
Abstract
Objective
Prehabilitation encompasses preparatory clinical intervention(s) delivered during the period between diagnosis and treatment commencement. Despite widespread successful usage preoperatively, psychological prehabilitation is neglected in outpatient chronic pain management. Although pain management waitlists are associated with treatment attrition and psychological and physical decline, this time window is underutilised in preventing escalation. Waitlists present an under-explored opportunity to ‘prehabilitate’ patients waiting for treatment. This topical review aimed to: (1) examine the effectiveness of psychological prehabilitation for pain services; (2) evaluate the psychological and physical decline associated with waiting for pain management; (3) highlight key psychological prehabilitative targets for increasing treatment engagement; (4) promote pain management psychological prehabilitation within personalised pain medicine, building recommendations for future interventions.
Methods
Studies regarding the impact of waitlists and prehabilitation for chronic pain were reviewed.
Results
Findings demonstrated that the psychological constructs of patient expectations, health locus of control, self-efficacy and pain catastrophizing dynamically influence attrition, treatment engagement and outcomes while waiting. These constructs are amenable to change, emphasising their potential utility within a targeted waitlist intervention.
Conclusions
Prehabilitating chronic pain patients towards treatment engagement could circumvent cycles of failed treatment seeking, preventing psychological and physical decline, and reducing healthcare utilisation. Utilising the waitlist to identify psychosocial risk factors (external health locus of control, low self-efficacy and high pain catastrophizing) would identify who requires additional support to prevent increased risk of treatment failure, enhancing personalised care before prescribed treatment is accessed. This review cements the urgent need for pain services to engage proactively with prehabilitation innovation.
Introduction
Chronic pain presents an increasing global public health issue, impacting an estimated 20% of adults worldwide.1,2 Societal costs attributed to chronic pain are high, ranging from $560 to $635 billion due to pain and pain-related comorbidity care provision, and days lost to productivity. 3 Moreover, economic and service strains have dramatically increased in recent years; vast backlogs due to withdrawn treatment during the COVID-19 outbreak has resulted in extensive waitlists. 4 Furthermore, chronic pain is a prevalent symptom of long-COVID, 5 contributing an additional subset of patients waiting for treatment. Chronic pain is highly associated with psychological comorbidities, that together, entrench pain and detrimental psychological decline over time.6,7 The longer patients are left waiting, unfurnished with psychological strategies, the greater the cumulative detrimental physical and psychological impact. 8 Pain and depression interact bidirectionally 9 with a dose-dependent relationship; greater pain intensity is associated with elevated levels of depression. 6 Thus, intervening at the earliest point to prevent escalation is intuitive to reduce health, social and economic burdens. At present, there is an underutilised weapon in chronic pain management that is used pre-operatively in other physical conditions: psychological prehabilitation.
Prehabilitation is the clinical intervention between diagnosis and commencement of treatment.
10
This aims to promote physical and psychological wellbeing to prevent or reduce the severity of future complications. Evidence shows better general preoperative health is associated with improved postoperative outcomes across a range of chronic conditions including musculoskeletal disorders, chronic pelvic pain and cancer.11–13 Prehabilitation approaches are largely applied within preoperative settings, an example being Enhanced Recovery After Surgery (ERAS).
14
Traditionally, they are bimodal, encompassing physical exercise and nutritional optimisation.
15
However, the complex relationship between chronic pain and psychology requires greater emphasis on psychological elements in the pre-treatment phase.16,17 Hence, trimodal prehabilitation additionally includes psychological strategies.
18
The chronicity of persistent pain requires patient active participation in self-managing their condition.19,20 To do so, individuals need to be equipped with successful self-management strategies at the earliest point. However, in practice, psychology is not currently strongly integrated at pre-treatment in outpatient settings. Thus, the aim of this review is four-fold: (1) To examine the effectiveness of psychological prehabilitation for pain secondary care; (2) To evaluate psychological and physical decline associated with long treatment delays; (3) To highlight prehabilitative psychological targets to prevent patient decline and increase engagement; (4) To promote psychological prehabilitation for pain management within personalised pain medicine, building recommendations for future prehabilitation research.
Why psychological prehabilitation?
Prehabilitative strategies are highly cost effective; pre-operative ERAS protocols indicate a mean saving of $1458.62 per patient, 21.5% of the total cost of surgical procedures from reduced subsequent healthcare utilisation. 21 Psychological intervention is utilised as a chronic pain management strategy (at point of treatment) due to its efficacy and cost effectiveness. 22 Thus, on an economic level, exploring psychological prehabilitation for chronic pain self-management is valuable to further enhance the cost benefits of pre-intervention protocols. Unsupported long treatment delay increases attrition in pain management. 23 Thus, clearly, without psychological preparation, patients are less likely to be motivated to engage in treatment once accessed. As motivation and capability beliefs determine engagement in exercise participation24,25 and diet, 26 psychological prehabilitation will also have indirect benefits of adherence to the other trimodal prehabilitation elements. Behavioural decisions are continuously required; whether to participate in prehabilitation at all, and thereafter, daily to upkeep pain management strategies, physiotherapy and nutritional regimes. 24 Thus, psychology functions as the lever that facilitates adherence, increases interest, and initiates reflective motivation over why self-management is important. Therefore, psychological prehabilitation must be reasserted as a critical pre-requisite for pain management to optimise treatment.
Where few trimodal prehabilitation strategies have been implemented pre-operatively, psychological elements include cognitive behavioural strategies, preoperative education, behavioural instruction and stress management to influence pain perception and psychological wellbeing. 12 Postoperative pain, behavioural recovery, affect and healthcare utilisation are reduced as a result of psychological prehabilitation.12,18,27 Implementing education within chronic pain interventions is also found to increase internal locus of control, pain self-efficacy, positive perceptions, life satisfaction and reduce pain-related interference, pain intensity and anxiety.18,28,29 Anxiety and depression are also significantly reduced following trimodal prehabilitation utilising psychological strategies in chronic pain patients waiting for surgery.30,31 Given such results for pre-surgical psychological prehabilitation, it is likely these benefits may also be extended to prehabilitation before secondary care.
Psychological and physical decline: The need for waitlist optimisation
Consistent excessive strain from under-resourced health services globally has resulted in elongated waitlists. 4 These have been further exacerbated by the COVID-19 outbreak 32 reflected in a 46.3% increase in people waiting for NHS treatment in the UK; 6.48 million people as of April 2022, compared to 4.43 million in February 2020 (pre-pandemic). 4 Globally, average Pain Management Programme (PMP) waiting time ranges from 7.9 months (Canada) 33 to 2-years (UK). 34 Even prior to the added service pressures induced by the COVID-19 pandemic, these waiting times drastically exceed the International Association for the Study of Pain’s (IASP) guidelines of a 2-month wait-time for routine conditions, and 1 month for urgent or semi-urgent cases. Thus, the need for waitlist optimisation is rising.
The rapidity of treatment delivery for people with chronic pain is paramount for managing psychological vulnerability. Chronic pain is an independent predictor of higher suicide likelihood. 35 Furthermore, comorbid anxiety and chronic pain are also associated with greater odds of suicidal ideation and attempts. 36 Comorbid anxiety and chronic pain is well established35–37; a nationally representative sample indicating more than 60% of patients with generalised anxiety disorder had at least one chronic pain condition. 36 Extensive waitlists are characterised by anxiety and uncertainty, 38 and patients are left feeling helpless, disregarded and lost within the system.39,40 Reduced treatment as a result of COVID-19 led to worsening pain, greater stress, anxiety and depression.8,41,42 Concerningly, empirical data suggests rapid psychological decline occurs within 5-weeks on waiting lists, depleting health-related quality of life. 7 Therefore, intervention to support people living with pain during their waiting time is critical for psychological health and to prevent early mortality or suicidality.
Alongside psychological decline reduced physical health during long waitlists is also observed. Deterioration of pain-related conditions, increased pain intensity, fatigue, limited mobility and reduced activity engagement are all associated with longer waiting times. 40 Indeed, 33%–65% of chronic pain patients report worsened pain-related symptoms and functional disability when on extensive waitlists.43,44 Permanent disability benefits and unemployment are also increased with elongated treatment delay.33,44 Physical decline further exacerbates psychological distress, elevating anxiety and frustration. 40 This creates a cumulative effect between physical and psychological outcomes during longer waitlists. Notably, concurrent physical and psychological decline are observed in pain patients waiting for longer than 6 months. 40 Thus, clearly, in the context of increased service pressure, waitlists represent a substantial challenge for patients and a ‘critical time window’ for prehabilitation.
Psychological targets within prehabilitation to increase engagement
To effectively optimise the pre-treatment period, it is important to identify factors influencing behavioural engagement with treatment.
45
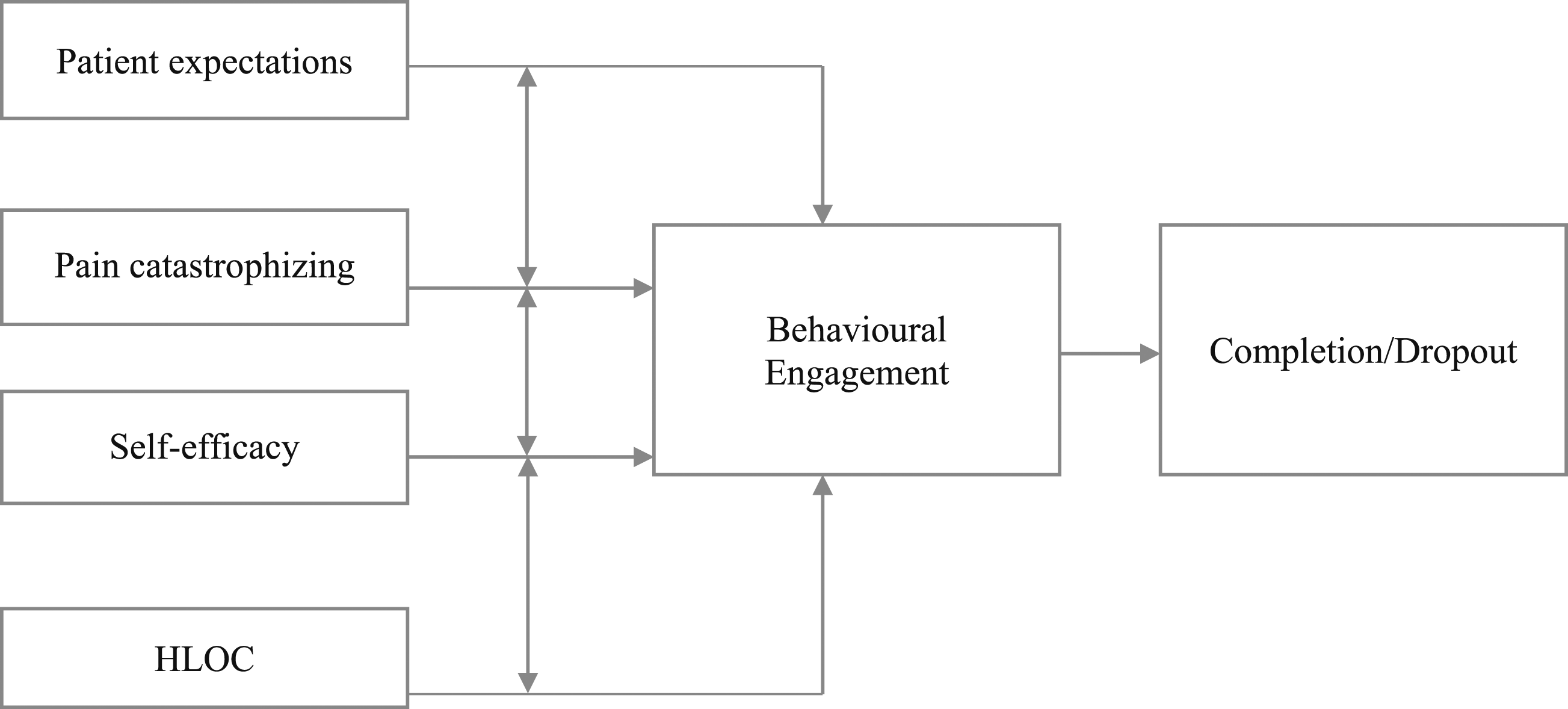
Evidence suggests these include interacting factors of patient expectations, health locus of control, self-efficacy and pain catastrophizing (see Figure 1).40,46–48 Moreover, the Faculty of Pain Medicine
49
recommends earlier application of pain management principles, and these constructs are central to the British Pain Society
50
guidelines for PMP content; such cognitive elements of perceived behavioural control are highly relevant to pain self-management engagement. Encouragingly, these factors are flexible to change through targeted intervention utilising cognitive behavioural and acceptance and commitment strategies, indicating their value in prehabilitation. The interrelating psychological constructs influencing behavioural engagement for pain management. Note. Patient expectations, pain catastrophizing, self-efficacy and health locus of control (HLOC) are all independently associated with behavioural engagement with self-management and treatment completion or attrition.23,39,65,81,82 Negative expectations are associated with higher pain catastrophizing.
57
Pain catastrophizing has a negative relationship with self-efficacy; higher levels of pain catastrophizing are negatively correlated with lower self-efficacy.
109
Self-efficacy and health-related locus of control are directly associated 46; high levels of internal HLOC are positively correlated with high pain self-efficacy, having greater behavioural engagement in pain self-management strategies.
47
Patient expectations
Patient expectations are defined as the set of beliefs regarding anticipated treatment and its potential effects 51 ; these are predictive of treatment outcomes.52,53 Positive expectations, compared to negative, are associated with greater improvements in disability, functional activity and reduced pain intensity, sustained beyond 6 months.54–56 Negative expectations of treatment and symptom worsening are associated with reported increased pain severity up to 8 months later. 44 In osteoarthritis patients, those with moderate to high expectations prior to treatment reported improved pain intensity, self-efficacy, quality of life, pain catastrophizing, and reduced use of pain medication following psychological intervention. 57 Therefore, even moderate, and not necessarily high, expectations can improve pain management outcomes.
Long waiting times with no information may also lower expectations regarding service quality and treatment outcomes. 40 Lack of information can lead to feelings of abandonment and disenchantment. 40 Thus, provision of sufficient information can be a simple way of abating a cascade of negative cognition and reduced engagement. Elongated waitlists pose a barrier in of themselves to accessing treatment; recent evidence suggests waiting lists of 4 months or longer increase the risk of not attending the first PMP session by 25%. 23 Thus, improving patient expectations through increased communication whilst waiting would likely increase perceived support, improving expectations and thus accessibility.
Managing patient expectations of potential outcomes is especially important prior to accessing treatment for chronic pain. While PMPs are effective in improving pain self-efficacy and pain interference, pain intensity may not significantly reduce. 58 When patients are left with inaccurate outcome expectations during extensive waitlists from incomplete information provision, this leads to extreme dissatisfaction once treatment is accessed. 40 When treatment outcomes are not congruent with patient expectations, frustration ensues, resulting in dropout. 59 This would further compound the increased susceptibility to attrition associated with long waitlists, 23 and short circuit a cycle of failed attempts and excessive healthcare utilisation. Therefore, targeting expectations of treatment outcomes via pain education during waitlists may improve both emotional wellbeing and completion rates. Consequently, this could reduce financial and service strains at a systemic level.
Health locus of control
An individual’s belief of their capability to exert control over their condition is fundamental to successful pain self-management.60–62 Health-related Locus of Control (HLOC) is a central construct conceptualised as either: (1) Internal (patients hold control and influence over their health), (2) Powerful Others (doctors and healthcare professionals hold greatest influence over health), and (3) Chance (health is determined by fate or chance events outside of individual control). 63 Within behavioural science, capability is one of three interacting elements (capability, opportunity and motivation) predicting behavioural change (COM-B model). 45 For a desired behaviour to occur, these behavioural elements must be supported. 64 Thus, given the integral role of perceived capability within HLOC, it is likely a fundamental construct for increasing pain self-management engagement.
Evidence suggests higher levels of internal HLOC are associated with greater competence and engagement in pain self-management for chronic disorders.63,65 Systematic review evidence indicates that HLOC is predictive in determining rehabilitation outcomes in chronic pain, with internal HLOC associated with optimal improvement. 46 Higher internal HLOC at pre-treatment significantly predicts greater reductions in pain intensity following multidisciplinary intervention, compared to those with low internal HLOC. 66 Greater functional improvement is also observed in patients with higher internal HLOC at pre-intervention, in both surgical (18 weeks post operatively), 67 and multidisciplinary settings.66,68 As chronic pain patients tend to present greater levels of external HLOC (69% identified as external HLOC vs 31% as internal) 48 ; optimising personal agency and belief towards capacity for self-management represents an important intervention objective. HLOC is amenable to change; CBT-based self-management interventions display efficacy in increasing perceived control immediately post-intervention and internal locus of control 12 months later. 23 Together, this evidence highlights the importance of HLOC at pre-intervention and its malleability. Thus, it is only efficient to implement such targets within prehabilitation to improve both treatment engagement and outcomes.
Self-efficacy
In the context of health, self-efficacy is defined as an individual’s belief in their ability to engage in health management behaviours pertinent to their condition. 67 Whilst patients are waiting, identifying those with low self-efficacy would enable stratification to additional support to prevent increased risk of treatment failure. Higher levels of pain self-efficacy encompass the perception of sufficient internal resources to overcome pain-related demands, and thus the ability to effectively cope with pain. 69 Pain self-efficacy is a greater independent predictor of disability, above pain severity, 70 and a key mediator of behavioural change.69,71 Patient engagement in pain self-management programmes is greater in those with higher pain self-efficacy 72 and low pain self-efficacy is a barrier to accessing treatment. 39 High self-efficacy is also associated with positive affect and greater physical function. 73 In chronic pain patients, greater levels of pain self-efficacy are protective of psychological health 74 : (1) they moderate the direct effects of pain intensity on depression; and (2) indirectly lower levels of depression and pain by reducing pain catastrophizing.75,76 Importantly for intervention, self-efficacy is a construct flexible to change; pain self-management interventions are effective in increasing self-efficacy, improved physical function, reduced pain intensity and depression.72,75–77 Thus, when considering the psychological decline associated with long waitlists,7,8 enhancing self-efficacy prior to treatment is an insightful psychological prehabilitative strategy in priming patients for engagement once treatment is accessed.78–80
Pain catastrophizing
Screening for pain catastrophizing (PC) during the waiting list provides a key opportunity to stratify patients at-risk of worsening pain. For people living with persistent pain, cognitive rumination, catastrophic thinking and helplessness can develop, increasing pain intensity and interference.73,81 These are interacting dimensions of PC: rumination (negative preoccupation with pain and pain-related fears and thoughts); magnification (the amplification of the salience of pain on one’s health); and helplessness (perceived despair regarding the ability to control the pain experience). 82 Furthermore, evidence shows higher PC at pre-intervention significantly predicts lower engagement in PMPs 81 and attrition. 82 As PC is typically elevated during waitlists, 7 and more broadly, as attrition rates for PMPs are generally high (up to 51%), 83 targeting PC during the waitlist may activate this period of decline to improve PMP completion. Identifying patients with higher PC at point of triage would facilitate optimal implementation of further support, reducing attrition and subsequent healthcare utilisation.
Importantly, PC is amenable to change through psychological intervention. 84 Strategies including pain science education, exercise for pain self-management 85 and cognitive behavioural therapy display reduced levels of PC post-intervention. 86 Moreover, improved PC is also related to greater benefits following multidisciplinary pain management including greater reductions in pain intensity, interference, depression and functional disability by 30%.84,87 Due to the influence of PC on treatment engagement, 81 completion 82 and pain-related outcomes, 88 together, this suggests reducing PC as an effective strategy for prehabilitation efforts within clinical practice.
Clinical recommendations: Prehabilitation within personalised medicine
Psychological prehabilitation is critical in targeting the psychological processes involved in the exacerbation of chronic pain. Thus, utilising the waitlist period for patient stratification according to these psychosocial risk factors (expectations, health locus of control, self-efficacy and pain catastrophizing) within prehabilitation may ultimately enhance treatment retention and PMP completion.52,89 This would provide understanding for whom further support is best directed towards; the patient would receive personalised care before treatment is even accessed. This predictive assessment could be applied easily, simply via the application of widely available psychometrics. The need for personalised pain treatment based on patient characteristics is increasingly recognised.90–92 This cultural clinical shift, led by IASP, emphasises the difference between personalised and stratified care. 90 Stratified care is cost effective, 92 however, personalised care increases patient satisfaction, re-centring clinical focus to that of the gold-standard person-centred approach. 93 Personalised care acknowledges individual differences even within stratified subgroups, taking into consideration the patient’s values and perspective. This encompasses reformulating maladaptive cognitions and beliefs and considering the influence of self-efficacy when determining treatment pathways. 90 Importantly, chronic pain patients express a desire for personalised treatment and self-management strategies. 93 Given that patient expectations are a predominant factor for patient engagement, this would have great influence in reversing the negative cascade to attrition. By improving retention and completion, such psychologically focused pre-treatment intervention would improve healthcare provision on a macro-scale, reducing service and economic burdens in the long-term.
Viable implementation modalities for prehabilitation
Currently, there is no consensus on the best modality for psychological prehabilitation delivery for outpatient chronic pain. There is the risk that while psychological prehabilitation could be valuable, if it is not employed efficiently, it may lead to an additional waitlist for starting prehabilitation itself. However, evidence from surgical interventions suggests that multiple digital modalities are effective.94,95 Pre-surgical digital interventions vary widely in their content; however, they typically include tailored goal-setting, education, cognitive behavioural principles, reminders, activity and sleep logs. 95 An online, self-guided mindfulness-based stress reduction (MBSR) programme encompassing a total of 16 hours audio-video content, comprising 8 primary sessions and 6 additional hours, resulted in significantly reduced pain 30 days after surgery. 96 Lower pain interference, disability and greater physical function was also observed 3 months post-surgery, with mindfulness identified as a predictor of change in physical function 96 and pain interference at 12 months. 94 A self-guided internet-delivered pain-coping skills training also increased self-efficacy for pain management compared to standard controls. 97 In patients with chronic conditions undergoing surgery, a combination of psychoeducation via information booklets and diary keeping significantly reduced postoperative pain compared to standard care. 98 Psychoeducation provided through websites is also superior in improving knowledge and satisfaction regarding pending treatment, compared to a surgical consultation alone. 99 Accessibility, convenience, self-monitoring and progress reports are all key benefits reported by patients undertaking digital interventions while waiting for surgery. 95 Psychological digital prehabilitation strategies can either be guided by a psychologist, or self-guided via watching video content. Each will have different requirement of resources, yet self-guided may be more appropriate for reducing implications on additional waitlists as it will not depend on staff availability to lead the sessions. Thus, due to the effectiveness and lower staff resource requirement, self-guided online psychological intervention may be an efficient implementation style for psychological prehabilitation in outpatient chronic pain. Regarding digital modality, there is greater engagement with mobile apps and Facebook community group pages compared to websites, due to push notifications and reminder functions.100,101 Therefore, perhaps the development of an app comprising education and self-guided cognitive behavioural principles would be effective for an outpatient chronic pain prehabilitation intervention. Such promising evidence for digitally implemented pre-surgical prehabilitation suggests value in exploring such.
Future directions
At present, the evidence base for chronic pain prehabilitation grounded in psychological theory and behavioural science is lacking. 102 Research to develop an innovative prehabilitation intervention to activate the waitlist for pain self-management is required. For maximum impact at an individual and systemic level, it is important such intervention design is grounded in behavioural science. 46 The Behaviour Change Wheel (BCW) 46 provides a structured approach for intervention development, 103 greatly utilised within health policy implementations. Systematic review and meta-analytic evidence suggest rehabilitation practice, with a behaviour change focus, is effective in changing physical activity and eating behaviours in cancer patients. 104 However, no guidelines currently exist for PMP prehabilitation, encompassing patient preferred content, recommendations for delivery, or knowledge of the prospective influence on patient satisfaction. 105 To identify pathways for waitlist intervention design, further research is needed exploring the facilitators and barriers to engagement from the patient perspective, strategically mapped to the COM-B model. Patient involvement is crucial for effective intervention design, as aligned with NICE guidelines of gold-standard care. 98 Thereafter, the Behaviour Change Technique Taxonomy Version 1 (BCTv1) 46 can be applied to identify Behaviour Change Techniques (BCTs) to target specific processes to initiate behavioural action. BCTs including ‘self-monitoring’, ‘instruction on how to perform a behaviour’ and ‘behavioural practice’ effectively increase physical activity adherence in chronic pain patients.102,106 Therefore, this gap needs to be addressed for prehabilitative practice. To rectify inconsistent reporting of behaviour change interventions within literature, 45 the Behaviour Change Intervention Ontology (BCIO), 107 together with the BCIO data extraction template, 107 should be utilised as a comprehensive and systematic framework for high quality reporting of BCIs and their contexts. Doing so will enable the development of an effective, replicable, theoretically grounded prehabilitation waitlist intervention.
Conclusion
Innovative psychological prehabilitation offers a valuable enhancement to current outpatient pain practice. The wholly negative impacts of long treatment delay can be reinterpreted as presenting an underutilised opportunity to target barriers of self-management engagement. Psychological constructs of positive expectations, internal health locus of control, high self-efficacy and low pain catastrophizing all improve pain outcomes and behavioural engagement.47,52,58,108 Critically, these psychological factors are all amenable to change through psychological intervention.23,52,76 To avoid the risk of creating additional waitlists to start prehabilitation itself, digital modalities involving self-guided cognitive behavioural principles and education suggests promise for an effective and efficient implementation style.96,97 Activating the waitlist by intervening during this period, utilising behavioural science principles, could reverse the downward spiral of pain, negative affect and maladaptive cognitions presenting during the waiting period. Health and social care systems could improve efficiency by priming patients for treatment engagement, reducing repeat cycling through failed treatment attempts and excessive healthcare utilisation. Moreover, phenotypically identifying patients with increased susceptibility to treatment failure within the waitlist would enable stratified treatment pathways and enhanced personalised care at the earliest point, optimising treatment outcomes. Significant potential exists to extend psychologically-led prehabilitation intervention beyond PMPs, with application to other clinical waiting lists. Further research is needed to develop such prehabilitation practice which can be applied within health settings worldwide, improving healthcare globally.
Footnotes
Author contributions
All authors made substantial contributions to the study design and interpretation of the data; drafting and revising the manuscript for important intellectual content; and approval of the final manuscript to be published.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.