
Abstract
Background
Chronic pain is a highly prevalent long-term condition, experienced unequally, impacting both the individual living with pain, and wider society. ‘Acceptance’ of chronic pain is relevant to improved consultations in pain care, and navigating an approach towards evidence-based, long-term management and associated improvements in health. However, the concept proves difficult to measure, and primary qualitative studies of lived experiences show complexity related to our socio-cultural-political worlds, healthcare experiences, and difficulties with language and meaning. We framed acceptance of chronic pain as socially constructed and aimed to conceptualise the lived experiences of acceptance of chronic pain in adults.
Methods
We conducted a systematic search and screening process, followed by qualitative, interpretive, literature synthesis using Meta-ethnography. We included qualitative studies using chronic pain as the primary condition, where the study included an aim to research the acceptance concept. We conducted each stage of the synthesis with co-researchers of differing disciplinary backgrounds, and with lived experiences of chronic pain.
Findings
We included 10 qualitative studies from Canada, Sweden, The Netherlands, Ireland, UK, Australia and New Zealand. Our ‘lines of argument’ include a fluid and continuous journey with fluctuating states of acceptance; language and meaning of acceptance and chronic pain, a challenge to identity in a capitalist, ableist society and the limits to individualism; a caring, supportive and coherent system. The conceptual framework of the meta-ethnography is represented by a rosebush with interconnected branches, holding both roses and thorns, such is the nature of accepting life with chronic pain.
Conclusion
Our findings broaden conceptualisation of ‘acceptance of chronic pain’ beyond an individual factor, to a fluid and continuous journey, interconnected with our socio-cultural-political worlds; an ecosystem.
Keywords
Introduction
‘Chronic Pain’ is the complex and broad medical category given when pain is long-term; recognised as either a primary condition in itself, a symptom of another condition, or both. 1 Pain is subjective and multi-faceted, making diagnosis and management challenging.2,3 Chronic pain is a highly prevalent long-term condition, associated with significant societal and economic cost, including impacts on employment, benefits and healthcare provision.4–6 For the individual and their network, living with pain can bring condition management ‘work’, 7 or ‘treatment burden’, 8 involving multiple tasks, emotional management and coordination with healthcare. Experience of chronic pain can vary in severity, intensity, impact on mood and daily functioning,1,9 and people may additionally live with other long-term health conditions, a situation that increases with deprivation. 10 The contribution of distress, poor mental health and trauma to chronicity of pain is well established, along with the relationship of these factors to the wider determinants of health.11–13 These factors offer some explanation for the unequal experience of chronic pain, with higher prevalence among women, socioeconomically disadvantaged and racially marginalised groups. 14 As researchers, we should appreciate these factors and the role of society, including economic systems, in understanding chronic pain experiences and concepts. 14
Despite this complexity, there are research-based guidelines for chronic pain, with recommendations including supervised exercise, cognitive behavioural therapies, pain education and pharmacological management.15–17 In practice, however, the healthcare response to chronic pain often begins with short-term goals of pain relief, such as medication prescription, with the focus of healthcare only switching to longer-term goals of improved mood, function and quality of life (e.g. through rehabilitation, therapy and education) when the former is ineffective.18,19 Unfortunately, many medications have limited efficacy for chronic pain, 15 and escalating pain medication prescribing has led to concerning issues such as opioid related harms, 20 and particularly high levels of prescribing in areas of deprivation.21,22 Acceptance of the long-term nature of chronic pain is therefore increasingly seen as important and helpful in navigating the change in management approach, from seeking medical solutions, towards long-term management, and is associated with improved quality of life, mood and function.19,23,24 However, acceptance is challenging due to the inherent uncertainty of prognosis and outcome, 24 and the subjective nature of pain, which conflicts with the objectivity sought within the medical model, potentially affecting trust between healthcare professional (HCP) and patient. 3 Furthermore, the lack of societal – and healthcare – response to either accommodate for the long-term nature of chronic pain (for instance, chronic pain is not treated in the same way as other long-term conditions), or reduce chronic pain onset where this is possible, 25 can mean that the burden of ‘acceptance’ falls predominantly on the individual; we find this situation problematic.
The concept of acceptance can play a helpful role in the shift needed in our thinking, towards recognition of chronic pain as a long-term condition; however, conceptualising ‘acceptance’ has proven challenging. In the health literature, psychology has led the way in defining and operationalising acceptance of chronic pain, integrating the concept into therapeutic models.19,23,26 Acceptance is framed as a ‘behaviour’, measured by two components of engaging in life activities with the pain, and dropping ineffective efforts to control or avoid the pain. 27 However, questionnaires based on this dominant definition of chronic pain acceptance have poor psychometric qualities and the validity of the ‘acceptance’ content has been questioned.28,29 Furthermore, written statements on acceptance of chronic pain may be unclear in meaning and lead to misunderstanding in clinical practice.30,31 The qualitative literature on the lived experiences of acceptance of chronic pain shows complexity associated with the meaning, expression of language, and ideas related to cultural representations of ‘acceptance’, pain and illness.32–35
Delivery of pain care is complex, involving behaviours of both the HCP and person with pain, operating within a care system, influenced by availability and accessibility of care, and marketing regulations of healthcare products, for example, medications. 36 Furthermore, any individual response takes place within a healthcare environment, and cultural discourse, that may be inconsistent; promoting on the one hand, unrealistic cures that prohibit acceptance, may not be realisable, and can cause harm.20,36 Alternatively, the individual may receive quality care and responses that promote accepting chronic pain in an adaptive, helpful way, including recognition of the long-term and complex nature of chronic pain.15,19
While we recognise acceptance as an important mechanism that may mediate adaptive change for individuals with pain, our understanding is limited, and complicated by socio-cultural phenomena. In this paper, we argue that further conceptualisation of acceptance of chronic pain is needed for future healthcare developments including work to improve navigation through pain care, and to improve the long-term situation for people with chronic pain. Any further conceptualisation requires to factor in complexity associated with chronic pain and acceptance concepts, including healthcare systems, inequities, and cultural ideas of health and illness. The aim of this meta-ethnography is to explore and conceptualise the lived experiences of acceptance of chronic pain in adults.
Methodology & Methods
In conducting research, we apply our perspectives on the nature of knowledge (our ontological beliefs), how we believe this knowledge can be known (our epistemological approach), connected to our theoretical perspectives, which all shape and inform our approach to particular research topics. 37 In our study, we used the qualitative, interpretive methodology of meta-ethnography, 38 and theoretical framing of acceptance of chronic pain as socially constructed 39 to facilitate conceptualisation of lived experiences within complex social worlds. While constructionism itself is usually aligned with relativism, 37 the ontological positions of our research team with regard to our research approach and topic, lie between a degree of relativism and critical realism 37 ; typical positions for meta-ethnography.38,40 Taking this approach, enabled us to work with the epistemological tensions and imbalances in our field, particularly regarding differing perspectives and beliefs concerning key concepts; the understanding of pain (e.g. biomedical and biopsychosocial), ‘acceptance’ of chronic pain, and how social phenomena may influence these concepts.
We conducted a systematic search and meta-ethnographic synthesis of primary qualitative studies, which we report in line with eMERGe guidance 41 with more detail on criteria in Appendix 1. The protocol is registered with PROSPERO (ID: CRD42021253509). Meta-ethnography consists of seven phases, increasingly interpretive in nature, with methodological variation often reported by authors.38,40,42 We detail our selected methods to facilitate transparency. Reflexivity and positionality are important for rigour, transparency and management of potential bias during research; we adopted an approach of creating space within the research process and meetings to reflect and challenge perspectives, and CM kept reflective notes throughout the process.43–45 The positionality of our meta-ethnography team included people with lived experience of chronic pain; clinical practitioners and academics. Our disciplinary backgrounds include physiotherapy, medicine and sociology with additional input from public health and psychology.
Phase 2: Search strategy and screening
We searched the following databases in June 2021: MEDLINE, CINAHL, PsycINFO, Web of Science and AMED, from inception of database to present, including all languages and unpublished citations. A sample search strategy is in Appendix 2 and this includes search terms. We conducted the grey literature search across Ethos, Dart-Europe, Open Grey thesis databases and Google Scholar between June and July 2021. Eligibility criteria included primary qualitative studies of adults with chronic pain for over 3 months as the primary condition. We excluded painful conditions caused by specific secondary conditions such as cancer or HIV. The studies included an aim to investigate acceptance of chronic pain. Our rationale for this meta-ethnography included uncertainties with the psychological definition of acceptance of chronic pain. To be inclusive of conceptual boundaries, we therefore developed our own broad definition of acceptance of chronic pain for the study by combining definitions generated by nine members of the research and advisory team, given in full in the PROSPERO protocol.
CM initially screened all records to remove duplicates and simultaneously excluded immediately irrelevant results, 46 then imported citations into Rayyan software 47 for screening. In meta-ethnography, limiting the included studies can enable a focus on in-depth analysis. 48 We required rich data offering conceptual clarity relevant to our aim; therefore, we used purposeful sampling. 49 Title and abstract, and full text, screening was conducted by two blinded reviewers with a third available to resolve any disputes. CM reviewed all citations with additional co-researchers (CS, CC, RB and JM) acting as second or third reviewers. We completed screening in February 2022.
Phase 3: Reading the studies
Phase 3 of meta-ethnography involves reading the studies to develop familiarity. CM conducted quality appraisal of each included study and extracted data using a standard form (details and example in Appendix 3). This was conducted as part of the contextual analysis and not to influence decisions about inclusion. CM read all the papers to develop familiarity and extracted conceptual data, preserving author-given themes. We conducted pilot testing with three studies where a second synthesiser (CC or CS) independently read and extracted data. We then met to compare and discursively resolve which data we extracted, although both reviewers tended to broadly agree on data extraction. CM kept notes of this process. CM completed the data extraction for the remaining studies, with checks on this process by CC and CS.
Phase 4: determining how the studies are related
Firstly, we developed summary points that were the combined meaning of participant quotes and the author interpretation. We conducted pilot testing with three studies. CM and a second co-researcher (CC, CS or DB) independently highlighted the main findings from conceptual and contextual data extraction sheets to be taken forward as summary points. We then met to discuss and agree findings. CM and another co-researcher (CC, CS, ET, DB or RB) met for checks and discussion for the remaining seven studies. CM labelled each conceptual summary line with the original author-given theme/s.
Secondly, we developed a conceptual category grid to enable initial comparison of studies. We selected LaChapelle et al. 50 as an index paper. CM laid out the index paper’s summary points into the author-given themes in a Microsoft Word table, then added summary points from further studies, expanding and revising the table to account for additional author-given themes. We then compared the studies to consider useful ways of grouping the studies that could help preserve the study contexts and assist with the interpretation, until consensus.
Phase 5: the translation
Firstly, CM realigned the conceptual categories from phase 4 to provide an overview of how the differences and similarities between studies mapped out across studies. Secondly, CM developed mind maps for each grouping, to help conceptualise further aspects of interpretation and the relationships between these. Thirdly, CM used the mind map as a basis for translating the sections of study data into each other. CM conducted this for each of the three groupings with feedback and checks throughout from co-researchers.
Phase 6: line of argument synthesis
At phase 6, we extended the interpretation of the phenomena under investigation. 41 CM primarily conducted this with checks, feedback and perspectives from co-researchers and additional advisors from different disciplines (psychology, medicine, physiotherapy, public health, social science) between May 2022 and September 2023.
Findings
Search
The database search returned 2584 citations after initial removal of duplicates. Following manual duplicate removal and screening for immediately irrelevant results, we moved 460 to title and abstract screening, then 28 to full text screening. Eight studies were included from the initial search including Viane et al.
51
following translation from Dutch to English; Brady et al.
52
following correspondence with the author and the provision of additional data on the acceptance theme; and Kinzel
33
following review of the thesis. The grey literature search returned another two theses Ng and Liersch,34,35 leading to 10 studies included in the meta-ethnography. Figure 1 shows the PRISMA flowchart of the process. PRISMA flowchart.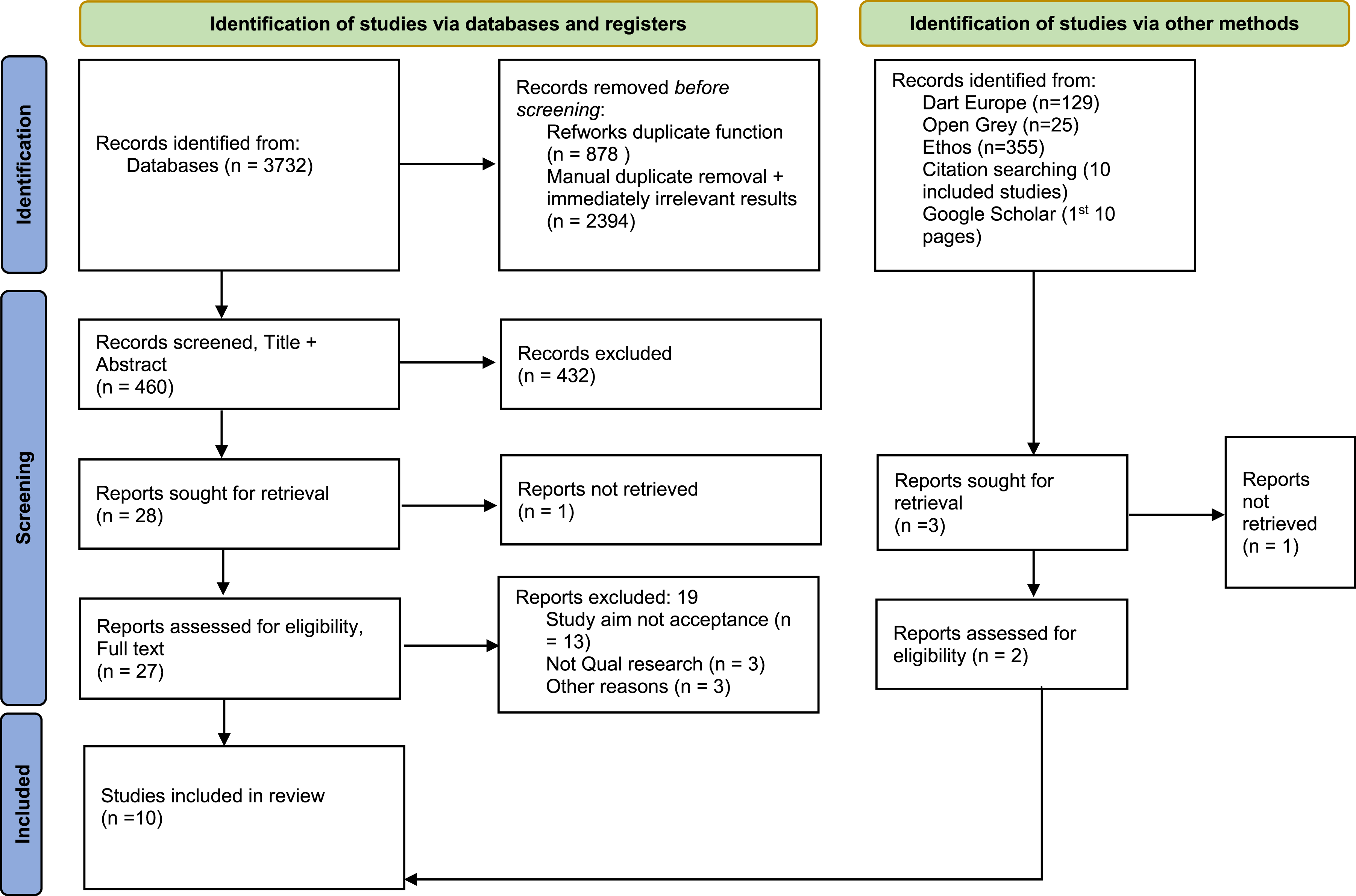
Study characteristics
Population characteristics of the included studies per grouping.
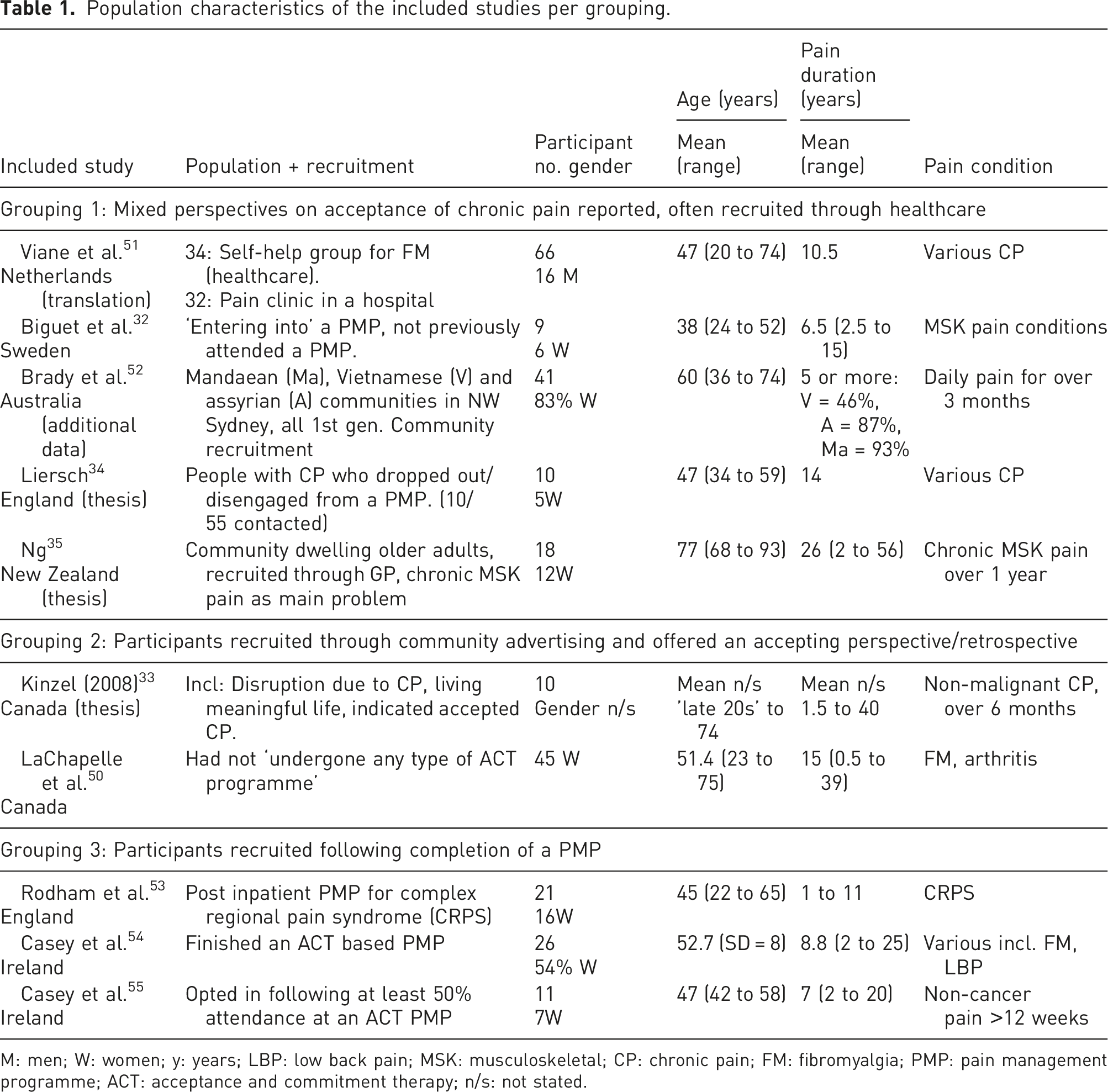
M: men; W: women; y: years; LBP: low back pain; MSK: musculoskeletal; CP: chronic pain; FM: fibromyalgia; PMP: pain management programme; ACT: acceptance and commitment therapy; n/s: not stated.
Phase 4 findings
Aspects of the studies considered and compared for potential groupings at phase 4 were recruitment method; theoretical approach to acceptance; chronic pain conditions or duration; socioeconomic status or ethnicity (insufficient details); geography; data collection method; and study aims. The perspective of the study on acceptance of chronic pain was our selected approach as this was coherent, could be used to preserve the study context, and extended the interpretation. This perspective showed to what degree the populations had accepted life with chronic pain, influenced by the authors’ approach to the research.
Phase 5 findings
The studies translated reciprocally within three groups, and although there were some differences in perspectives, they described aspects of the same complex, fluid phenomena associated with acceptance of chronic pain. The study groupings are shown in Table 1 and, to facilitate transparency, the full translation tables are in Appendix 6.
Phase 6 findings: Lines of argument and conceptual framework
At this stage of meta-ethnography, we present our interpretation of ‘lines of argument’, developed from the included studies, brought together in the conceptual framework that we present first to convey the fluidity of the phenomena and interconnectedness between the lines of argument that follow. While the phase 6 findings only use literature from the included studies, following this, we discuss our findings in relation to the literature thus providing further contextualisation of the interpretation.
The conceptual framework
The overarching conceptual framework is given in Figure 2; ‘An Ecosystem of Accepting Life with Chronic Pain’. The centre shows fluctuating and fluid states of acceptance. The outer branches, and roots, show aspects that are societal, cultural and political in nature. Aspects of the process of accepting, ‘a fluid and continuous journey’, that surround the fluid states are shown as a middle section of the circular ecosystem. The connections in the framework are fluid, indirect, and interconnected, and depicted by the branches of the rosebush holding both flowers and thorns, such is the nature of accepting life with chronic pain. The bees, as pollinators, emphasise the connected nature of the concepts in the ecosystem. The conceptual framework of ‘an ecosystem of accepting life with chronic pain’.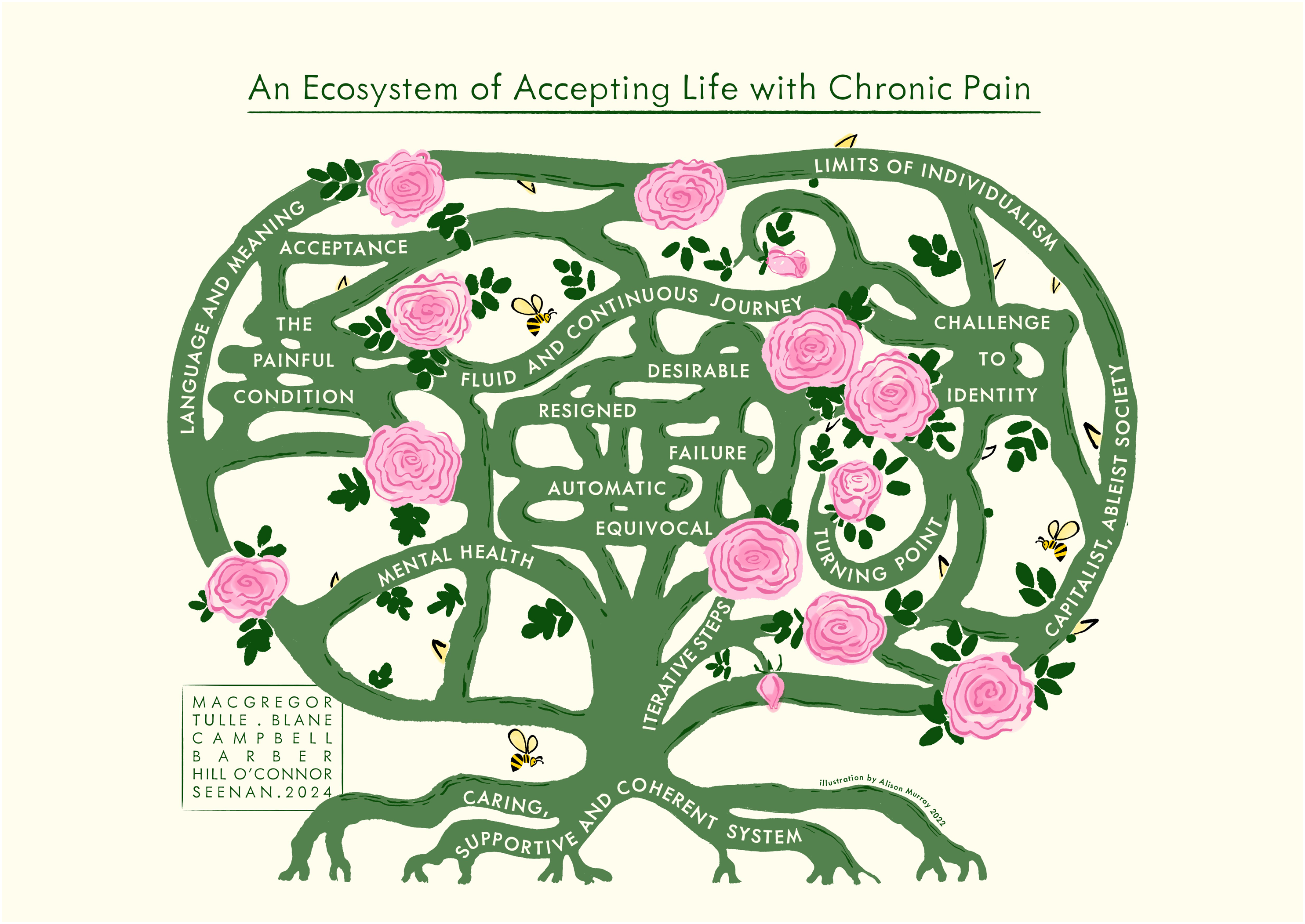
Phase 6 findings: Lines of argument
Viane et al. 51 translated text, and the author of Brady et al. 52 supplied additional data on the acceptance theme to us on request. Therefore, these quotes do not have a page number.
A fluid and continuous journey of accepting life with chronic pain
A ‘line of argument’ in our findings is that the process of accepting life with chronic pain is a fluid and continuous journey, featuring fluctuating states of acceptance, iterative steps, a turning point and relationship with mental health. The fluid quality is apparent where ideas of movement and direction are described; circular, back and forth, parts repeatedly revisited, occurring on multiple levels. The process can involve an overall quality of forwards movement and adaptation, and likened to learning, growth and frequently to grieving. “Acceptance of pain was described as a dynamic and ongoing process of adapting to chronic pain, rather than being static… various aspects appeared to influence the process of acceptance such as role identity and social context.” (Viane et al., 2004)
The process of accepting is described in more linear terms by people who are looking back on the journey. In this sense, ‘acceptance’ can be understood as a ‘desirable state’ and people can recognise what has helped or hindered their journey, describe a purpose to the journey and learning that has occurred. However, in accepting life with chronic pain, there is ‘no definite end-point’ (Rodham et al., 2012). An aspect of fluidity ‘referred to the temporality of acceptance and that participants could exist between the two states of acceptance or non-acceptance at the same time’, (Ng 2020: 74), possibly linked to the nature of the painful condition, where one can be pushed back to non-acceptance and cure-seeking in a pain flare. ‘There are times when you feel one way and then as your condition changes you will feel quite the opposite and it goes back and forth until you arrive at a point where you feel this is where it’s going to be’,(Kinzel 2008: 78). There is nothing to suggest from the study demographics, however, that older age or longer duration of pain facilitates the process towards a ‘desirable state’. The study with the oldest population, with the longest reported pain duration (Ng, 2020), reported a theme of ‘begrudged acceptance’.
Fluid and fluctuating states of acceptance
We describe the fluctuating states of acceptance below. It is necessary to describe each state as a discrete experience. However, there are links, overlaps and coexistence between them. These fluid and fluctuating states include acceptance as desirable, failure, equivocal, begrudged and automatic states.
Acceptance can be a desirable state of reconciliation, hard won and empowering, with an active, adaptive relationship with the pain and its impact. There is purpose to taking responsibility for health, pain and action to deal with it, more connection with meaning in life, and less mental health difficulties. There can be qualities of kindness, openness, with less judgement about oneself or others. The body can be experienced with awareness and ‘listened to’ as a guide to set limits. ‘“The pain is there and the acceptance is that you have to agree with your body that it’s going to be there but you can control it in the activities that you do.” Acceptance for Gordon “meant a little bit of being at peace with myself”’ (Kinzel, 2008: 51).
A state of acceptance can be conceptualised as failure of the self and others, ‘non-acceptance’, or barriers to a desirable state of acceptance. The term ‘acceptance’ is problematic for some people living with chronic pain and can mean ‘giving up’, ‘giving in’ and can represent ‘failure’ or ‘surrender’. ‘You have to keep fighting; you don’t surrender to the pain’, (Viane et al., 2004). One can be overwhelmed: ‘the body in pain constantly makes itself felt in restricting everything; it is in the foreground, hard to see beyond it. The focus upon the restricting body closes off all possibilities to experience acceptance’ (Biguet et al., 2016: 1263). It feels impossible to live with the pain. There is a search for a cure and an explanation. One may feel doubted, abandoned, that life is not worth living and may withdraw from others.
Acceptance of chronic pain can be resigned or begrudged; a forced coexistence with the pain and its impact which is beyond one’s control. ‘It isn’t that I accept it, I put up with it … there is no alternative, right so get on with it’ (Ng, 2020: 63). ‘Many considered pain as beyond their control and one with which they were “forced to coexist”: “I have been suffering from the pain since 5 years. I coexist with it, what else can I do?”’ (Brady et al., 2017).
Liersch 34 described a state of acceptance as an automatic response, not a conscious decision. Life is lived around the relationship with the pain, automatically aiming to neutralise the impact: ‘Anders, for example, engaged with [persistent pain] by dropping all activities that could anger it…It seems that he became accustomed to disengaging from the world around him and standardising his social withdrawal to control the [persistent pain]’ (Liersch, 2019: 71).
Equivocal acceptance is characterised by contradictions, uncertainty, ambivalence and struggle. ‘Often a turning point can be described, where it was obvious life could not go on like this: “there have to be alternatives to drugs,”…However, there is some doubt about one’s own ability, the resources of the body and the self, and about what concrete strategies to use’ (Biguet et al., 2016: 1262). Brady et al. 52 describe apparent contradiction between acknowledgement of no cure and continued pursuit of one: ‘Despite almost universal acknowledgement across both ethnocultures that pain…had “no cure,” this did not stop the communities from pursuing solutions. For the Assyrian community, this pursuit was underpinned by a sense of hope and fundamental spiritual belief that “a solution will be advised… with God’s help.”’
Turning point
The phrase ‘turning point’ frequently appeared in the studies representing a significant feature in the journey. Liersch (2019: 77) used the term ‘experiencing dawn’, meaning a ‘significant event of insight, understanding or clarity, a stepping out of darkness’. The turning point represents a shift in attitude and approach to living with pain, associated with adaptation and accepting life with chronic pain. The studies frequently associated receipt of a ‘diagnosis’ with a turning point. Casey et al. 54 describe a point of rock bottom, which evolves to a sense of hope. The turning point can also be seen in the context of a longer, complex journey of smaller moments. Kinzel (2008: 78) illustrates a more gradual realisation: ‘it wasn’t a sudden kind of thing that one morning I woke up and said “well I accept this” and that’s that… It was more of a gradual process and I think that that process probably is ongoing’.
Iterative steps in the journey
Another aspect of the fluid and continuous journey is the notion of iterative steps, or strategies, mainly described by participants in studies relating to an accepting perspective. ‘Acceptance of pain is a process. You have to go through it step-by-step and I don’t think there’s any fast track to the end’ (Kinzel, 2008: 78). We summarise the iterative steps described across the included studies below: • Having a diagnosis/name for symptoms, that provides validity and legitimacy. • Recognition and acknowledgement that there is no cure, and letting go of pursuit of a cure. • Acknowledgement of limitations. • Acknowledgement and realisation there is no return to ‘normal’, pre-pain life; life has changed and one needs to move forwards and live life with the pain. • Creation of space to look forwards. • Reframing of perspectives, priorities, goals, bringing focus on aspects of life that bring meaning, purpose and satisfaction. • Recognition that others are needed for support and it is important to communicate and ask for help. • Redirect effort from seeking causes/triggers of pain or trying to control these, to managing the consequences of pain and adaption. • Grieving losses of the changed situation. • Learning from one’s own previous experiences including disappointments.
Mental health and accepting life with chronic pain
The quality of mental health experiences varies across different states of acceptance. Biguet et al. (2016: 1262) illustrate the complex relationship that can exist between pain and mental health that they argue plays a role in the accepting process: ‘pain is also experienced as diffuse: it is difficult to distinguish from, often tangled up with, feeling ill, anxious and depressed. Sometimes bodily pain and mental pain are difficult to separate’. Past suicidal thoughts or thoughts of death as a way of escaping the pain, or the situation, were mentioned in the three theses,33–35 but did not appear in the published studies. Several studies likened accepting life with pain to the grieving process, moving on with multiple losses, where support can be helpful: ‘having a psychologist or someone to talk to…to help you with the anger… the denial and all the other stages of grieving you go through’ (LaChapelle et al., 2008: 206).
Acceptance as failure/non-acceptance can be characterised by shame, guilt, feeling overwhelmed, anger, depression, disappointment and worry, as illustrated by Biguet et al. (2016: 1263): ‘one cannot rely on a body that is a constant disappointment, as the good days never last and the hope for a cure fades… “The body is constantly screaming and shouting for help, but I don’t know what the body wants. I’m shouting back, I don’t know what to do!”’ Liersch (2019: 68–69) described ‘resignation’ where mental health can be poor: ‘I used to get this, like, a giving-up sensation… “oh, I’ll give up, oh sod it, you know, rather than go out for a walk or do this lot, I’ll just go to bed.”’
Where people described acceptance, there was often better mental health, less struggle and shame, although this did fluctuate. ‘Over time Sara started “being easier on myself and not judging myself so harshly… It’s the pressure I was putting on myself…so it’s been getting rid of that pressure, acknowledging it doesn’t need to be there, and it’s not helpful"’ (Kinzel, 2008: 96).
Language and meaning of acceptance and chronic pain
The studies frequently opened by discussing the complexity of language and meaning of acceptance related to life with chronic pain. ‘Language and Meaning’ goes beyond the particulars of terminology applied to ‘acceptance’ and chronic pain, and is both individually and culturally constructed, influenced by conceptualisation of health, illness, pain and capability.
‘Acceptance’ of chronic pain
The meaning of ‘acceptance’ is difficult to articulate, invites contradiction and appears to be a contested concept: ‘Patients struggled to describe and define acceptance of pain. Some patients found it difficult to attach meaning to the term acceptance’ (Viane et al., 2004). The word itself can be an obstacle; ‘I think acceptance is a rotten word’ (LaChapelle et al., 2008: 203), and can provoke emotional reaction or resistance, and at the same time, ‘the meaning attributed to acceptance seems particularly important in creating the ability to move forwards with pain’ (Casey et al., 2019: 13).
The individual meaning can depend on how the person relates to the state of acceptance. For some, acceptance is desirable, ‘hard won’, an ongoing journey; for others, ‘failure’, ‘giving in’, and these ideas may coexist. Furthermore, ‘concepts of acceptance emerged differently across the communities and were influenced by the explanatory model of pain and cultural values of each community’ (Brady et al., 2017).
LaChapelle et al. (2008: 203) suggested preferred terminology of ‘coming to terms’, ‘embracing’ and ‘dealing with’. ‘Accepting’ as a verb may be more appropriate as the term is usually referring to an ongoing process. Kinzel (2008) found the language of acceptance is different in word choice, tone, outlook and perspective to that of non-acceptance (the time prior to acceptance).
Conceptualisation of the painful condition and the need for ‘diagnosis’
The studies often showed that having ‘a name for the symptoms’ or ‘diagnosis’, and the meaning attributed to this, was important to accepting life with chronic pain, and could provide validity and insight to the person with pain: “I think for us with [Fibromyalgia], before you even get to acceptance that you have the condition, it’s having a diagnosis. You go for 10, 20, maybe more years without having a proper diagnosis…So it seems to be all in your head and you, people around you, your doctor, think it’s all in your head…So for me, the absolute crux of the matter is to actually get that diagnosis first and then you can start to accept it.” (LaChapelle et al., 2008: 204) “Without the diagnosis and a level of acceptance, it was impossible to work towards an ability to self-manage, because participants were essentially battling the unknown.” (Rodham et al., 2012: 34)
The meaning of the painful condition is subject to individual interpretation, thus associated with different factors. Ng 35 found that ‘ageing’ being given as a reason for the painful condition could either help to facilitate a positive position on acceptance, or may be seen as ‘dismissal’. Other factors associated with a more accepting conceptualisation included the pain viewed as non-threatening, recognition of the long-term nature of pain as similar to any other chronic illness, and ‘a belief that pain was part of living, and that pain was part of what you had done in life’ (Ng, 2020: 49). Similarly, Brady et al. 52 found that their Vietnamese cohort ‘interpreted pain as a natural consequence of living and as such was expected to behave in a cyclical nature’. The impact of the meaning of the painful condition is further illustrated by LaChapelle et al. 50 where some with arthritis resisted acceptance as they felt pain relief may be forthcoming through having surgery; whereas a Fibromyalgia diagnosis helped people to move forwards with accepting.
A caring, supportive and coherent system
We propose that accepting life with chronic pain occurs within an ‘ecosystem’, including healthcare and workplace environments, cultural norms and expectations. The studies showed that if this ecosystem provided a caring, supportive and coherent experience, then this helped the process of accepting. The relational aspect can be complex due to the multiple roles and interactions required of the individual, and the nature of pain as subjective and invisible; others cannot necessarily see or understand it. ‘Initially people understood my situation, but now, after years, they don’t show as much understanding. The exterior looks good, they don’t see what’s going on behind it’ (Viane et al., 2004).
Communication and information delivered with care
Supportive and caring communication is clear, open and empathetic, helping one feel believed and validated, and can lead to a greater sense of control, engagement and better self-management. ‘Looking back I think I needed somebody to sit down and talk with me and say “Yes, your pain is real, and let’s talk about what we can do to help you learn to accept to live with your pain”’ (Kinzel, 2008: 71). ‘Having a GP who was willing to learn about CRPS and to whom you could talk without feeling like a burden was of prime importance’ (Rodham et al., 2012: 35).
It can be helpful if advice and information is meaningful and specific. ‘Information and education therefore helped to normalise what were often unsettling CRPS symptoms…“I mean you can over-read about it, but try and get a good source of understanding the condition”’ (Rodham et al., 2012: 36). It helps if healthcare staff acknowledge limitations, uncertainty and unpredictability of pain and at the same time validate the pain. Conversely, unclear and uncaring communication can lead to emptiness, vulnerability and feeling abandoned. Resistance to accepting life with chronic pain can also come with a breakdown in trust with the HCP that can be brought on by lack of acknowledgement of pain, feeling not listened to, dismissed, and not taken seriously.
Support is needed to accept life with chronic pain
Practical and emotional support was frequently mentioned as important. ‘Perceived social support from family, friends, employers, patient support groups and HCPs was extremely important to pain acceptance. The women noted that different types of support were needed and were obtained from different sources’ (LaChapelle et al. 2008: 206). Sharing experiences with others can bring feelings of solidarity, validation, and acknowledgement of limitations and abilities. Support groups can help through recognising the long-term nature of chronic pain like any other chronic illness. A supportive workplace is flexible, understanding and accommodating to needs. Lack of financial resources, access, and support may limit adaptation, impact on mood, and interfere with pain management. The impact of having adequate finances is illustrated by Kinzel (2008: 93–94; 89): “Adequate financial resources facilitated adaptation… by allowing them to pay someone for services such as house cleaning…: ‘I’d rather fork out 40 bucks and be able to go work tomorrow than do it myself and not be able to go to work.”’ Furthermore: “Wilson eventually chose to leave a physically demanding job because of the resulting pain… this was ‘a big sacrifice in pay because you go from mid $70, $80,000 to $45, $50,000.”’ (Kinzel, 2008: 89).
Coherence
The experience of coherence in conceptualising the painful condition can be helpful. Ng (2020: 57–58) offers an example of the role of ‘diagnosis’ in a coherent experience: ‘participants felt receiving a diagnosis provided a framework for them to learn and manage their pain… “when I found out the diagnosis I knew how far I could push myself … you just got to work it out how you feel, your limitations.”’ The alternative scenario of incoherence is also illustrated: ‘Participants expressed the impacts of not receiving a diagnosis, such as being stuck in a state of helplessness and continuously trying to make sense of their pain experience… “I’m scared the pain will get worse … I don’t know what is happening, whether I will end up in a wheelchair or not”’ (Ng, 2020: 58–59). Medical systems can further lead to incoherence if their approach contradicts the nature of long-term pain: ‘To feel accepted as a pain patient appears to be related to the hope for a medical solution for their pain’ (Viane et al., 2004).
Workplace environments can provide a coherent experience by adapting to support workers with chronic pain: ‘current work environments offered flexibility, understanding, and accommodation to their needs. In contrast to the lack of understanding and lack of support many had experienced at work in the past, this type of support clearly facilitated their continuing with or returning to work while continuing healing, and gaining self-confidence, all of which influenced acceptance’ (Kinzel, 2008: 65).
The challenge to identity in a capitalist, ableist society and the limits of individualism
Another overarching ‘line of argument’ is the way that an individual’s sense of identity is challenged by the impact of chronic pain; their response appears to be an influential and pivotal part of the accepting process. Reconciliation with changes to identity, appears important to a sense of feeling better, and accepting, where one may re-appraise what brings meaning to life. ‘Perhaps the most significant barrier to the woman’s acceptance was the struggle to maintain their prepain identity…they often used their limited physical, mental and emotional energy to maintain an appearance of normalcy…The result was that their health status and quality of life further declined, often until they hit a crisis point that forced them to re-evaluate’ (LaChapelle et al., 2008: 207).
There can be a realisation that while aspects of identity may change, ‘the core of the self’ remains the same; ‘“I have realised that the pain is a part of me but it does not define me as a person”’ Biguet et al. (2016: 1261). However, the capacity to reconcile this challenge to identity may be negatively influenced by cultural ideology such as individualism. Identity was frequently tied to the normative expectation of the individual being ‘active’ and ‘capable’ in the studies, suggesting an ableism inherent to capitalist cultural norms and expectations including those of achievement and productivity. The ideology of individualism is visible in studies where the individual is understood to be the unit of agency that should be mobilised, over the structural, socioeconomic capacity of their situation. Brady et al. (2017: 5) show the impact of non-Eurocentric cultural values, contrasting with some other study findings: ‘rather than an individualistic point of view…Vietnamese integrated sense of self through their relationships with others and their community status’.
Reconciliation with the changes to identity brought on by chronic pain included participants letting go of previous identity tied to individual accomplishment, and was associated with becoming accepting: ‘“I’m a responsible person, I want to do a good job. I don’t want to go back to my job and not to do it well… so I put that on myself…so that gets in the way of me accepting that I have this and I have to change the way I do things in order to manage it,”’ LaChapelle et al. (2008: 207). This adjustment is further illustrated by Kinzel (2008: 96): ‘My identity was very much wrapped up in what I can accomplish, what I can be counted on for, and that’s something I’m still learning to let go of… I’m still that same person but my value isn’t because of the things that I can accomplish. It’s who I am’.
Alternatively, acceptance of chronic pain and its consequences may be conceptualised as failure or ‘giving in’, if one identifies as an ‘active, capable’ person and cannot accept the limits pain brings. The body can be understood as a ‘hindrance’ that renders one ‘incapable’ (Biguet et al., 2016). Viane et al. 51 illustrate this difficulty: ‘An important finding of this study was that some patients just did not accept pain and its consequences…These patients saw themselves as very active and capable before they were confronted with their pain. This makes it difficult for them to learn to live with the far-reaching changes in their lives as a result of pain such as no longer being able to work, losing social contacts and difficulty doing housework’.
The conceptualisation of acceptance as an individual factor is described in contradictory ways, as both ‘personal failure’ and a ‘personal empowerment process’ (Biguet et al., 2016: 1261, 1263) for which the person with pain has responsibility. ‘Taking responsibility was one of the choices many participants made at some point during their journey… Janice realized “somebody else wasn’t going to make this better and it was the realization that if I wanted to do something then it was up to me”’ (Kinzel, 2008: 85). The interpretation of ‘personal responsibility’, however, can be inconsistent and related to the state of acceptance in the studies. For some, personal responsibility can mean that they should be able to remain active, capable and to resolve their chronic pain, rather than ‘accept’ it. The inconsistency suggests that individual agency and concepts of ‘personal responsibility’ may be applied by participants, helpfully or unhelpfully, depending on wider contextual meaning, influenced by perception of cultural ideology.
The two study populations with the highest education levels50,55 more frequently described an accepting perspective. Whereas, the two study populations with the lowest education levels51,52 were both in the mixed perspective grouping, where acceptance was more often conceptualised as a state of resignation or failure. The studies did not report demographics consistently so we could not make further comparisons of the socioeconomic context. Nevertheless, these findings suggest that socioeconomic factors could have a bearing on the extent to which people are accepting of life with chronic pain. Some study participants have been able to move forwards in the accepting process with insight, re-evaluating identity, and reach out for support, particularly so in the studies where participants had completed a Pain Management Programme,53–55 and also in LaChapelle et al. 50 and Kinzel. 33 However, these aspects of the accepting process featured less in the mixed perspectives grouping. This could suggest that rather than the focus solely on individual agency, enhancing accessibility to care and support could have a positive impact in individual lives.
Discussion
The aim of this meta-ethnography was to review the currently available research within an interpretive paradigm to conceptualise the lived experiences of accepting life with chronic pain. We used meta-ethnography to synthesise data, including study context, from 10 qualitative studies. We broadened conceptualisation from an individual psychological construct to one interconnected with our social, cultural and political worlds. Our meta-ethnography is the first qualitative synthesis of acceptance of chronic pain. We describe accepting as both a potentially helpful process, but also one that can be problematic. We also propose to position ‘accepting’ as an overarching concept for the individual’s journey with chronic pain, that is interconnected with context, and multiple other concepts, including the nature of pain, access to care and societal approaches to health and illness.
Previous meta-ethnographies of chronic pain studies56,57 showed similarity in experiences of a process, and aspects of acceptance, which support our findings. The relevance of ‘diagnosis’ to moving forwards is evident in ‘the quest for a diagnostic holy grail’ with an adjacent theme of ‘ending the quest’, in Toye et al. 56 Validation of the person, pain and reconnection with the self and the world were important to recovery in ‘the healing journey’, of Toye et al., 57 with the idea of acceptance as a desirable state positioned in the final section. Our findings support the idea of a journey, the relevance of ‘diagnosis’, along with validation and letting go of unhelpful, curative hopes. Our work adds further context to the individual journey by placing it as part of an ecosystem interdependent with our social world including inequities in socioeconomic resources to manage chronic illness, the role of health systems, access to pain care, and workplace environments. We link the challenge to ‘identity’ that chronic pain can bring with cultural ideology. Our work emphasises the fluid and continuous journey as more iterative than linear. Using study demographics in the interpretation, we further evidence that age or pain duration does not necessarily mean that people move through a process to a desirable state; this does not automatically happen with time. Rather, there are cultural, social and economic factors that shape the acceptance process.
Our findings contain similarities to the dominant, psychological conceptualisation of acceptance in the psychological flexibility model of Acceptance and Commitment Therapy (ACT). 26 We did not aim to reconceptualise acceptance of chronic pain within the framework of psychology as a behaviour, process or mediator, 19 although it is possible to argue elements of these are visible in the findings. Similarities between our findings and acceptance within ACT include the fluid and ongoing nature of acceptance; capacity to be aware in the present moment with ‘the creation of space’ and ‘listening to the body’, and the self as context, similar to ‘identity’ in our more socially focused work. The transtheoretical model of behaviour change also contains similarity to our findings, foregrounding an iterative process of behaviour change stages, and can be applied to the behaviour of ‘self-management’ in chronic pain where ideas related to acceptance feature. 58
The difference between our framing of acceptance of chronic pain and previous work is that there is more focus on the socially constructed nature of the phenomena. We recognise that psychological models do include elements of an individual’s social context; however, we emphasise the phenomena as embedded in, and shaped by, our social, cultural and political worlds. While psychology literature has sought to include analysis of demographics as moderators, there is inconsistent data reported in primary studies, for secondary analysis. 59 Furthermore, the focus on people with chronic pain who have already entered into a psychology programme is selective, given most people attend primary care. 60 Improved understanding of individual behavioural and therapeutic mechanisms is essential to the development and effective delivery of interventions; however, social determinants of health and appreciation of life course including adversity are important to an equity framing. 61 An ecosystem approach can add social context to behavioural and therapeutic models in a similar way to analysis of ‘social practices;’ a critical perspective on health behaviours as dependent on structures, and culture, in addition to agency.62,63
It could be that for those with more socioeconomic capacity and resources it is possible to be more accepting of life with chronic pain. Although data on socioeconomic demographics in the included studies were incomplete, we report evidence that the ‘desirable state’ of acceptance featured more in studies with participants of higher socioeconomic status, with acceptance as ‘failure’ and ‘resignation’ more common among those with lower socioeconomic status. Lower socioeconomic status is associated with higher prevalence and severity of chronic pain. 64 Possible mechanisms of effect shown in our findings could include; the idea of ‘space’ required to accept, financial resources, mental health, workplace adaptation, capacity to negotiate the pain diagnosis and the associated health literacy, agency over identity, and having access and capacity to engage in pain care including groups. Webster et al. 65 report that people who live with chronic pain and lower socioeconomic capacity described difficulty with legitimising their pain, lack of access to care, having multiple, sometimes conflicting, pain diagnoses, with the additional work of poverty bringing out the idea of a knotted, chronic struggle. We also found this to be true, particularly in the mixed perspective grouping and less so in the two accepting groupings. Living with chronic illness brings condition management work that can be compounded by living with multiple co-morbidities, lower financial capital and health literacy. 66 Higher socioeconomic status brings more financial and social capital, and forms of power to cope with health and illness positively, including capacity to change the biographical narrative.67,68
Basing practice on exclusively individual, linear and normative approaches clearly is not effective. It is too much for individuals to take on, and side-lines the societal processes which affect people’s ability to fulfil the expectation of acceptance; new types of explanations are required to imagine different approaches that work for people. The challenge to identity brought on by chronic pain in our findings, is similar to the concept of biographical disruption that can occur within the illness trajectory of chronic pain.25,69 We linked this ‘challenge to identity’, to the normative idea of being ‘active’, and ‘capable’ and argue that this challenge to identity is most marked in capitalist, ableist systems. Varul 70 uses the term ‘resiliently capitalist achievement society’ when considering how people interact with social pressures and systems when living with chronic illness. We use this conceptualisation to understand the society in which participants struggle to continue their pre-pain role. Competition, individualism, the pursuit of economic growth and associated achievement as the priority of capitalist societies can displace wellbeing as a priority. Accepting chronic pain can involve reconciling disruption to a pre-pain identity. This reconciliation, however, may hold ongoing conflict with norms of ableism inherent in capitalist society that may prohibit acceptance. Framing of accepting life with chronic pain as a personal choice is influenced by prevailing, neoliberal ideology that focuses on individual agency, and responsibility for health, despite stronger evidence for social determinants impacting on the individual’s capacity to manage their health.71,72 In the context of neoliberalism, those who are unable to meet the ideals of an independent, active and productive citizens can experience stigma, shame and marginalisation, exacerbated in systems in which health status is tied to access to social security, requiring moral boundary work.73,74 Societal discourse frames those out of work as ‘scroungers’ and ‘shirkers’. 75 Without addressing these wider systems around the person in pain, there may be a limit to the extent to which they can become accepting.
Addressing the wider systems and limits of neoliberalism requires a new way of thinking about cultural, political, environmental and economic systems, to deliver a shift to a more caring, supportive and coherent system for people experiencing chronic pain. Our findings prompt us to consider wider debates about purpose of the economy and the role of the state 76 and engage with the growing calls for alternative economic systems, such as a wellbeing economy, which puts a focus on human and environmental wellbeing, over and above economic growth. 77 In a wellbeing economy, social and economic measures of success are multidimensional, taking an approach that values the quality of natural ecosystems, collective health, public trust and social relations, rather than a singular focus on economic productivity. 78 A change to systems in this way would influence conceptualisations of health and healthcare and open up the possibilities for acceptance of chronic pain in ways that do not require people to struggle against their pre-pain identities, reflecting our notion of the ‘caring, supportive and coherent system’.
Language is an important and influential area of health and healthcare, operationalised, consciously or otherwise. 79 Articulating on the fluid, complex and often contradictory nature of the journey brings difficulty. The tension in the studies between a process and a fluctuating state, suggest that researching ‘acceptance’ is a challenging proposition as the phenomena are fluid but meaning sought at a single time point in the participants’ lives. Cultural ideas of chronic pain, health and capability, identity and socioeconomic resources add to the complex situation.25,69,80 Terminology brings further challenges; ‘acceptance’ (the noun) can be conceptualised as a fluctuating state, but ‘accepting’ (the verb) may be more appropriate given the nature of the ongoing journey. However, some don’t like the term, or the prospect of, acceptance; it provokes resistance and alternatives may be better, including ‘coming to terms’. 50
We show the relevance of ‘diagnosis’, meaning that the person with pain has a name for the symptoms that provide validity and is associated with guidance on management. The criteria for this meta-ethnography included chronic pain as the primary condition, rather than pain as a symptom of a secondary condition such as cancer or HIV (which may have clearer, specific, diagnoses). Our included studies are therefore a subset of a broad chronic pain category and included conditions such as Fibromyalgia, complex regional pain syndrome, back pain and chronic musculoskeletal pain. Having a name for the symptoms was a key part of the journey for people living with these conditions, adding to the turning point, providing validity and coherence. Recent developments in chronic pain science, categorisation and increasing recognition of chronic pain as a disease in its own right 1 could prove helpful in providing validity. However, there can be a degree of sense-making with chronic pain that becomes unhelpful, in a condition that may not necessarily present a coherent experience. 81 Our findings highlight the importance of addressing health literacy for people living with chronic pain, which may otherwise be a source of inequity, as it can be with other long-term conditions. 66
Strengths and limitations
The GRADE-CerQual framework can be used to assess confidence in qualitative syntheses and outlines four main aspects to consider: methodological limitations, coherence, adequacy of data and relevance to the review question. 82 We prioritised transparency of the methodology at each stage to allow evaluation of this as we moved from a descriptive approach, towards an interpretive explanation. 83 We sought to maintain a high level of rigour, using co-researchers at each stage, engaging in reflexivity, continually reviewing and aligning methodological options. In reporting, we outline the methodological decisions and give our full translation findings and primary study contexts in online appendices. We do not report the frequency with which a primary study theme occurred in our lines of argument, because our interpretations were influenced by both what was said and unsaid across certain study contexts, for example, the relationships between the conceptualisation of acceptance, and socioeconomic positions of study participants.
Our meta-ethnography included 10 studies from high income, predominantly white, Eurocentric societies. The reported study demographics consistently commented on gender, age, duration of pain and painful diagnosis; however, socioeconomic and ethnic background details were inconsistently reported. This limited our interpretation of context in the synthesis to better understand equity issues. We conducted the initial search in June 2021 followed by our interpretation phases, which continued until Autumn 2023. While some systematic reviews may repeat a search after such time frame, with meta-ethnography we do not feel it would be possible to redevelop the interpretation after phase four. This could be considered a limitation, but is also part of the in-depth and lengthy nature of the interpretation in meta-ethnography.
In our meta-ethnography, we introduced primary data from five studies previously unpublished, in English. These studies included three theses,33–35 and one section of findings that the author passed on following email correspondence. 52 We also translated a study from Dutch to English. 51 It is noteworthy that four of these five studies contributed to the ‘mixed perspectives’ grouping, the less well-established perspectives on ‘acceptance of chronic pain’, and account for the two studies with the lowest, reported socioeconomic demographics and the only two studies to report inclusion of ethnic minority groups. We believe this has helped us to challenge the dominant narrative on the topic, and offer a broader perspective.
The ontological positions of our research team with regard to our interpretation lie between the ‘subtle relativist’ approach of Noblit and Hare 38 and the ‘subtle realist’ position of Campbell et al. 40 Another research team may not have reached our particular lines of argument, hence the alignment with relativism. However, there is a strong argument for realism in the relationship of the findings to the literature and recurrent themes in the included studies. Both acceptance and chronic pain concepts and how they relate to each other is influenced by time-period, cultural ideas of health and normative expectations of ability and productivity. Our interpretation was enhanced by including multiple co-researchers providing different perspectives including people with lived experience of chronic pain. 41
Conclusions
Our findings show how ‘acceptance’ – an important and commonly used concept in chronic pain – can be conceptualised using the interpretive methodology of meta-ethnography, and based on lived experiences. We conceptualise accepting life with chronic pain as an ecosystem to capture the fluid and continuous journey interdependent with our social, cultural and political worlds. Our findings can be used to develop understanding and delivery of healthcare, including interfaces and limits of care systems in a way that recognises fluidity and interconnectedness. The ecosystem of accepting chronic pain is an ongoing process that includes, but is not limited to, the concept of a desirable ‘acceptance’ state. In our conceptualisation, ‘chronic pain’ is a long-term health condition, and therefore comes with condition management work, and the required capacity, which may be impacted by health inequities. We argue for further consideration of if and how, a state of acceptance or the process of accepting, as complex as we have described, can be measured, and avoid promoting overstated objectivity. The prevailing, positivist paradigm of health research promotes ideas of reduction and measurement; however, the ecosystem of accepting life with chronic pain is complex, fluid and interdependent.
Supplemental Material
Supplemental Material - An ecosystem of accepting life with chronic pain: A meta-ethnography
Supplemental Material for An ecosystem of accepting life with chronic pain: A meta-ethnography by Cassandra Macgregor, David N Blane, Emmanuelle Tulle, Claire L Campbell, Ruth J Barber, Clementine Hill O-Connor and Christopher Seenan in British Journal of Pain.
Footnotes
Acknowledgements
With thanks to Dr Whitney Scott and Joletta Belton for comments on earlier drafts; Dr Joanna McParland for input on earlier work within our research including protocol development and literature screening, and Professor Blair H Smith for comments on earlier drafts and advice earlier in our research programme.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr David N Blane is academic lead for the Scottish Deep End Project, a collaboration between academics and frontline primary care practitioners working in the most socioeconomically disadvantaged communities in Scotland. Ruth J Barber is a sole trader as Lazy Beautiful Dream Yoga.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was undertaken as part of a jointly funded PhD studentship by Glasgow Caledonian University and NHS Lanarkshire held by Cassandra Macgregor.
Contributorship
CC and RB were involved in development of the protocol and conceptualisation, as co-researchers in data analysis from phases two through to phase six. CHO provided data analysis at phase six, and writing and editing the final interpretation. DB, ET and CS provided: supervision on the research conduct; data analysis as co-researchers; input to the writing and structure of the manuscript. CM led the conceptualisation, data analysis, wrote the original draft, reviewed and edited. All authors have approved the final draft.
Ethical statement
Guarantor
CS
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.