CR) calculation assumes a normal distribution of data, with a value of 1.96 indicating two-sided significance at the 5% level. When CR >1.96 for a given path, statistically significant differences can be assumed.
Abbreviations: CLPM, cross-lagged panel model; TKA, total knee arthroplasty; THA, total hip arthroplasty; CI, confidence interval.
Model fit statistics for the CLPM of relationships between anxiety levels and surgical pain.
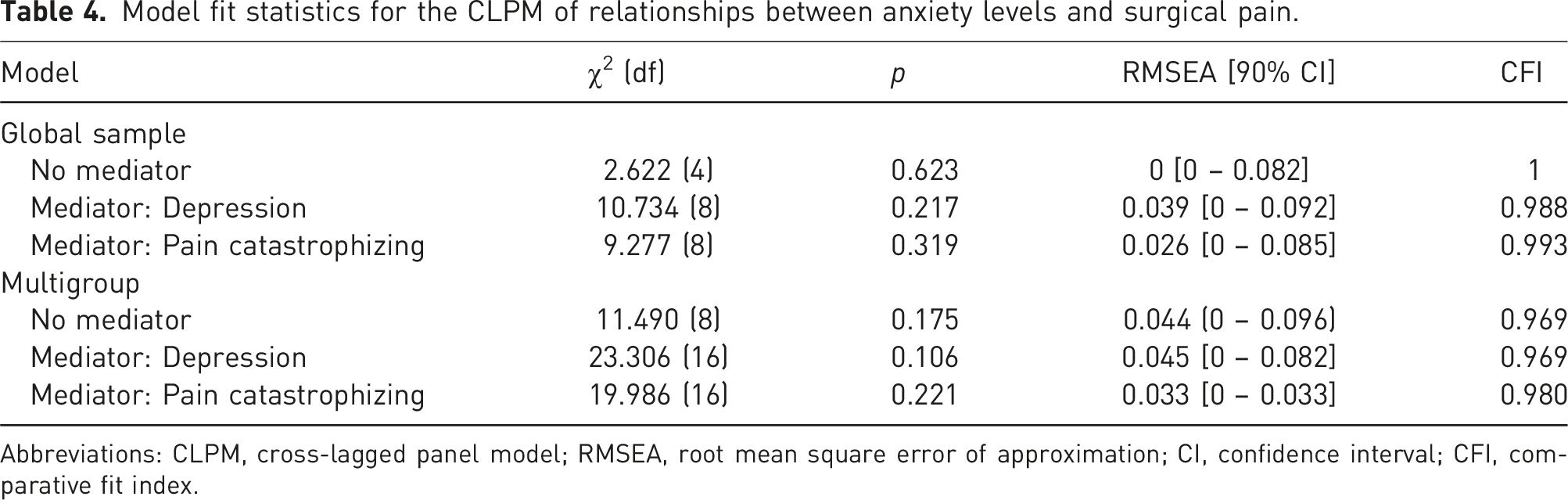
Abbreviations: CLPM, cross-lagged panel model; RMSEA, root mean square error of approximation; CI, confidence interval; CFI, comparative fit index.
The CLPM is depicted in Figure 3. For the global sample, there were statistically significant associations in three of the analysed paths (paths 1, 3 and 4). Baseline pain significantly predicted 48h pain (path 1: β = 0.17, p = .011) but was not associated with anxiety levels at 48h (path 2: β = −0.08, p = .216). On the other hand, baseline anxiety intensity predicted both 48h pain (path 3: β = 0.15, p = .024) and 48h anxiety levels (path 4: β = 0.37, p < .001). In the multigroup analyses, baseline pain continued to show a non-significant association with 48h anxiety levels in both surgeries (path 2, TKA: β = −0.10, p = .246; THA: β = −0.05, p = .557), while baseline anxiety predicted 48h anxiety intensity in both surgeries (path 4, TKA: β = 0.37, p < .001; THA: β = 0.44, p < .001). Path 1 (baseline pain predicting 48h pain) was only statistically significant in THA (β = 0.24, p = .015) and path 3 (baseline anxiety predicting 48h pain) was only statistically significant in TKA patients (β = 0.23, p = .012). That is, postsurgical pain was predicted by presurgical pain in patients undergoing THA and by presurgical anxiety levels in patients undergoing TKA. However, the critical differences ratios did not identify statistically significant differences in these paths, between the two groups (all p > .05; |Z values|<1.96). The full CLPM with standard estimates can be found in Supplemental Material 3. Illustration of the cross-lagged panel model between anxiety and pain for the global sample (1), TKA (2) and THA (3). The solid lines represent the cross-lagged relationships between constructs and time points. Cross-sectional correlations are represented by dotted lines and autoregressive effects by dashed lines. For simplicity, the included covariates and error terms are not depicted. Bold values are statistically significant at p < .05 (***p < .001, **p < .01, *p < .05).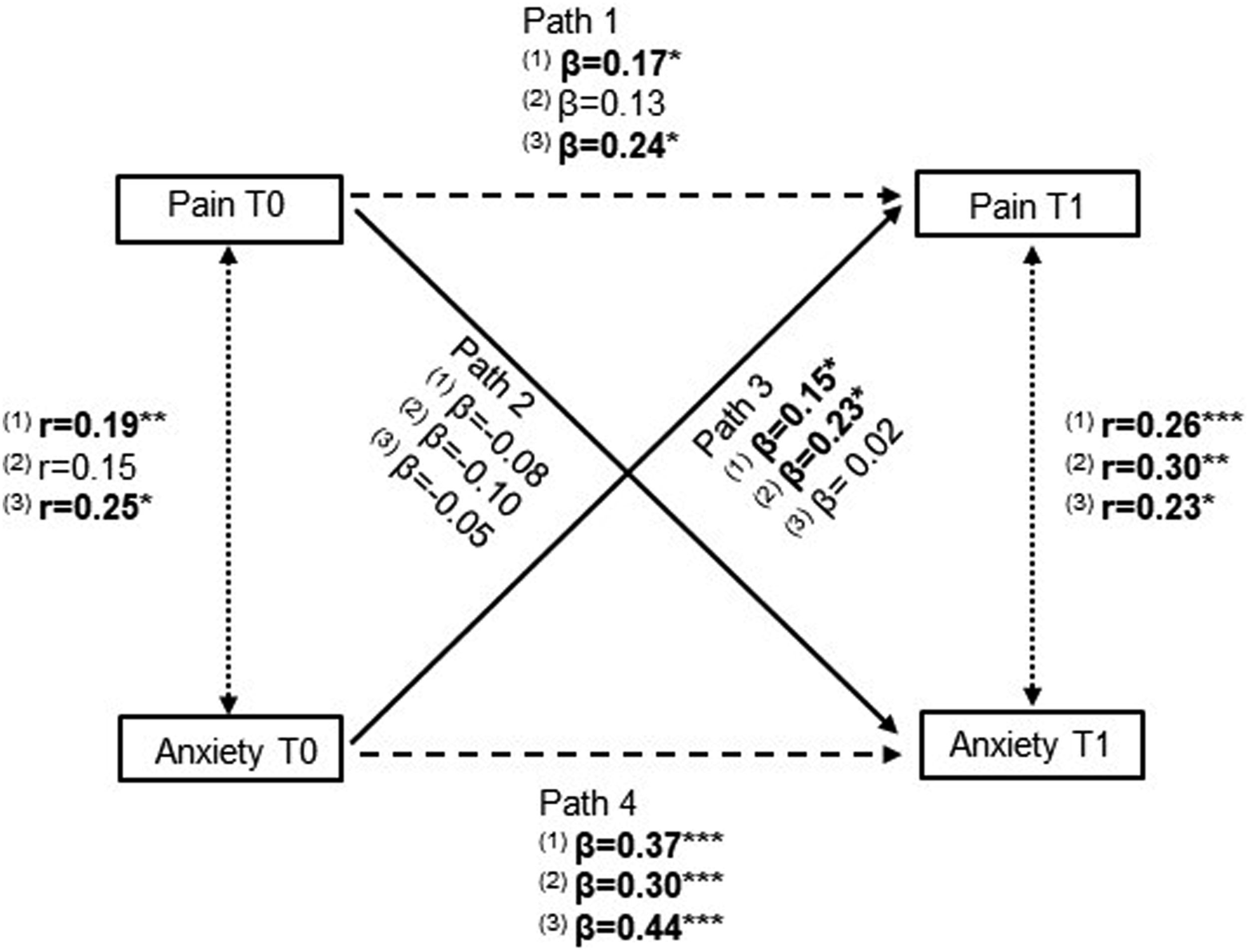
Mediation analyses
Standardised estimates for CLPM including potential mediators in the relationship between presurgical anxiety levels (T0) and postsurgical pain (T1).
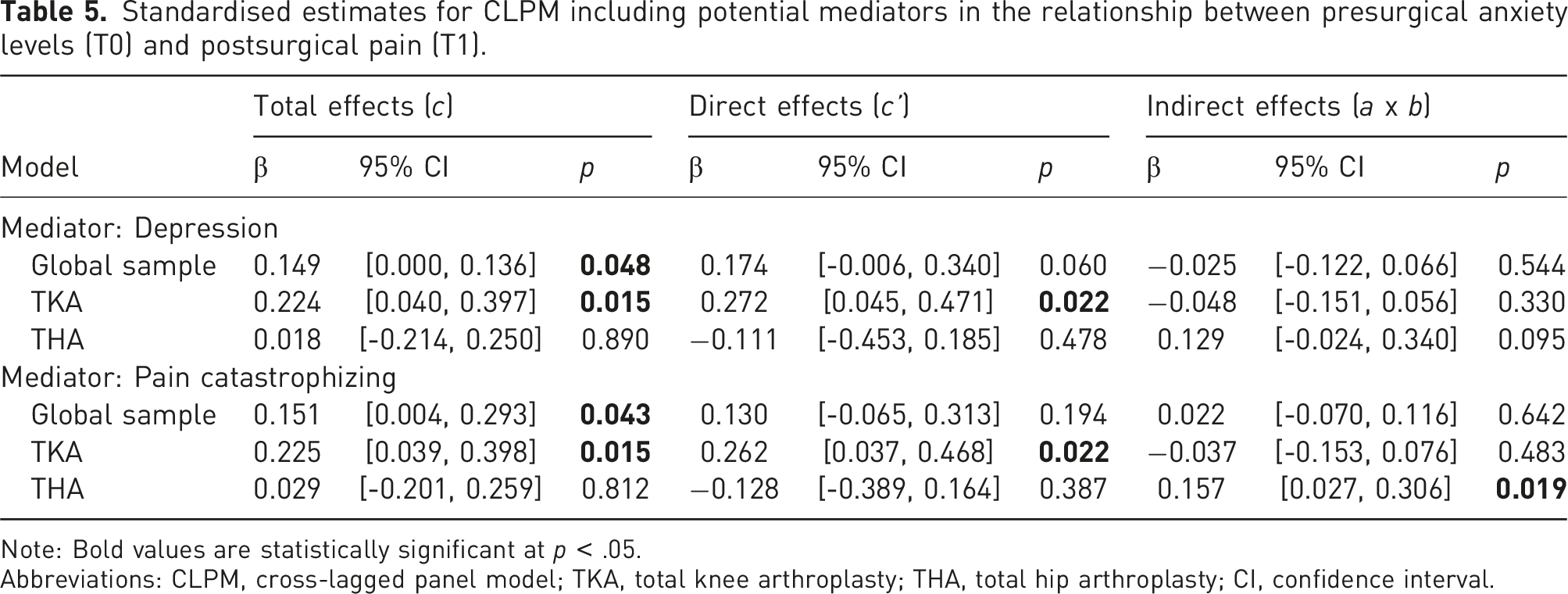
Note: Bold values are statistically significant at p < .05.
Abbreviations: CLPM, cross-lagged panel model; TKA, total knee arthroplasty; THA, total hip arthroplasty; CI, confidence interval.
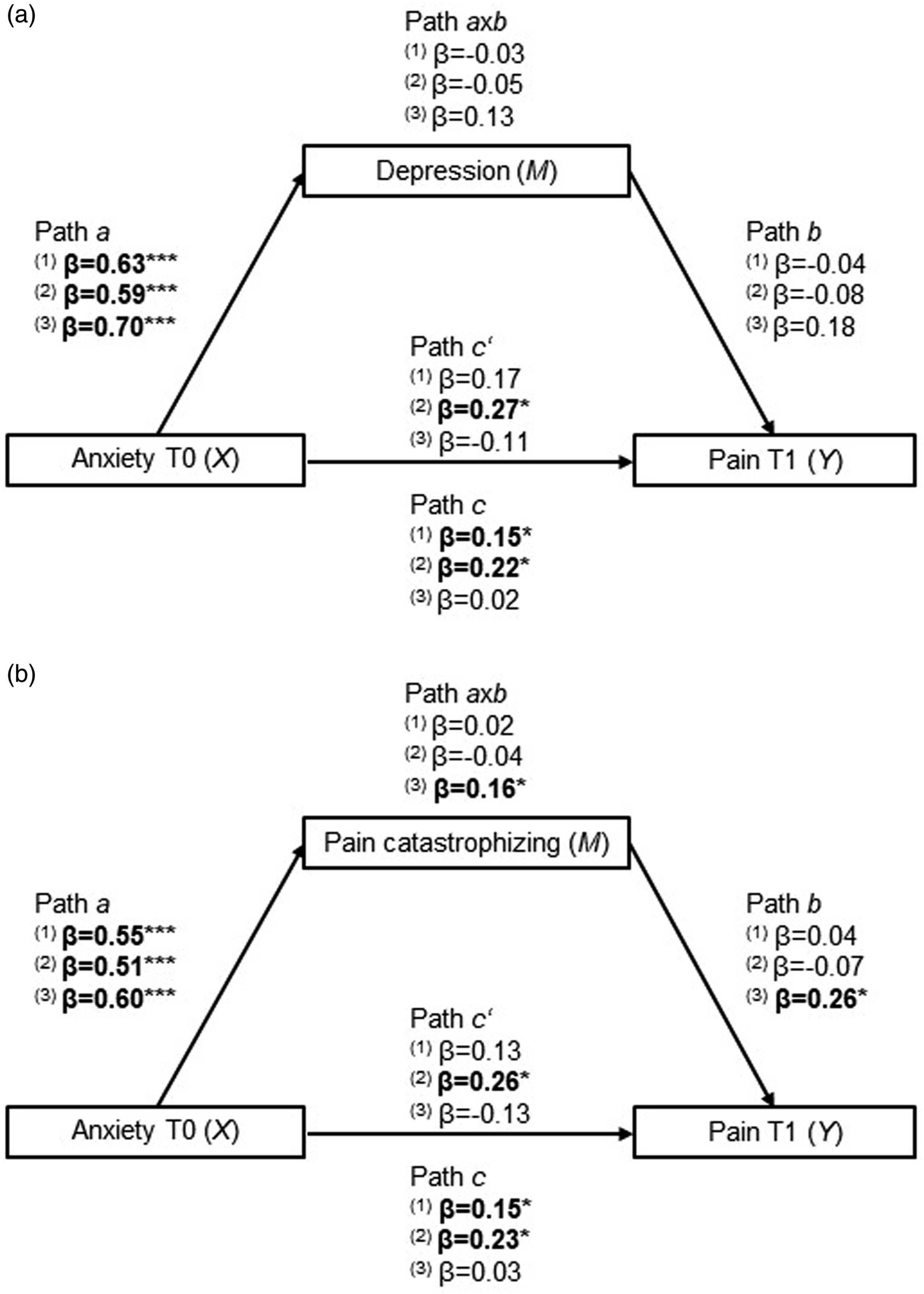
Illustration of the mediation analyses for the global sample (1), TKA (2) and THA (3). Depression (a) and pain catastrophizing (b) were tested as mediators (M) in the association between presurgical anxiety (X) and postsurgical pain (Y). The arrows represent relationships between variables. Path c’ is the direct effect from X to Y, path axb is the indirect effect from X to Y, passing through M and path c accounts for both the direct and indirect effects. Bold values are statistically significant at p < .05 (***p < .001, *p < .05).
When the variable ‘depressive symptoms’ was included to be tested as a mediator (Figure 4(a)), the results revealed statistically significant total effects for the global sample (β = 0.15, p = .048) and TKA (β = 0.22, p = .015) and significant direct effects for TKA only (β = 0.27, p = .022). In the THA group, there were no significant effects. Depression symptomatology was not a significant mediator in any of the tested models.
When analysing pain catastrophizing as a mediator (Figure 4(b)), there was a statistically significant total effect (β = 0.15, p = .043), but no mediation (indirect effects: β = 0.02, p = .642), in the global sample. In TKA, there were significant total (β = 0.23, p = .015) and direct effects (β = 0.26, p = .022) but no indirect effects (β = −0.04, p = .483). In THA, pain catastrophizing mediated the effect from baseline anxiety levels to 48 h pain (indirect effect: β = 0.16, p = .019).
Discussion
This study analysed the longitudinal reciprocal associations between pre/postsurgical pain and pre/postsurgical anxiety levels in patients undergoing total knee or hip arthroplasty (TKA/THA) and explored psychological mediators of these relationships. The type of surgery was analysed as a moderator. Results showed that, for the global sample, higher acute postsurgical pain (APSP) was predicted by higher presurgical pain and higher presurgical anxiety symptomatology. However, postsurgical anxiety was only predicted by presurgical anxiety. These associations were different according to the type of surgery, with APSP being predicted only by presurgical anxiety in TKA and only by presurgical pain in THA. However, the critical ratios did not show significant differences between the two groups. Notwithstanding, mediation analysis showed that, specifically in THA patients, presurgical anxiety levels influenced APSP through pain catastrophizing.
In the present study, participants with knee osteoarthritis more frequently reported having other painful sites and had longer pain duration at the time of surgery. Indeed, there is generally a shorter time between symptom onset and surgery for THA than for TKA. 50 This may be due to a more restricted joint range of motion typically experienced by patients with hip osteoarthritis that imposes more limitations. 51 This assumption matches current results, with THA patients having shorter pain duration, but higher disability, which probably also underlies the differences in presurgical self-efficacy. Also of note is the fact that most patients undergoing TKA were women. Since women tend to undergo surgery at more advanced arthritis stages than men, it is possible that sex differences also account for these findings.52,53
Other studies have compared psychosocial characteristics before TKA and THA and concluded that most variables did not differ. There were some reported differences in optimism, 33 emotional well-being 54 or quality-of-life, 55 but the findings were inconclusive in terms of which surgical group had better psychosocial status.
After surgery, APSP was higher in TKA patients, as expected. 34 It is not clear why TKA causes higher APSP, especially because THA requires more tissue damage to expose the joint than TKA. 56 Thus, identifying clinical and psychological determinants of APSP remains a relevant research field. For APSP control, the majority of TKA patients had a continuous disposable infusion balloon, while THA patients mostly received intravenous analgesia. It could be suggested that these differences influenced differences in APSP, but similar conclusions have been reached even when anaesthetic and analgesic strategies were uniform for TKA and THA. 32 Thus, it is unlikely that the differences in this study are better explained by different anaesthetic and analgesic procedures.
The results showed a cross-sectional association between presurgical pain and psychological variables, both negative (anxiety, depression and pain catastrophizing) and positive (self-efficacy and satisfaction with life). This is consistent with the literature, which shows that osteoarthritis patients with higher anxiety, depression or pain catastrophizing likely report more pain.57–59 Conversely, positive emotions and expectations are associated with less intense pain.59–61 Consistent results were found at 48h, showing a same-moment significant positive association between pain intensity and anxiety levels. It is not possible to derive causal inferences from these results, but they highlight the interrelationship between pain and emotional well-being and the relevance of a biopsychosocial understanding of patients undergoing arthroplasty. 62 A longitudinal correlation was demonstrated between presurgical negative psychological variables and APSP, which was not evident for positive psychological variables. Interestingly, optimism has emerged as the most important predictor of acute pain after TKA/THA, 29 but it was not correlated with either pre or postsurgical pain intensity in this sample. In fact, optimism is frequently associated with pain,16,63 but there are also inconclusive reports of its effect on pain intensity after TKA and THA. 64
Globally, the present findings are consistent with literature on psychological predictors of APSP, which pinpoints anxiety, depression and pain catastrophizing as risk factors for more intense pain.11,12,16 Anxiety is the psychological variable most frequently assessed before surgery, 16 including before TKA/THA. 31 While some investigations report that presurgical anxiety is associated with APSP,25,28,65 others do not replicate these conclusions.24,26,33 The present study provided further data on this matter by analysing bidirectional longitudinal relationships between these variables. For the global sample, APSP was predicted both by presurgical pain and presurgical anxiety levels. In fact, presurgical pain due to long-lasting osteoarthritis may underlie phenomenon of local and spreading central sensitisation with impact on pain ratings in the acute postsurgical period. 66 Simultaneously, descending pain pathways can be modulated by emotional and cognitive processes, such as anxiety. 67 This is line with the Gate Control and Neuromatrix theories of pain, which highlight the contribution of motivational-affective and cognitive-evaluative factors to pain experience.68,69 It is possible that more anxious patients are prone to increased muscle tension and to heightened attention to bodily sensations after surgery, and thus more likely to experience increased pain.14,70
Subsequent multigroup analyses showed differences according to the type of arthroplasty. Presurgical anxiety levels predicted APSP after TKA, but not after THA. Inversely, presurgical pain predicted APSP after THA, but not after TKA. Hence, anxiety seems to be a relevant variable only for patients undergoing TKA. Though the differences between paths were not significant among groups, the results suggest that predictors of APSP may differ according to the type of surgery, even when only joint arthroplasties are being considered. In fact, a systematic review concluded that the role of psychological factors seems to be stronger for TKA, though there were few studies on THA.30,31 It seems likely that different variables may predict short and long-term outcomes of different joint arthroplasties. There are significant differences in APSP intensity even among surgeries of the same anatomical site, reinforcing that risk factors should be investigated individually, instead of under larger categories (e.g. arthroplasty, abdominal). 71 The specific variables that may be more relevant for each surgery remain uncertain, with more recent investigations coming to contrary conclusions on the weight of psychological variables for TKA and THA.33,54 It is now important that studies aiming to identify predictors of APSP include between-surgery comparisons. Deriving general conclusions from one surgical model may introduce relevant biases in the final conclusions.
Postsurgical anxiety was exclusively predicted by its presurgical counterpart, with no relevant influence of presurgical pain. This reinforces the utility of specific presurgical interventions targeting anxiety, with a potential beneficial effect on acute pain and recovery. 20
The role of psychological variables was further scrutinised through mediation analyses. Despite the absence of total or direct effects, an interesting result emerged for THA when pain catastrophizing was a mediator, revealing a statistically significant indirect effect in the association between presurgical anxiety levels and APSP. Indeed, current views of mediation analysis do not require an association between independent variables and outcomes as a prerequisite to establish significant indirect effects.47,72 According to our data, higher presurgical anxiety was associated with higher pain catastrophizing, which predicts more intense APSP in THA. Comparable findings have been reported for hysterectomy surgery, wherein pain catastrophizing also emerged as a mediator between anxiety and APSP. 73 The mediating role of pain catastrophizing has also been recently evidenced in osteoarthritis patients,74,75 further supporting the relevance of this construct for pain outcomes. Actually, pain catastrophizing has been pinpointed as the most consistent predictor of APSP,16,31 also with a relevant role for chronic postsurgical pain. 76 The idea that different variables may predict APSP after TKA or THA received further support in this study. The analyses revealed that anxiety had a direct effect in pain after TKA, and an indirect effect through pain catastrophizing in pain after THA. The reasons for this difference are not straightforward but may be due to specific group characteristics at baseline. Since THA patients had higher disability and lower self-efficacy, it is plausible that these patients view their painful condition and the surgical procedure as more threatening events for which they may lack the adequate coping resources. In face of this, anxiety symptoms may trigger catastrophizing thoughts that in turn contribute to increased pain.
Despite differences between types of arthroplasties, the present results highlight the role of emotional and cognitive factors for acute pain after both procedures, namely, anxiety and pain catastrophizing. Psychological variables contribute to APSP, along with the physiological processes related to tissue injury. 77 Thus, the biopsychosocial model should be adopted also for acute pain management. 13 Presurgical psychological interventions can improve pain control, reduce negative mood and improve surgical recovery,78,79 as recognised by current guidelines for APSP control. 17
This study has some limitations to be acknowledged. The age and sex discrepancy in patients undergoing TKA or THA is worth noting, since the first group included mostly women and had a higher mean age. The effect of these variables was controlled by including them as covariates in the CLPM models. Additionally, postsurgical pain was assessed at one time point. It is likely that an assessment with more than one evaluation moment during the acute period would provide a more comprehensive depiction of patients’ pain. Similarly, there are other psychological variables that would be relevant to consider in the context of postsurgical pain for a more comprehensive patient characterisation (i.e. fear of surgery, kinesiophobia, locus of control, resilience). These should be included in future studies to investigate their impact on APSP. Future studies should also be designed to investigate how pre/postsurgical pain and anxiety levels interact to impact longer-term outcomes. Though the longitudinal measurement invariance of anxiety was guaranteed, our decision was not to evaluate the measurement invariance of pain assessment since it was based on only two items from the BPI, which hindered this analysis.
To ensure real-world data, there was no restriction in terms of the anaesthetic and analgesic protocols.
Conclusions
It is still unclear if and which individual characteristics weigh differently on TKA and THA outcomes. This study provided further data on this subject, by revealing different variables associated with APSP after each arthroplasty type. Presurgical anxiety levels were shown to have a direct effect in pain experience after TKA, but an indirect effect in pain after THA. For THA patients, the anxiety – pain association operated through pain catastrophizing (indirect effect): higher anxiety contributed to more catastrophizing about pain, which led to increased pain perception. Taken separately, these findings are insufficient to recommend differential psychological evaluation for TKA and THA patients but are crucial in reinforcing the need for such an assessment in both groups and the relevance of more research comparing TKA and THA. Future studies should seek to explore and specify differences between arthroplasty types and understand the reasons that may underlie them. In order to develop, test and implement effective interventions for postsurgical pain, it is crucial to identify risk factors associated with APSP after each type of surgery. Besides the humanistic reasons that warrant effective pain control at any stage, the critical contribution of APSP to developing chronic postsurgical pain should be acknowledged. Effective management of APSP may be an important measure to prevent pain chronification and reduce the associated health care costs.
Supplemental Material
Supplemental Material - Differences in the relationship between pain and anxiety in total knee and hip arthroplasty: a longitudinal cross‐lagged analysis mediated by depression and pain catastrophizing
Supplemental Material for Differences in the relationship between pain and anxiety in total knee and hip arthroplasty: a longitudinal cross‐lagged analysis mediated by depression and pain catastrophizing by Ana Cristina Paredes, Patrício Costa, Márcia Costa, Patrícia Oliveira, Pedro Varanda, Armando Almeida and Patrícia R Pinto in British Journal of Pain
Footnotes
Acknowledgements
None.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work has been funded by Portuguese national funds, through the Foundation for Science and Technology (FCT) – project UIDB/50026/2020 (DOI 10.54499/UIDB/50026/2020), UIDP/50026/2020 (DOI 10.54499/UIDP/50026/2020) and LA/P/0050/2020 (DOI 10.54499/LA/P/0050/2020) and by the project NORTE-01-0145-FEDER-000039, supported by Norte Portugal Regional Operational Programme (NORTE 2020), under the PORTUGAL 2020 Partnership Agreement, through the European Regional Development Fund (ERDF). ACP has a PhD scholarship (SFRH/BD/146135/2019, DOI 10.54499/SFRH/BD/146135/2019; and COVID/BD/153639/2024) funded by the Portuguese Foundation for Science and Technology.
Ethical statement
Trial Registration
Not applicable because this study is not a clinical trial.
Guarantor
ACP
Contributorship
ACP: study conceptualisation, protocol development, ethical submission, patient recruitment and assessment, data analysis and interpretation, writing. PC: data analysis and writing; MC: protocol development, patient recruitment and writing; PO: protocol development, patient recruitment and writing; PV: protocol development, patient recruitment, data interpretation and writing; AA: study conceptualisation, protocol development and data interpretation; PRP: study conceptualisation, protocol development and data interpretation. All authors critically reviewed and edited the manuscript and approved the final version.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.