
Abstract
Introduction
People with persistent pain experience problems modifying their cognition and behaviours when task or environmental demands change – abilities otherwise known as cognitive flexibility. However, limitations and inconsistent results of previous studies raise concerns over the quality of that evidence. We aimed to determine whether people with and without persistent pain differ on two assessments that are commonly used to assess cognitive flexibility. We also examined the relationship between the two assessments and explored whether people with and without persistent pain are distinguishable based on their scores on these assessments.
Methods
Participant demographics and symptoms of anxiety and depression were assessed. Participants completed the Cognitive Flexibility Inventory (CFI) and the Wisconsin Card Sorting Test (WCST). Multiple linear regression on the two outcome variables: CFI (total score) and WCST (% perseverative responses) was applied using backward stepwise selection. Both outcomes were calculated as a standardised proportion of the outcome scale and log-odds transformed to meet the model assumptions. Correlation analysis and logistic regression were used to investigate our secondary and exploratory aims.
Results
Data were available from 128 participants with persistent pain and 68 pain-free controls. After adjusting for covariates, no differences were found between people with and without persistent pain on either assessment of cognitive flexibility. No significant correlations were detected between the two assessments in either group. The probability of having persistent pain was also not associated with scores on either or both assessments.
Conclusion
‘Cognitive flexibility’ appears similar in people with and without persistent pain.
Introduction
Persistent pain, characterised by pain that exceeds the normal time frame required for bodily tissue to heal after injury (i.e. usually >3 months),1,2 is a worldwide health problem. 3 Persistent pain affects approximately 20% of the population4–6 and interferes with many aspects of everyday life including physical, emotional and social functioning. 7 Despite major advances in our knowledge and understanding of persistent pain, important gaps remain. Particularly, the role of cognitive factors in the development of and recovery from persistent pain remains to be fully understood. Uncovering such factors has the potential to lead to more effective and tailored strategies to prevent and treat persistent pain.
One potentially important factor is what is commonly known as ‘cognitive flexibility’. Cognitive flexibility is thought to be a multifaceted construct 8 that broadly refers to the ability to adjust thoughts, and cognitive and behavioural strategies when task or environmental demands change.9,10 There are two approaches to assessing cognitive flexibility – self-report questionnaires and neuropsychological assessments. The Cognitive Flexibility Scale (CFS), 11 the Cognitive Flexibility Inventory (CFI) 12 and the Shift subscale of the Behavior Rating Inventory of Executive Function (BRIEF) 13 are commonly used self-report assessments of cognitive flexibility. Commonly used neuropsychological tests of cognitive flexibility include the Wisconsin Card Sorting Test (WCST), 14 the Trail Making Test (TMT) 15 and the Stroop Test. 16
Several studies have investigated how people with persistent pain perform on neuropsychological assessments of cognitive flexibility, but those studies have yielded contrasting results. Some suggest people with persistent pain perform worse than pain-free controls;17–19 others suggest they do not.20–25 One study 26 found that people with fibromyalgia and people with musculoskeletal pain performed better on the Stroop Test (used here and by others e.g. Johnco et al. 27 as a marker of cognitive flexibility) than pain-free controls, once depression and premorbid intelligence had been statistically controlled for. The mixed findings are difficult to interpret because most studies are underpowered,17,18,20,22,23,25,26 use a combination of assessments and outcome variables without correcting for multiple comparisons,18,22,24,26 or provide insufficient information about the task being used or how outcome variables were calculated.19,23,26 Further, the assortment of neuropsychological assessments and outcome variables that are used to assess cognitive flexibility poses great challenges when comparing results across studies. When data are combined, meta-analyses reveal that people with persistent pain perform worse than pain-free controls on neuropsychological tests of cognitive flexibility,28–31 but high risk of bias of constituent studies leaves some degree of uncertainty. Therefore, although the general pattern of systematic evidence indicates that people with persistent pain are impaired on neuropsychological assessments of cognitive flexibility, there are significant uncertainties around that evidence.
There is a building body of evidence that, although these self-report and neuropsychological assessments both purport to be capturing ‘cognitive flexibility’, they are unlikely to be tapping into shared, or similar, constructs.32,33 In people with and without fibromyalgia, there appears to be a lack of association between self-reported cognitive and behavioural flexibility (i.e. Shift subscale of the BRIEF) and neuropsychological tests of cognitive flexibility (i.e. TMT B-A and WCST sum of perseverative responses). 21 Our two meta-analytic reviews also failed to detect a relationship between self-report questionnaires and neuropsychological tests of ‘cognitive flexibility’ in both clinical (11 studies) 33 and non-clinical (21 studies) 32 cohorts.
With the exception of two cross-sectional studies,21,34 no research to date has examined how people with persistent pain differ from pain-free controls when self-evaluating their ability to be cognitively and behaviourally flexible. Baker et al. 34 found that people with persistent pain reported worse functioning on the Shift subscale of the BRIEF than pain-free controls did, whereas Gelonch et al. 21 reported no differences between people with and without fibromyalgia on both self-report and neuropsychological assessments of cognitive flexibility, after adjusting for depression and anxiety.
It is possible that there may be distinguishable groups of people with persistent pain that can be identified on the basis of their performance on self-report and neuropsychological assessments of cognitive flexibility. Indeed, a study by Attal et al. 35 found that in a cohort of people undergoing surgical procedures for osteoarthritis and breast cancer, the presence of chronic post-surgical pain at 6 and 12-month was significantly predicted by performance on the TMT (part B). However, in people undergoing knee arthroplasty or noncardiac chest surgery, performance on the TMT (B-A) and Stroop (interference T-scores) did not predict the incidence of persistent post-surgical pain 6-month later. 36 To our knowledge, there have been no attempts to predict the presence of persistent pain based on concurrent self-report and neuropsychological assessments of ‘cognitive flexibility’. It seems reasonable to suggest that there may be subgroups of people who are characterised by different patterns of self-reported and neuropsychological assessment results, but more evidence is needed to fill this gap in knowledge. Identifying such patterns may be important because if such groups exist, it would aid in the development of therapeutic approaches that are specifically targeted to individual needs.
The current study had three aims. Our first aim was to determine how people with persistent pain perform on a self-report questionnaire and on a neuropsychological assessment of cognitive flexibility relative to pain-free controls, after controlling for known confounders. We hypothesised that people with persistent pain would, on average, perform worse than their pain-free counterparts on both a self-report and a neuropsychological assessment of cognitive flexibility, even after controlling for confounders. Our second aim was to determine the relationship between self-reported cognitive flexibility and neuropsychologically assessed cognitive flexibility in people with and without persistent pain. Based on previous findings, we hypothesised that the two assessments would not relate. Our third, and exploratory aim, was to explore whether the probability of having persistent pain (or not) is associated with scores obtained on two concurrent cognitive flexibility assessments. No specific hypothesis was generated around this exploratory aim. For a full description of our a priori predictions, refer to the statistical analysis plan, which can be accessed via Open Science Framework (OSF) (https://osf.io/9q8ut/).
Materials and methods
The University of South Australia's Human Research Ethics Committee (HREC) granted ethical approval for this online, cross-sectional study (approval no. 202439). The Checklist for Reporting Results of Internet E-Surveys (CHERRIES) 37 and the STROBE guidelines38,39 were adhered to during the reporting of this study (see Supplemental Files 1 and 2). An a priori protocol was registered and locked under embargo on OSF (https://osf.io/9q8ut/). Deviations from the protocol or statistical analysis plan were recorded and were either outlined in this manuscript, or uploaded and time-stamped on OSF.
Participants
Participants from the general population were recruited using an online, convenience sampling strategy. The study was advertised via recruitment flyers, social media posts, announcements on the Universty of South Australia's Research Volunteers website, and emails that were distributed using previously consented participant mailing-lists and the Research Participation Sign-up System, managed by the School of Psychology, Social Work & Policy, University of South Australia. Participants with or without persistent pain (i.e. pain experienced most days for three months or longer)1,2 were invited to take part in an online survey. Participants were eligible if they were aged ≥ 18 years, had adequate ability to read and understand English, had normal or corrected-to-normal (e.g. glasses or contact lenses) vision, and had access to, and competency with, a computer/laptop or smartphone with internet access. Participants were excluded if they had colour vision deficiencies.
Measures
Primary outcomes
Self-reported cognitive flexibility – the Cognitive Flexibility Inventory (CFI)
The CFI is a 20-item scale that aims to assess: (i) the tendency to realise that challenging situations are indeed controllable; (ii) the ability to perceive different explanations for life incidences and human behaviour; and (iii) the capability to produce multiple alternative solutions to difficult scenarios. 12 The CFI consists of two subscales: the Alternatives subscale (13 items) and the Control subscale (7 items). Respondents are required to indicate the degree to which they agree or disagree with various statements. Each item is rated on a 7-point Likert scale from 1 (strongly disagree) to 7 (strongly agree), with some items being reversed scored. Higher scores on the CFI are considered to reflect greater self-reported cognitive flexibility. The CFI has previously demonstrated high internal consistency, adequate test-retest reliability over a 7-week time frame (r = 0.81, p < .001), and convergent validity with the Cognitive Flexibility Scale. 12 We selected the CFI because unlike other available questionnaires, it was developed with the intention of assessing components of cognitive flexibility that are thought to be adaptive when faced with stressful circumstances. 12 Here, the CFI’s total score was used as an outcome of self-reported cognitive flexibility.
Neuropsychologically assessed cognitive flexibility – the Wisconsin Card Sorting Test (WCST)
The WCST
14
is a card-sorting task that has been widely used to assess cognitive flexibility.27,40 Participants are instructed to ‘match’ 128 response cards, one by one, to one of four stimulus cards that vary in terms of their colour, form and number – see Figure 1. An electronic version of the WCST, which was scored in accordance with the standardised manual,
14
was administered via Inquisit Web – an online software program hosted by Millisecond.
41
Participants were able to match a response card to one of the four multidimensional stimulus cards by clicking on it with either a computer mouse or with their fingertip via a touch-screen. Participants were not provided with direction on how to correctly sort the response cards, but relied only on written feedback (‘correct’ or ‘wrong’) displayed on the screen to determine the correct sorting principle with which to sort the cards by. After 10 correct responses were made in succession, the correct sorting principle changed and participants were required to determine the new sorting principle through a process of trial and error. In line with the recommendations outlined by Miles et al.
42
perseverative responses (percentage score) were used as an indicator of neuropsychological cognitive flexibility. Perseverative responses are continual responses made in accordance to a stimulus dimension that does not match the correct sorting principle, that is, the response is incorrect. However, since the cards are multidimensional and at times ambiguous – that is, a response card has the potential to match a stimulus card on multiple dimensions (e.g. colour and number) – perseverative responses may also be correct. A higher percentage of perseverative responses is thought to reflect poorer neuropsychologically assessed cognitive flexibility. We selected the WCST over other neuropsychological assessments because it most closely aligns with the definition of cognitive flexibility and is widely used in cognitive flexibility research. However, the validity and reliability of the WCST remains to be fully established. Sub-optimal psychometric properties of the WCST may partly stem from varying scoring procedures and administration modalities (i.e. manual or computerised), matters we have covered elsewhere.
42
An illustrative example of the WCST. The single card with one yellow triangle is one of 128 response cards. The four bottom cards from the left-hand side to right hand side: one red triangle, two green stars, three yellow crosses and four blue circles are the stimulus cards.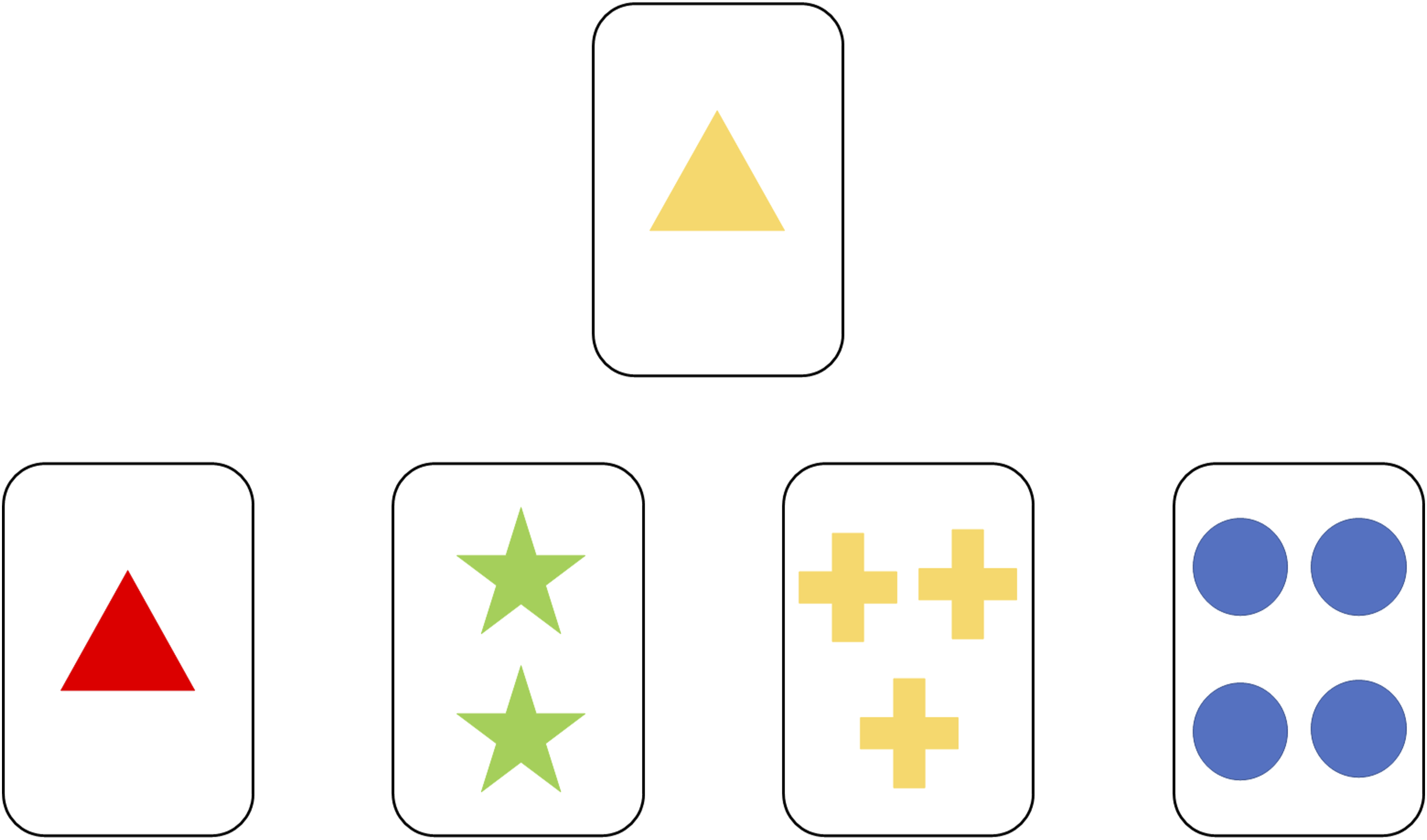
Surveyed demographics
Participants responded to questions relating to age, sex assigned at birth, current gender identity, education level, current activity/occupation, financial situation, place of residence, country of residence, country of birth, refugee status, identification with ethnic or racial groups, mental health, neurological conditions and medication use. Using adaptive questioning, all participants were then asked whether they have persistent pain, defined as ‘pain experienced most days for 3 months or longer’. Participants who responded ‘yes’ to this question were presented with additional questions relating to pain intensity, duration, location(s) and diagnosis (if applicable).
Hospital Anxiety and Depression Scale (HADS)
The HADS is a questionnaire that is used to assess symptoms of anxiety and depression. The HADS consists of 14 items rated on a 4-point Likert scale ranging from 0 to 3. The 14 items are divided into two subscales: 7 items assess depressive symptoms and 7 items assess anxiety symptoms. The scores from each subscale range from 0 to 21, with higher scores reflecting more severe symptoms: 0–7 (normal), 8–10 (borderline abnormal) and 11–21 (abnormal).43,44 The two subscales of the HADS are internally consistent (HADS-D ranging from 0.67 to 0.90; HADS-A ranging from 0.68 to 0.93) and the HADS is a valid and reliable scale, with high sensitivity and specificity (range: 0.70 to 0.90). 45
Procedure
The online survey was developed and administered using Inquisit Web. 41 Participants voluntarily accessed the online survey by following a link that prompted them to install the Inquisit 6 Player application (version 6.5.1) on their chosen device (either a computer or smartphone). Once Inquisit was installed, participants were instructed to click the ‘start’ button, which directed them to an information sheet and consent form. Informed consent was obtained electronically from each participant by selecting the ‘I wish to proceed’ button at the bottom of the page before commencing the study. The introductory page informed respondents about the purpose of the study, the eligibility criteria, the estimated time required for survey completion, the management of data and confidentiality, and that participation was not mandatory even after agreeing to take part. Participants were asked to enter a 6-digit alphanumerical ID code and were then asked to respond to 3 screening questions to confirm their eligibility: (1) are you at least 18 years of age? (2) are you colour-blind? and (3) can you read and understand English? Where participants were not eligible for this study, they were redirected to a page that notified them that they were ineligible to participate in this study and thanked them for their interest.
Eligible participants were asked whether they wished to receive a summary of the results and whether they would like to be contacted about future research being conducted – responding ‘yes’ to either or both items prompted participants to enter their preferred email address in a text-box. Personal information (i.e. email addresses) were removed prior to data analysis and stored separately from the data in a password protected file. Participants were then directed to a demographic questionnaire, self-report questionnaires and the WCST. Data for the Immune Status Questionnaire (ISQ) 46 were collected as part of a larger study, but were not analysed or reported here. The number of questionnaire items was limited to three per page. Questionnaire items were distributed across a different number of screen pages depending on group allocation – 41 pages for people with persistent pain and 36 pages for pain-free controls. Due to the nature of the WCST, presented screen pages varied across participants; the maximum number was 130 (including instruction and completion screen pages). It was compulsory to respond to every question that was presented in the survey, except for demographic questions relating to participants’ life (age, education level, financial situation etc.); however, participants could quit the survey at any time by pressing ‘Alt + E’ on their computer/laptop keyboard or by closing the application on their smartphone. The self-report questionnaires (i.e. CFI, HADS and ISQ) and the neuropsychological test (i.e. WCST) were presented in a counterbalanced order, such that some participants received these tests in the order presented above, while others received the tests in the reversed order (i.e. WCST, ISQ, HADS, CFI). The demographic questionnaire was always presented first. Participants were able to change their responses using a ‘Back’ button up until the point of submitting each of the self-report questionnaires; it was not possible for participants to change their responses during the completion of the WCST.
Upon study completion (or where consent was withdrawn part way through the study), participants were directed to a debriefing form that outlined the true purpose and aims of the study. Participants were then provided with information relating to mental health services, instructions on how to uninstall Inquisit from their device and contact information of the project’s primary investigator. Participants were given up to 1 week after study completion to withdraw their data from being included in the final analysis if they wished to do so. No honorariums were offered for study completion. A small group of colleagues within our laboratory piloted the survey, wherein they provided feedback on the clarity of the demographic items and the functionality of the survey as a whole. All recruitment materials and the full online survey are provided in the Supplementary material (see Supplemental Files 3–9).
Data analysis
Sample size calculation
Sample size calculations were made under the assumptions of the analysis to be performed on the two primary outcomes (see primary analysis for further details) to ensure sufficiently powered primary analyses. Mean and standard deviation estimates of the outcome variables (WCST perseverative responses and CFI total score) in previous studies12,27,47 were used. A detectable increase of 5% for WCST perseverative responses (%) in the persistent pain group than that of the pain-free control group was used, and a detectable decrease of 6 (similarly 5% of the scale) for the CFI (total score) in the persistent pain group than that of the pain-free control group was used. A required sample size of at least 120 would achieve 95% statistical power at the level of significance of 0.05. The sample size calculations were performed using simulation48–50 of a beta distributed response of a linear model data generating process because both outcomes are approximately continuous, skewed and bounded. Sensitivity analysis of the required sample size was also performed using alternative model specifications and a range in the number of covariates and their relative effects. The empirical calculations were verified using analytical multiple linear regression power analysis methods available in G*Power 351,52 and the pwr package 53 in R (version 4.1.3). 54 Sample size calculations were undertaken prior to data analysis, but not prior to data collection. Full details regarding the sample size calculation can be found on OSF (https://osf.io/9q8ut/).
Statistical analysis plan
Data analysis was performed using R (version 4.2.2). 54 Raw data were imported into R using the readr 55 package. Data manipulation was performed using the tidyverse 56 and janitor 57 packages. Data visualisation and figures were created using ggplot2, 58 ggpubr, 59 ggstatsplot 60 and jtools, 61 while diagnostic plots were generated using the performance 62 package. The Classic Color Blind colour palette via the ggthemes 63 package; the Darjeeling1 colour palette via the wesanderson 64 package; the Okabe-Ito colour palette 65 via the colorblindr 66 package; and the base R grDevices 54 package were used in our attempt to make data visualisation more accessible to people who are colour-blind. Descriptive tables were created using gtsummary. 67 Linear and logistic regression outputs were interpreted using the report 68 package. Model equations were adapted from the equatiomatic 69 package. Other packages that were used include writexl, 70 skimr, 71 car, 72 and parameters. 73
We decided a priori that (i) the same user ID indicated duplicate participants and that we would retain the first entry for analysis and exclude any subsequent entries; (ii) data collected prior to participant withdrawal (i.e. non-completion of primary outcomes) would not be analysed and (iii) data would be excluded from statistical analyses if 10 or more identical responses were given in succession on the CFI. No data were missing for any of the variables used to perform our primary analyses, so multiple imputation was not required (refer to the statistical analysis plan on OSF: https://osf.io/9q8ut/). Data for each of the reported non-binary identities did not meet our predetermined sample size (i.e. >5 participants). To protect the privacy and safety of participants, we needed to either (i) combine non-binary gender identities into a third group (providing the reported non-binary gender identities were similar enough to warrant being combined) or (ii) remove them from data analysis. Using The Trans Language Primer,
74
we found that the reported non-binary identities were similar, so we decided to collapse them into a third group, namely ‘transgender and non-binary individuals’. Unless otherwise stated, statistical significance was set at
Primary analysis
Multiple linear regression
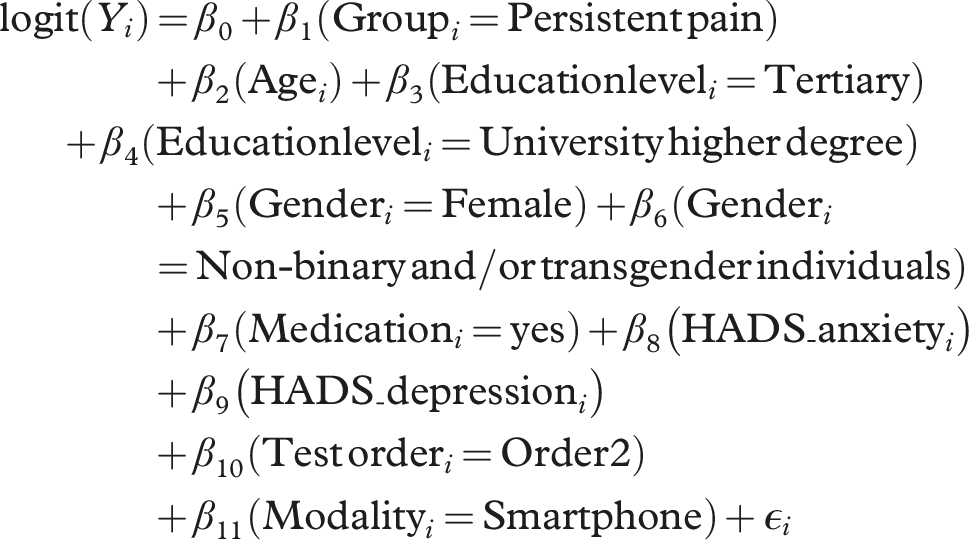
Separate regression analyses were carried out to (i) determine whether people with persistent pain perform worse, on average, than pain-free controls on a neuropsychological assessment of cognitive flexibility and (ii) determine whether self-reported cognitive flexibility is lower, on average, in those with persistent pain than in pain-free controls, after adjusting for confounding variables in both models. The following variables were entered into each model as covariates: age, gender (male, female, non-binary or transgender individuals), education level (high school, tertiary education, university higher degree), medication use (no, yes), HADS depression and anxiety scores, as well as test administration order ([order 1]: CFI first, WCST last vs [order 2]: WCST first, CFI last), and modality of survey completion (computer/laptop vs smartphone). The first level listed in each of the categorical covariates refers to the reference level used. Multiple linear regression with backwards stepwise selection was used to ensure model parsimony to avoid overfitting. 75 The predictor variable of interest was the grouping variable – that is, healthy control (HC) or persistent pain (PP); the outcome variables were the CFI (total score) and the WCST (% perseverative responses), calculated as proportions along their associated scales, herein, referred to as Cognitive Flexibility Inventory proportion of total score (CFI proportion) and WCST proportion of % perseverative responses (WCST proportion), respectively. These proportional outcome variables were transformed via log-odds transformation to satisfy the assumptions of multiple linear regression. Proportions equal to 0 or 1, which would result in undefined logit transformed values, were handled by adding (or subtracting) a half of the smallest unit of the scale. The assumptions of linearity, homoscedasticity of the residuals, influential observations, normality of the residuals and multicollinearity were inspected. Initially, all predictor variables were entered into each regression model to create the full initial models. Predictors with p-values >.05 were then removed in a stepwise manner – removing the predictor with the largest p-value first – until only significant predictors remained in both models. 76 Since the effect of group (i.e. PP or HC) on the two outcome variables (CFI and WCST proportion) was of primary interest, this variable remained in the final models irrespective of the p-value.
The aforementioned covariates were selected based on prior literature. Indeed, performance on the WCST has been found to be influenced by gender, 77 age and education.14,78 Some studies have reported that poor cognitive performance is associated with depression and anxiety.79,80 Further, medications including antidepressants, opioids and anticonvulsants have been found to have both enhancing and detrimental effects on cognitive function.81–83 On the other hand, gender, 84 and symptoms of depression and anxiety have been found to influence scores on the CFI.12,27,85,86 For the purposes of consistency, and that not every demographic characteristic has been previously investigated for its effects on both the CFI or WCST, we decided to enter each of these variables as covariates in the regression models of the two outcomes variables.
The full initial regression models for the i = 1, 2…, 196 participants take the form: • • • • the categorical predictor variables take the form •
Sensitivity analyses were carried out with univariate outliers – CFI or WCST proportion values that fell below Q1 - 1.5 × IQR or exceeded Q3 + 1.5 × IQR – removed, which was visually confirmed via box-plots.
Secondary and exploratory analyses
Correlations
Currently, the relationship between self-reported and neuropsychological assessments of cognitive flexibility remains uncertain in people with persistent pain. To investigate the relationship between a self-report and neuropsychological assessment of cognitive flexibility, raw scores on the CFI subscales (i.e. Alternatives and Control) were correlated with raw perseverative response (%) scores on the WCST in people with and without persistent pain. Separate correlation analyses were performed for the persistent pain group and pain-free control group. Holm–Sidak adjusted significance thresholds (based on the sorted p-values) were applied to account for multiple comparisons and reduce the risk of Type I errors. 87 Holm–Sidak adjusted 95% confidence intervals of the estimated coefficients were also calculated. The assumptions of linearity or homoscedasticity were independently assessed by two authors (CAH, TS), and a third author (GLM) was conferred with when consensus could not be reached. Effect sizes for correlation coefficients were considered small (0.1–0.29), medium (0.3–0.49), and large (>0.5) as recommended by Cohen. 88 Sensitivity analyses were carried out with univariate outliers – CFI (Alternatives and Control subscales) or WCST (% perseverative responses) values that fell below Q1 - 1.5 × IQR or exceeded Q3 + 1.5 × IQR – removed, which was visually confirmed via box-plots.
Logistic regression
Logistic regression was used to explore the probability of the presence of persistent pain based on scores from a self-report and neuropsychological assessment of cognitive flexibility simultaneously. Predictor variables were centred and scaled based on sampled distributions of the observed values. A backward model reduction process was used, with non-significant model terms being removed in a stepwise manner.
The full initial logistic regression model was: • • • • • •


Results
Sample characteristics
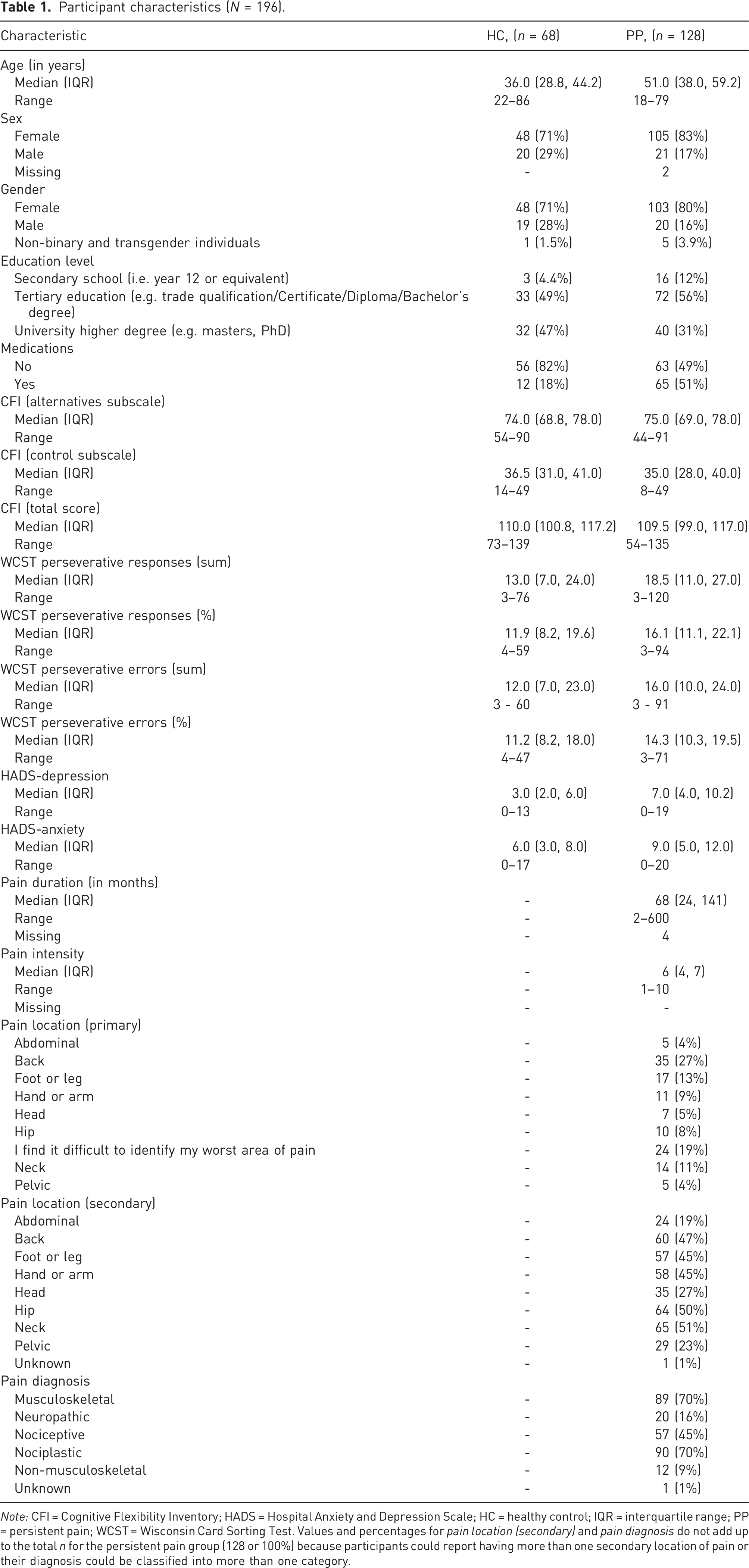
A total of 241 participants (excluding duplicates) accessed the online survey between December 8th 2021 and April 9th 2022. Data from 196 participants were available for analysis (see Figure 2). Participant characteristics are summarised for each group separately using descriptive statistics in Table 1. Continuous variables are presented as values of central tendency (median) and dispersion (interquartile range). The minimum and maximum range of values for continuous variables are also provided. Dichotomous and categorical variables, as well as missing values, are presented as counts and percentages. Mental health conditions were broadly categorised by the primary investigator (CAH) using the Diagnostic Statistical Manual (DSM)-5-TR
89
Complex post-traumatic stress disorder and misophonia were not otherwise categorised because they are not formally recognised in the current version of the DSM.
89
Two experienced physiotherapists (GLM and CB) categorised pain diagnoses. Additional characteristics of the sample are provided in the Supplementary material (see Supplemental File 10). Participant flow diagram. Participant characteristics (N = 196). Note: CFI = Cognitive Flexibility Inventory; HADS = Hospital Anxiety and Depression Scale; HC = healthy control; IQR = interquartile range; PP = persistent pain; WCST = Wisconsin Card Sorting Test. Values and percentages for pain location (secondary) and pain diagnosis do not add up to the total n for the persistent pain group (128 or 100%) because participants could report having more than one secondary location of pain or their diagnosis could be classified into more than one category.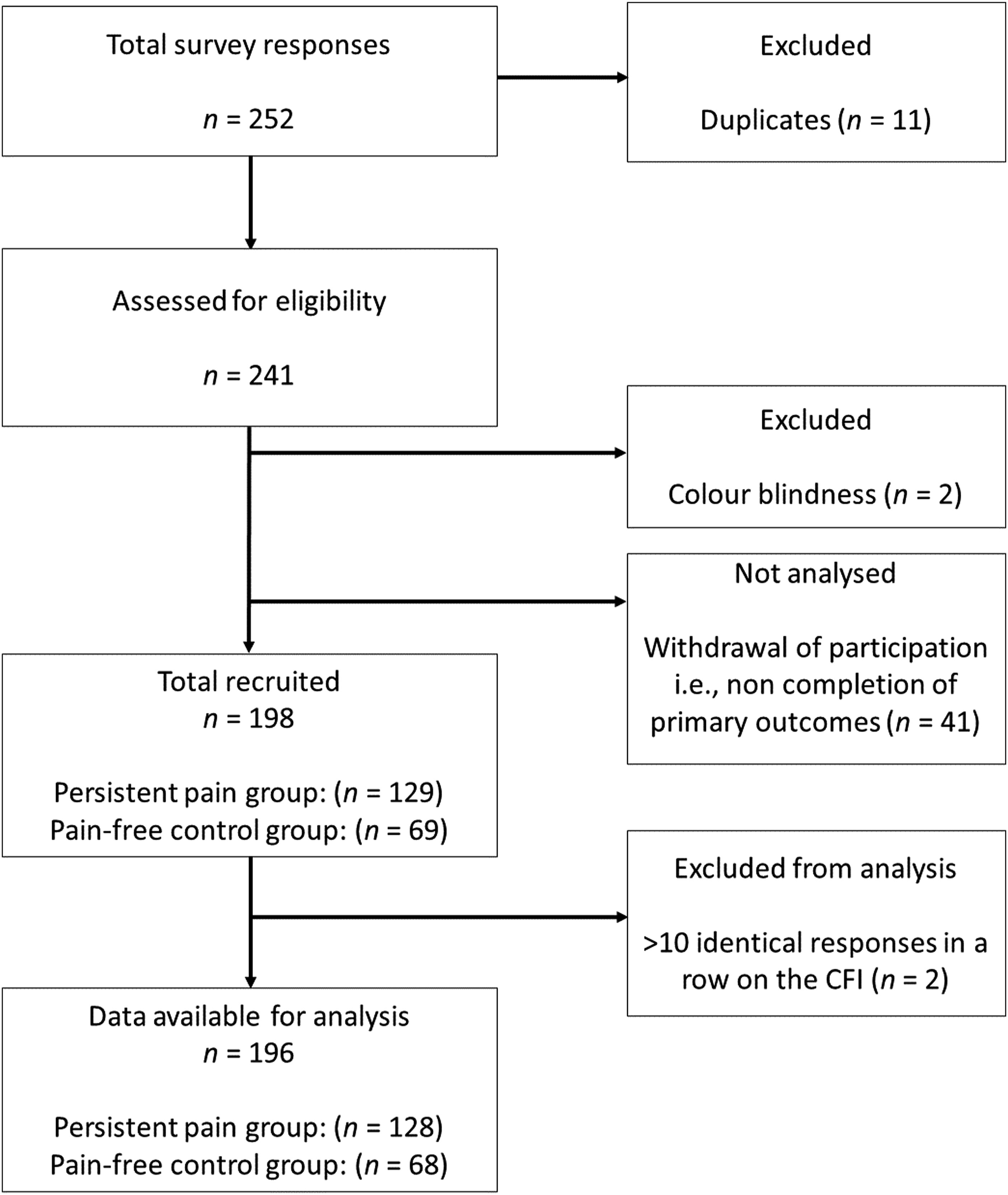
Group comparisons for assessments of cognitive flexibility
Multiple linear regression models were used to assess group differences on two outcomes of cognitive flexibility (CFI and WCST proportion), after accounting for the effects of the aforementioned covariates. Diagnostic plots were inspected for each of the backward selection models and no major deviations from statistical assumptions were observed (see Supplemental File 11).
Final regression model for the CFI (proportion of the total score).
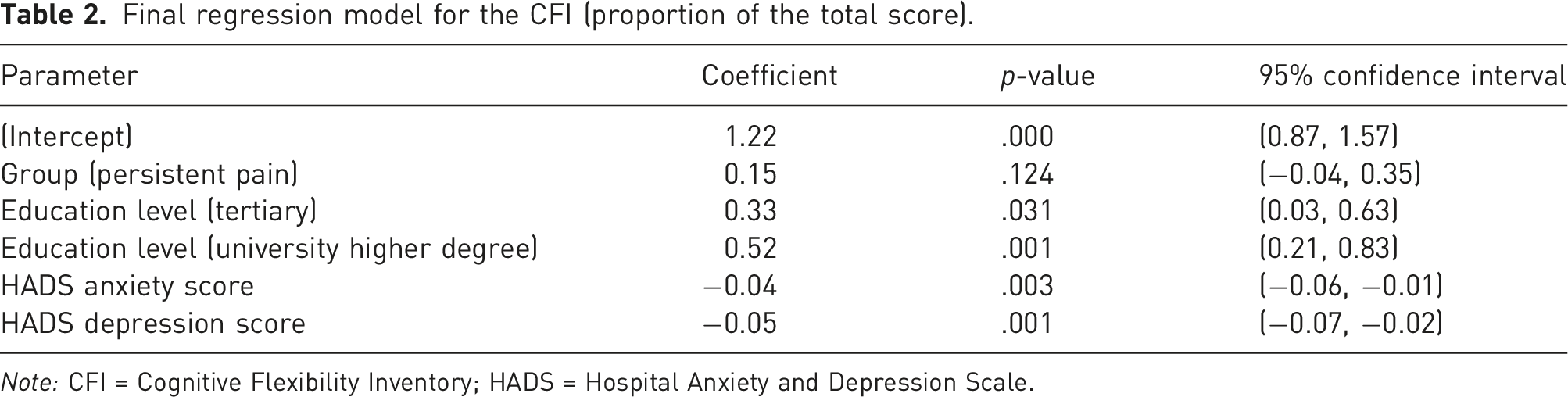
Note: CFI = Cognitive Flexibility Inventory; HADS = Hospital Anxiety and Depression Scale.
Final regression model for the WCST (proportion of % perseverative responses).
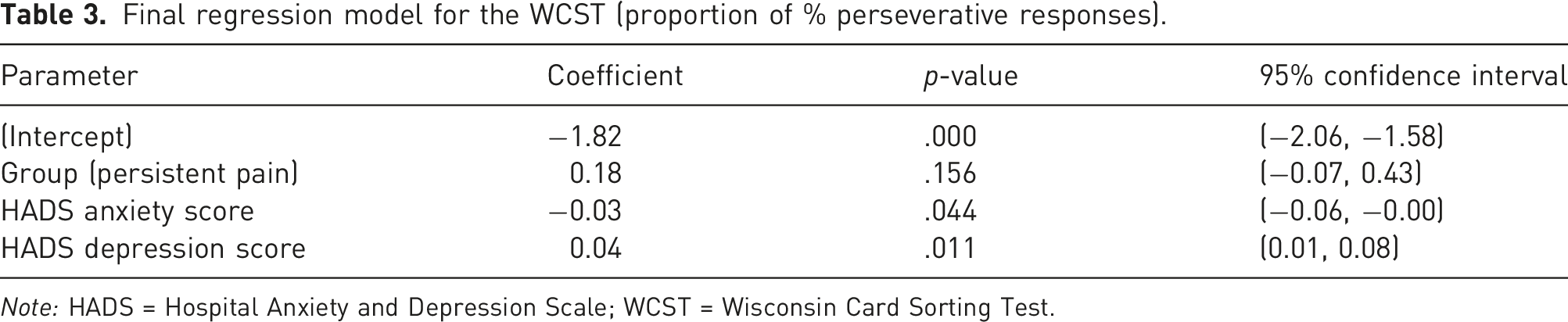
Note: HADS = Hospital Anxiety and Depression Scale; WCST = Wisconsin Card Sorting Test.
Table 3 shows the results of the same process applied to the WCST proportion log-odds outcome. The model was statistically significant (compared to an intercept model), but only explained 5.9% of the variance (
Correlations between assessments of cognitive flexibility
Spearman’s rho correlation coefficients between self-reported cognitive flexibility and neuropsychological cognitive flexibility.
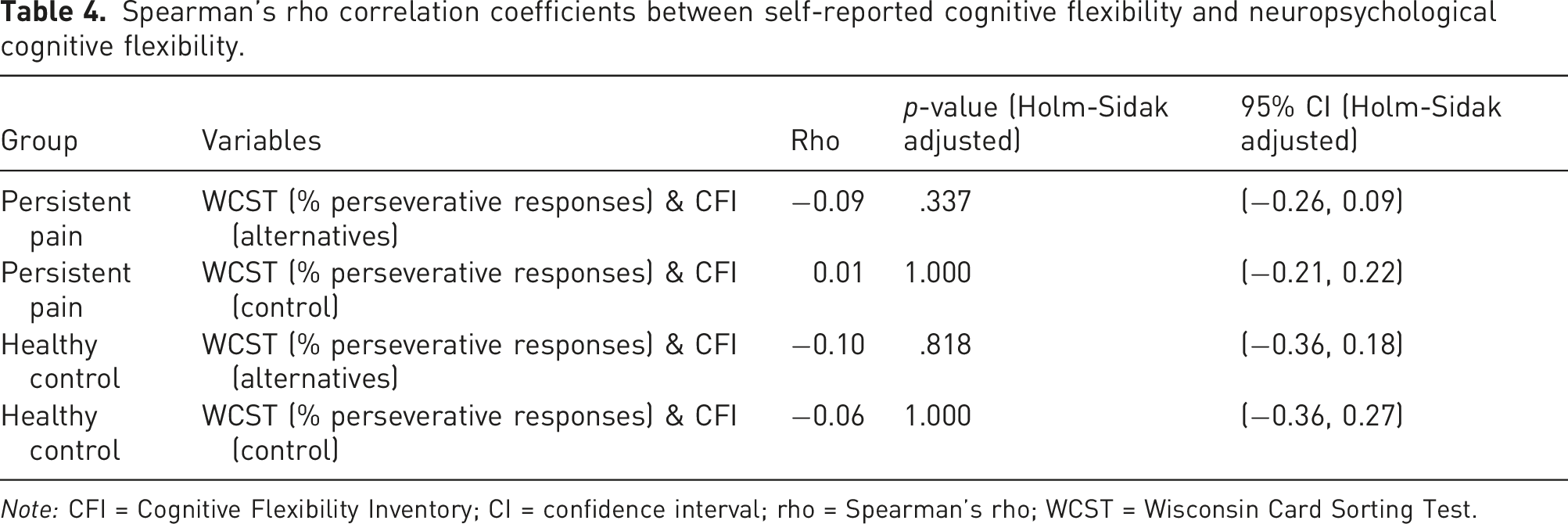
Note: CFI = Cognitive Flexibility Inventory; CI = confidence interval; rho = Spearman’s rho; WCST = Wisconsin Card Sorting Test.
The probability of having persistent pain based on assessments of cognitive flexibility
Model parameter estimates of each logistic regression model fit in the backward selection process.
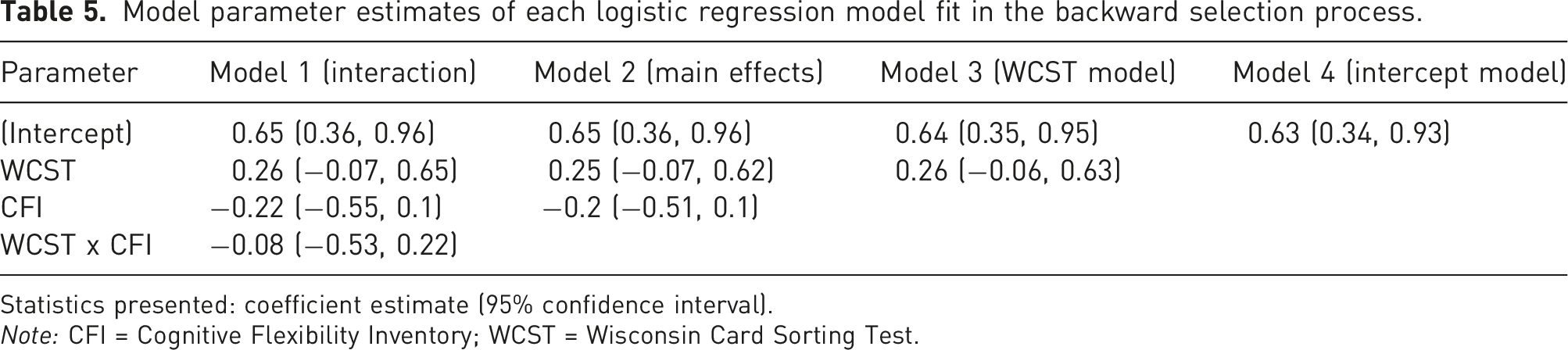
Statistics presented: coefficient estimate (95% confidence interval).
Note: CFI = Cognitive Flexibility Inventory; WCST = Wisconsin Card Sorting Test.
Discussion
Summary of findings
We investigated whether people with and without persistent pain differ in their ability to implement different cognitive and behavioural strategies when faced with changing environmental, or task demands. Contrary to our hypothesis, we found no evidence to suggest that people with persistent pain are different from pain-free controls on either a self-report questionnaire (i.e. CFI) or a neuropsychological test (i.e. WCST), after adjusting for covariates. However, we found that more severe symptoms of anxiety and depression were associated with lower scores on the CFI, and higher educational attainment was associated with higher CFI scores. This finding is consistent with prior research that has demonstrated that self-reported anxiety and depression are negatively related with self-reported cognitive flexibility.12,27,85,86,90 Additionally, once outliers were removed, we found no association between anxiety and depressive symptoms and performance on the WCST – a finding that is also consistent with previous research. 90
Our study supports and extends the work of Gelonch et al. 21 who found that people diagnosed with fibromyalgia are not significantly different from pain-free controls on the Shift subscale of the BRIEF, after controlling for depression and anxiety. By contrast, Baker et al. 34 found that people with persistent pain reported impairments on the Shift subscale of the BRIEF relative to pain-free controls. However, unlike our study and that of Gelonch et al. 21 Baker et al. 34 did not control for the effects of depression and anxiety, and thus it is possible that the observed group differences in their sample could have been largely attributable to negative affect. Indeed, an inverse relationship between self-reported cognitive flexibility assessments and symptoms of depression and anxiety has been identified in people with and without comorbid depression and anxiety, 27 in people with and without anorexia nervosa, 90 and in undergraduate students, 12 providing support for the potential influence of negative affect on self-reported cognitive flexibility. In line with our results, Gelonch et al. 21 also found that people with fibromyalgia were not significantly different from pain-free controls on the WCST (perseverative errors) after controlling for negative affect. Our findings also echo a number of previous studies that have found no differences between people with and without persistent pain on various neuropsychological assessments of cognitive flexibility.20,22–25 However, our findings do not support those of large-scale meta-analyses that have demonstrated that people with persistent pain have small-to-moderate impairments on neuropsychological tests that are used to assess cognitive flexibility.28–31,91
So why then do previous meta-analyses show a small-to-moderate difference between people with and without persistent pain on neuropsychological tests that are commonly used to assess cognitive flexibility? A drawback of meta-analyses is that they, by default, rely on the included constituent studies to account for confounding factors (depression, medications etc.), which could potentially explain the discrepant findings between the current study and previous meta-analytical findings. It is possible that failing to adjust for important confounders in meta-analyses could give the false impression that people with persistent pain have an impaired ability to adapt and implement new strategies when task or environmental demands change, when in fact, these small-to-moderate effects could disappear once relevant confounding factors are controlled for. Further, despite power calculations for meta-analyses being recommended, they are rarely undertaken. 92 Indeed, it remains possible that previous meta-analyses could be underpowered, which could result in an overestimation of the true effect size, and in turn, misleading conclusions.92,93
We also aimed to investigate the strength and direction of the relationship between a self-report questionnaire and a neuropsychological assessment of cognitive flexibility in people with and without persistent pain. As expected, we did not find a significant relationship between our two chosen assessments – the CFI (Alternatives and Control subscales) and the WCST (% perseverative responses) in the persistent pain group, nor in the pain-free control group. Our findings corroborate previous research that indicates that self-report and neuropsychological assessments that purport to assess cognitive flexibility are poorly related. Specifically, Gelonch et al. 21 found no association between a self-report questionnaire (Shift subscale of the BRIEF) and multiple neuropsychological assessments of cognitive flexibility (TMT B-A and WCST perseverative responses) in people with and without fibromyalgia. Our results also support previous studies that have found little-to-no overlap between self-report and neuropsychological assessments of cognitive flexibility in non-clinical27,90,94–96 and other clinical cohorts, including people with comorbid depression and anxiety, 27 attention deficit hyperactivity disorder, 95 anorexia nervosa90,96 and obsessive-compulsive disorder. 97 Our group was the first to undertake two comprehensive meta-analyses that investigated the relationship between a range of self-report and neuropsychological assessments of cognitive flexibility. In both clinical 33 and non-clinical 32 cohorts, we found little-to-no relationship between self-report and neuropsychological assessments of cognitive flexibility. However, a recent study with a large sample (n = 246) of non-clinical, younger adults reported a small, but significant relationship (r = −0.22) between the CFS and the WCST (perseverative errors). 98 One potential explanation as to why our results conflict with that of Grant et al. 98 may be because they used different outcomes and had a much larger (and non-clinical) sample.
The lack of association between self-report and neuropsychological assessments found here and elsewhere is not confined to the construct of cognitive flexibility, but also extends to the executive function literature. 99 While it has been argued that strong correlations would be detectable if self-report and neuropsychological assessments assess the same construct, 99 others have suggested that the non-correspondence between self-report and neuropsychological assessments should not be unexpected since the nature of the two assessments are fundamentally distinct – neuropsychological assessments often provide respondents with specific instructions, and thus are assumed to capture a person’s maximum, momentary ability, whereas self-report questionnaires are thought to capture how respondents perceive their typical behaviours. 100 This may be true, but it seems unlikely to be the only difference between the assessment approaches likely to contribute. Our final and exploratory aim was to determine whether people with and without persistent pain are distinguishable on the basis of their scores on both a self-report and a neuropsychological assessment. Our findings contradict that of Attal et al. 35 but are consistent with that of Vila et al. 36 because we found that the probability of having persistent pain (or not) was not associated with neuropsychological, nor self-reported cognitive flexibility.
Strengths and limitations
The strengths of this study include the preregistration of our protocol, as recommended in all pain research, 101 our statistical analysis plan, our sufficiently powered sample, and that we controlled for confounders. Another strength of this study was that we limited the number of assessments and their respective outcomes, while also controlling for multiple comparisons where appropriate. Doing so addressed the shortcomings of previous studies and minimised the risk of Type I errors. Further, we adopted gender-inclusive research practices; we made the intentional decision to avoid categorising transgender and non-binary people into a single ‘other’ category because such categories reflect ‘othering’ of non-cisgendered people.102,103 This study also has several limitations. First, IP addresses were not collected, so as to protect the anonymity of respondents. Therefore, it is possible that some participants may have completed the survey more than once using different participant ID codes, which may have resulted in duplicate data going unidentified. Although we cannot eliminate such a possibility, this scenario seems unlikely because participants did not receive incentives for their participation. Second, we did not exclude participants who were not naive to the WCST. Given that the WCST is susceptible to practice effects when re-administered within a 12-month time interval,104,105 prior knowledge of the rules that underpin the WCST could potentially yield better scores that are not reflective of enhanced cognitive flexibility, but rather measurement error. 106 Thus, there is a risk that such a decision could have skewed our results. Third, although we used a computerised version of the WCST that scores perseverative responses and perseverative errors in accordance to the Heaton et al. 14 manual, the scores obtained from computerised versions may not be psychometrically equivalent to the manual version. 107 Fourth, although the absence of a researcher during testing is likely to reduce elements of social desirability bias when completing the questionnaires, it meant that we were unable to monitor attention/distraction and other fidelity aspects when participants were undertaking the WCST. Fifth, the categorisation of medication use as a binary (yes/no) response has limitations – in particular, the response options did not allow us to capture dose or to examine whether certain medications have differential effects on the primary outcomes. We also did not assess or control for aspects of pain-related functioning (e.g. pain-related disability, quality of life or pain interference); future investigations using self-report or neuropsychological assessments to assess cognitive flexibility in people with persistent pain conditions should consider controlling for such factors to better understand the association between persistent pain and the ability to adapt cognitive and behavioural strategies in response to changing task or environmental demands. Sixth, we relied on a convenience sampling strategy, so it is possible that our sample, and in turn our findings, were influenced by selection bias,108,109 and our sample was dominantly WEIRD (Western, Education, Industrialised, Rich and Democratic), 110 which limits the generalisability of our results. Seventh, that the data were collected via an online survey meant that we had little control over the comparability of the characteristics between the two samples. In addition, we acknowledge that the sample size of the persistent pain group was larger than that of the healthy control group, but data collection could only be ceased once the minimum required sample size was reached for both groups. We recognise that such scenarios are limitations of conducting online survey studies. Nevertheless, we adhered to the STROBE guidelines,38,39 which provide guidance on how to report sample characteristics in observational studies; the guidelines advise against using inferential statistics, including significance tests, to describe the variability of sample characteristics. Instead, we decided a priori which confounders would be included in our two regression models (informed by previous literature) and removed them using backward-stepwise selection – a widely accepted statistical approach 111 – until the most parsimonious models were reached. Lastly, we did not assess the validity or reliability of the items of the demographic questionnaire due to time constraints; however, the current study would have benefited from such an undertaking to ensure that the questions were precise enough to evoke consistent information from respondents. 109
Implications and considerations
Although there is sufficient evidence to support the notion that persistent pain is characterised by impairments in executive function more broadly,29,112,113 the findings of the current study suggest that the ability to adapt to new strategies in the face of changing demands, which is considered to be one aspect of executive function,8,114 may not be the component of executive function that is problematic in people with persistent pain. It remains possible that our chosen instruments were not sensitive enough to detect problems with self-reported and neuropsychologically assessed cognitive flexibility in people with persistent pain. However, that we found no difference between people with and without persistent pain on both self-report and neuropsychological assessments that purport to capture cognitive flexibility despite having a large sample size, controlling for multiple confounders and restricting the number of assessments and outcome variables used, seems to challenge previous assertions that claim that more sensitive tests or advanced methods need to be developed to assess subtle distinctions in cognitive functioning. 115 Even if subtle impairments on the CFI and WCST do exist between people with and without persistent pain and more sensitive tests are required to detect such impairments, the effects are probably too small to be clinically meaningful.
It is also important to consider the drawbacks of both self-report and neuropsychological assessments of ‘cognitive flexibility’. Self-report questionnaires that are designed to capture cognitive flexibility are likely influenced by the respondent’s capacity to be self-aware and report the information in an accurate and non-biased manner. Similarly, a notorious problem of neuropsychological tests of ‘cognitive flexibility’ is that they inevitably rely on other executive and non-executive processes, which makes interpreting outcomes of such tasks difficult and rather non-specific.116,117 Although previous studies that have used the WCST report no differences in the number of perseverative errors between people with and without persistent pain conditions,24,25 the findings of other neuropsychological tests that are thought to assess cognitive flexibility – such as the TMT – are much harder to reconcile. Some studies have identified impaired performance on part B of the TMT in people with persistent low back pain 19 and fibromyalgia 18 relative to pain-free controls, while other studies have found no differences between people with and without persistent pain.20,24,26 A potential explanation for these contrasting findings may be because the TMT – part B is fundamentally different from the WCST even though they are both used to assess the same construct of ‘cognitive flexibility’. For instance, the TMT – part B requires respondents to alternate between an alpha-numeric sequence (1-A-2-B-3-C etc.) as quickly as possible, whereas the WCST requires respondents to adapt to changing rules during card-sorting. Further, the outcome variables of the WCST and TMT are different: the TMT – part B is typically reported as time in seconds, whereas cognitive flexibility targeting outcomes of the WCST are most often presented as total sum or percentage scores (i.e. perseverative responses or perseverative errors). Although it has been suggested that part B of the TMT reflects, at least in part, cognitive flexibility, 118 the influence of baseline motor speed, which is calculated by subtracting part A from part B, 119 is seldom controlled for. Even when it is, difference scores do not produce adequate reliability coefficients.120,121 For these reasons, future research may wish to steer anyway from relying solely on self-report and neuropsychological assessments to uncover problems in executive function and move towards using more ecologically valid tasks (e.g. the Virtual Cooking Task 122 or the Highway Driving Test 123 ) that require individuals to perform tasks that are relevant to everyday life. Doing so could improve functional outcomes for people with persistent pain; however, it should be noted that such tasks need to be specifically developed and validated for people with persistent pain before their implementation.
It is important to note that our findings are not immediately applicable to what is termed psychological flexibility, which is the main construct targeted by Acceptance and Commitment Therapy (ACT). 124 Cognitive and psychological flexibility originated from different theoretical backgrounds; cognitive flexibility arose out of the neuropsychology field, whereas psychological flexibility has its roots in behavioural psychology, mindfulness and acceptance-based techniques. While there is some empirical evidence that self-reported cognitive flexibility (as assessed via the CFS) and self-reported psychological flexibility (as assessed via the Acceptance and Action Questionnaire-II (AAQ-II)) are related, 98 the specific construct that underpins the AAQ-II has recently been put into question.125,126 Thus, our findings cannot be applied to the construct of psychological flexibility. It is also important to note that although ACT is often used as an intervention to enhance psychological flexibility and facilitate improvement of pain-related functioning in people with persistent pain, 127 currently no data exist on whether people with and without persistent pain differ on outcomes of psychological flexibility. Additionally, learning about key pain concepts – that is, reconceptualising or changing the perception of pain – is valued by people who have recovered from persistent pain.128,129 Clinically, educational interventions that aim to change one’s understanding of pain from a marker of tissue injury to a marker of the need for perceived protection are part of evidence-based pain management. 130 Set-shifting – conceptualised as a core component of cognitive flexibility 131 – is impaired in people with persistent pain. 29 Poor cognitive flexibility may play a role in maintaining pain by undermining one’s capacity to reconceptualise the problem, or shift sets. However, we found no evidence to support the notion that people with persistent pain have poorer cognitive flexibility, leading us to suggest that other components of executive function such as decision making or working memory might play a role in the successful reconceptualisation of the meaning of pain, but future studies are needed.
Conclusion
We found no evidence that people with persistent pain and pain-free controls differ on self-report and neuropsychological assessments that purport to assess ‘cognitive flexibility’. Our study did not find evidence to support the notion that people with persistent pain are less effective than pain-free controls at adapting their cognitive and behavioural strategies when environmental or task demands change. Despite evidence that executive function is compromised in people with persistent pain, our results suggest that ‘cognitive flexibility’ is not how that compromise occurs. However, other confounding factors need to be considered in future research and ecologically valid assessments of ‘cognitive flexibility’ specifically, and executive function, more broadly, will need to be developed before definitive conclusions can be drawn.
Supplemental Material
Supplemental Material - Investigating self-report and neuropsychological assessments of cognitive flexibility in people with and without persistent pain: An online, cross-sectional, observational study
Supplemental Material for Investigating self-report and neuropsychological assessments of cognitive flexibility in people with and without persistent pain: An online, cross-sectional, observational study by Caitlin A Howlett, Tyman Stanford, Carolyn Berryman, Emma L Karran, Valeria Bellan, Scott Coussens, Stephanie Miles, and G Lorimer Moseley in British Journal of Pain.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: GLM has received support from California Institutes of Health; Reality Health; ConnectHealth UK; Workers’ Compensation Boards in Australia, Europe and North America; and AIA Australia. Professional and scientific bodies have reimbursed him for travel costs related to presentation of research at scientific conferences/symposia. He has received speaker fees for lectures on pain and rehabilitation. He receives book royalties from NOIgroup publications, Dancing Giraffe Press & OPTP. CB has received support from Workers’ Compensation Boards in Australia and Kaiser Permanente. All remaining authors (CAH, TS, ELK, VB, SC, and SM) declare no potential conflicts of interest (personal or financial) with respect to the research, authorship, or publication of this manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: CB, ELK and GLM were supported by a National Health and Medical Research Council (NHMRC) Leadership Investigator Grant [ID 1178444] to GLM. CB was supported by a NHMRC Early Career Fellowship [ID 1127155]. ELK was supported by a project grant from Lifetime Support Authority of South Australia. These funding bodies had no role in the study design, collection, analysis or interpretation of the data, writing of the manuscript, or the decision to submit the manuscript for publication.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.