
Abstract
Introduction
There is emerging evidence that posttraumatic-stress disorder may have mediating effects in development of chronic-non-cancer-pain and opioid-use-disorder independently, but its impact on the development of opioid-use-disorder in people with chronic-non-cancer pain is still unclear.
Objectives
(i) Estimate the risk of opioid-use-disorder among individuals with chronic-non-cancer-pain and posttraumatic-stress disorder, relative to those with chronic-non-cancer-pain only, and (ii) identify potential correlates of opioid-use-disorder among people with chronic-non-cancer-pain and posttraumatic-stress disorder.
Methods
This systematic review was conducted as per the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. Longitudinal, epidemiological, cohort, follow-up, retrospective, prospective and cross-sectional studies reporting measures of variance on the likelihood of developing opioid-use-disorder with posttraumatic-stress disorder among individuals with chronic-non-cancer-pain were identified from six-electronic databases (Medline, Embase, Evidence-based Medicine reviews, PsycINFO, Scopus and Web of Science) until December 2022.
Results
Three out of the four studies, which met the selection criteria for this analysis reported statistically significant positive association between risk of developing opioid-use-disorder with posttraumatic-stress disorder among chronic-non-cancer-pain cohort (unadjusted Relative-Risk range: 1.51–5.27) but this association was not evident in the fourth study (adjusted Relative-Risk: 0.96; statistically non-significant), when adjusted for sociodemographic variables. The increased risk was noted particularly with females and chronic musculoskeletal pain conditions.
Conclusions
Posttraumatic-stress disorder can increase the risk of development of opioid-use-disorder among people with chronic-non-cancer-pain and a better understanding of this relationship will help to predict and prevent the development of opioid-use-disorder and may also help in reducing the disability and burden associated with chronic-non-cancer-pain.
Perspective
This review quantifies the risk of developing opioid-use-disorder in the context of posttraumatic-stress disorder among individuals with chronic-non-cancer-pain. Awareness and subsequent practice change will reduce the increasing global burden associated with the chronic-non-cancer-pain.
Introduction
Chronic non-cancer pain (CNCP), defined in the ICD-11 1 as persistent or recurrent pain for at least 3 months, is recognised as a major global health concern. 2 Population prevalence estimates of CNCP vary widely from 8.7% to 64.4% depending on study methodology and characteristics of the sample (e.g. geography, sample age, sex, pain duration or location of pain). 3 There are indications that the prevalence of CNCP may be increasing, with a Danish population survey showing an 8.3% increase between 2000 and 2017. 4 The disabilities and burden associated with CNCP, as reported in the 2019-Global Burden of Diseases Study conducted among people living in 195 countries and territories, lists CNCP conditions among the top-10 causes of disability across most age groups, with chronic low back pain among the leading cause of years-lived-with-disability among adults. 2 This study also reported a gradually increasing burden due to pain conditions (percentage of disability adjusted life-years for low back pain: 1.7% in 1990 to 2.5% in 2019).2,5 CNCP is reported to have a significant negative impact in terms of overall health parameters, quality of life and social functioning. 6 Opioid use disorder (OUD) is defined in the DSM-V 7 as a problematic pattern of opioid use leading to clinically significant impairment or distress. OUD, in the context of CNCP, has become a gradually increasing concern, as opioids remain the most prescribed medication for this cohort despite evidence of limited efficacy and increasing harm. 8 A systematic review of 30-studies reported that on an average, 8%–12% of adults who are prescribed long-term opioids for CNCP will develop OUD, 9 substantially higher than the global prevalence of OUD in the general adult population, that ranges from 0.04% to 4.74%. 10 There is emerging evidence that individuals with CNCP and OUD report higher pain severity, higher pain-related disability and lower functioning compared to those who are on short-term prescribed opioids or no opioids for CNCP.11,12 Additionally, in developed countries such as the USA and Australia, there are patterns of marked increased mortality due to accidental overdose with increased prescribing of opioids for CNCP, so much so that in these counties, more fatalities are attributed to prescription opioids than illicit opioids.13–16 There is increasing evidence to support the ‘adverse selection’ hypothesis that those with CNCP, who have risk factors to develop OUD are often prescribed higher doses of opioids.17,18 There are early indicators that the presence of psychiatric comorbidities may be associated with the development of both CNCP and OUD independently, 19 with increasing reports that PTSD may have a mediating effect in the development of both CNCP and OUD20–22 independently.
The global lifetime prevalence of PTSD in the general population varies from 3.0% to 6.9%, 23 but a meta-analysis of 21-studies reported the pooled prevalence of PTSD among people with CNCP to be 9.7%, about twice that of the general population. 24 Similarly, individuals with PTSD are at 2–3 times higher risk of developing OUD compared to the general population 25 and conversely, individuals with OUD are more than 10-times more likely to meet criteria for PTSD than the general population. 26 Australian studies report higher rates of PTSD in individuals receiving treatment for OUD than in the general population (1.3% in general population compared to 33.2% among those with OUD). 27
Despite the high rates with which these conditions co-occur, few studies have examined the impact of PTSD on OUD among people with CNCP. A recent systematic review of 10-studies by Lopez-Martinez et al., (2019) 28 explored the association between CNCP, PTSD and opioid prescribing patterns. Allten studies were conducted in the USA and six were conducted among veterans only. This review showed that those with comorbid PTSD and CNCP were more likely to be prescribed higher doses of opioids, more likely to be prescribed multiple opioids simultaneously, and were more likely to be taking longer-term prescribed opioids compared to those with CNCP alone. This finding is quite pertinent as there are early indicators that the risk of the development of OUD with prescription opioids for CNCP may be directly related to a higher dose of opioids. Reported rates of OUD increase from 0.7% among those with a daily oral morphine dose up to 36 mg/day, to up to 6.1% among those above 120 mg of oral morphine per day. 29 Similarly, a longer duration of opioid prescribing (above 90 consecutive days) with CNCP is reported to have direct associations with OUD prevalence.29,30 While there is robust evidence of an association between PTSD and OUD in the general population, the impact of PTSD as a risk factor for OUD among individuals with CNCP remains unclear.
Whilst there are some indicators of a relationship, to date, there has not been a systematic review to explore the impact of PTSD on the development of OUD among individuals with CNCP. The current systematic review aimed to (i) estimate the risk of OUD among individuals with CNCP and PTSD, relative to those with CNCP only, and (ii) identify potential correlates of OUD among people with CNCP and PTSD.
Methods
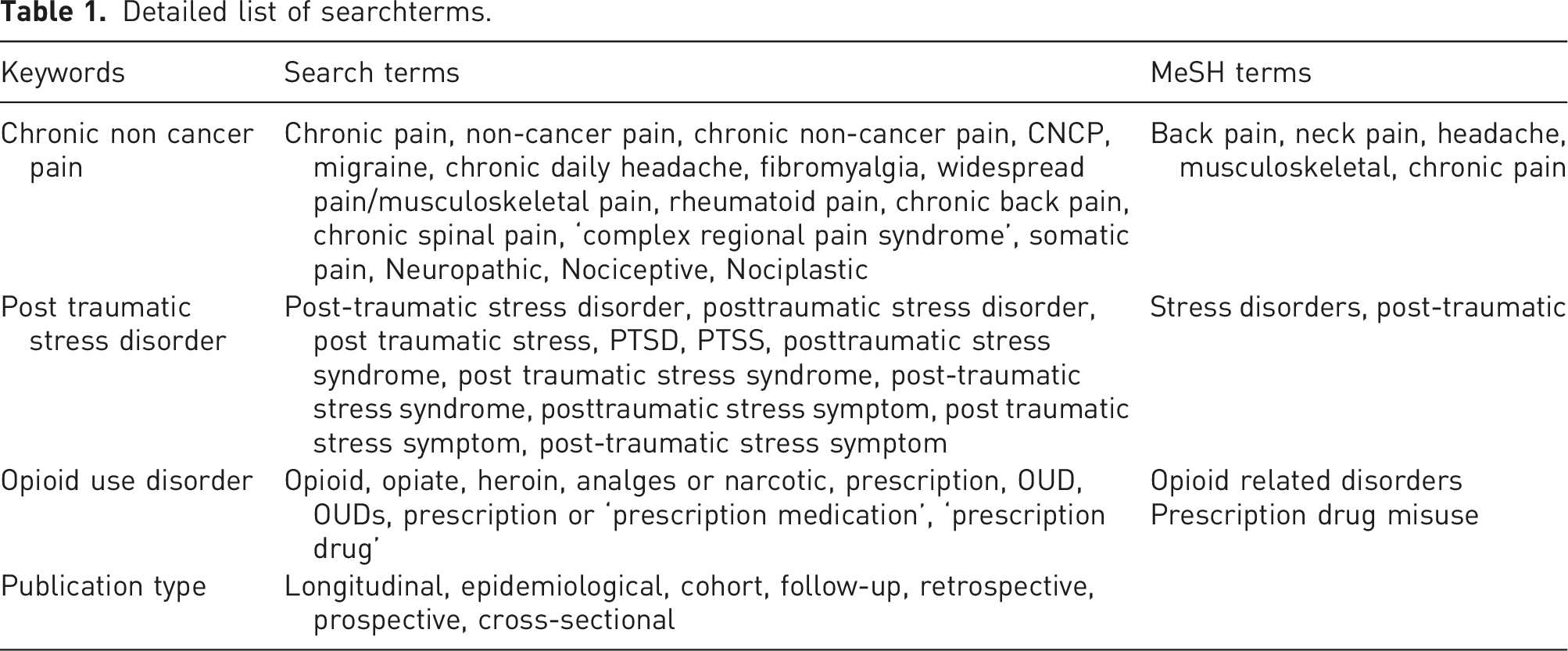
Information sources and search
Detailed list of searchterms.
Protocol and registration
PRISMA 2020 checklist.
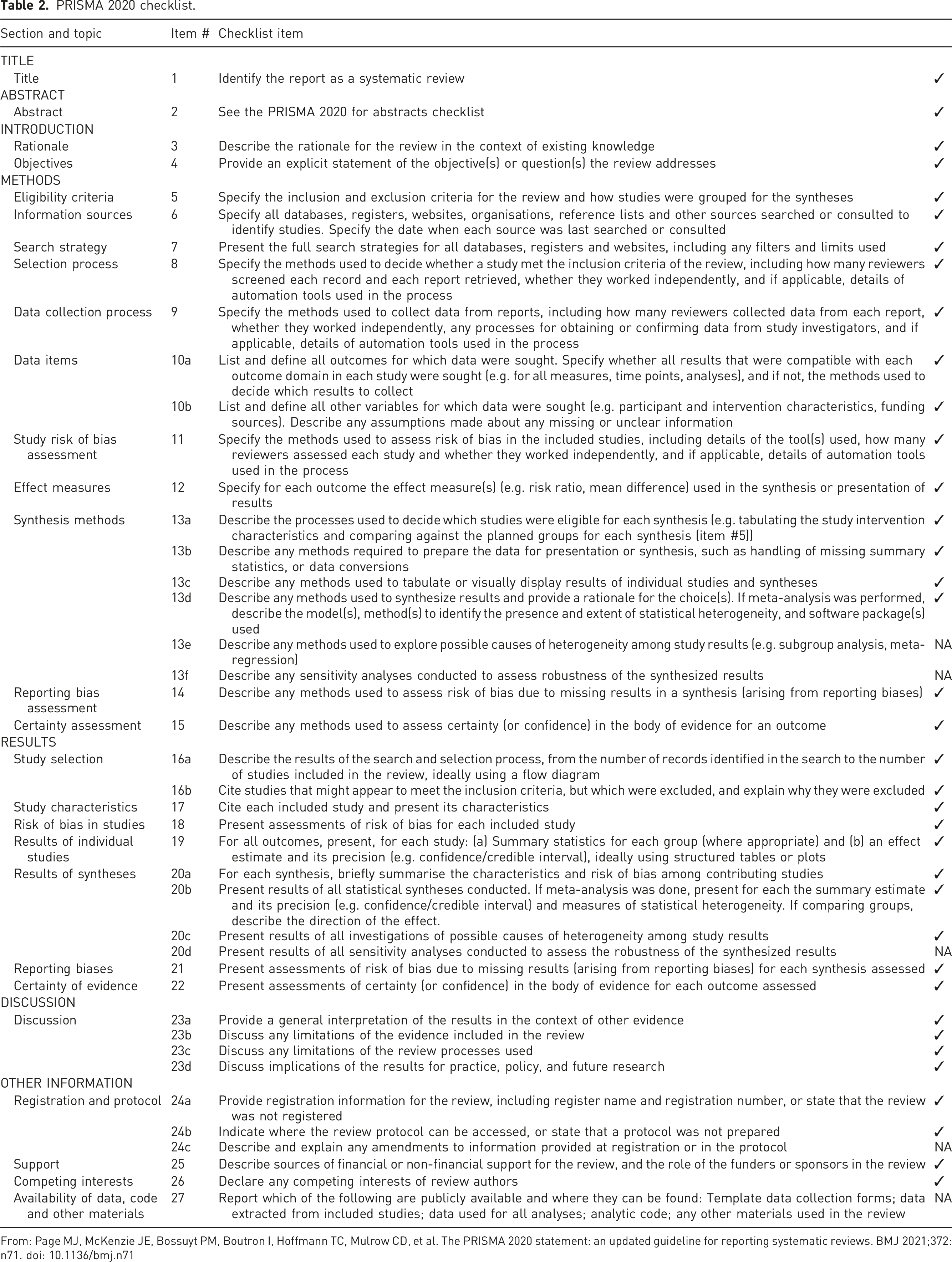
From: Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372:n71. doi: 10.1136/bmj.n71
Eligibility criteria
Studies were included if they met the following inclusion criteria: (a) published in English; (b) reported specific data for PTSD and OUD among the CNCP cohort (rather than ‘mental health’ or ‘substance use issues’ more broadly) (c) provided odds ratios (OR), risk ratios (RR), hazard ratios (HR) or other appropriate measure of effect size with 95% CIs (Confidence Intervals) or other appropriate measures of variance on the likelihood of developing OUD with PTSD among individuals with CNCP. Study types included (d) longitudinal, epidemiological, cohort, follow-up, retrospective, prospective and cross-sectional meeting the above criteria. Studies were excluded if they were non-human studies, included participants below 18 years of age or included participants with cancer pain.
Study selection and data extraction
All studies were screened and extracted using Covidence. 33 Studies were independently screened by two reviewers (AK and JW) in two stages: (a) title and abstract screening, and (b) full text review, where eligibility was assessed and specific reasons for exclusion were reported. Where there were discrepancies, consensus was reached by discussion with one other reviewer (KM).
Data were extracted independently by the two reviewers (AK and JW). The key data extracted and analysed were: first author, publication details, study characteristics, sample size, demographic and clinical characteristics, CNCP measures, PTSD measures, OUD measures, unadjusted and adjusted effect sizes, and variance for the association (odds ratio, risk ratio or other similar measures) between PTSD and OUD among CNCP cohort. To reduce the risk of publication bias, authors of unpublished work (e.g. conference abstracts identified from the above-mentioned databases and cross-referencing of identified studies) were contacted for data.
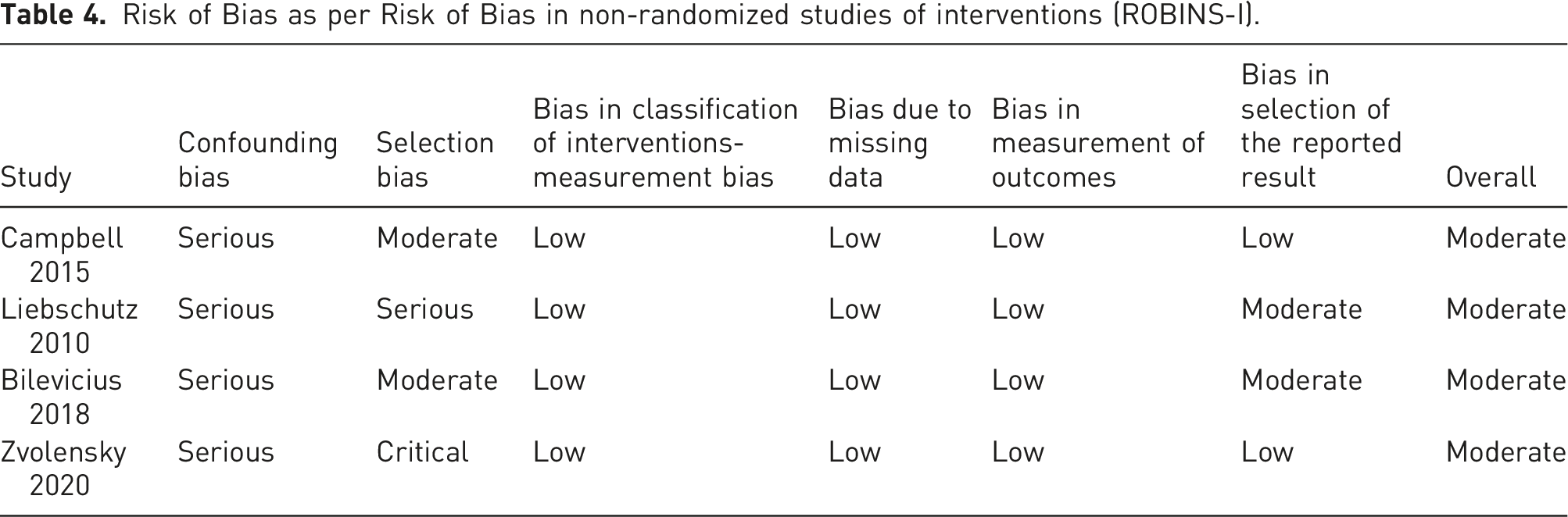
Assessment of the methodological quality
The risk of bias for each study was assessed, using the Risk of Bias in non-randomized studies of interventions (ROBINS-I) tool on the following bias domains: bias due to confounding, bias in selection of participants into the study, bias in classification of interventions, bias due to missing data, bias in measurement of outcomes, bias in selection of the reported results and overall bias. 34 Studies were rated as having ‘low’, ‘moderate’, ‘serious’ or ‘critical’ on each domain of bias separately. The two reviewers (AK and JW) rated the bias separately and consensus was reached by mutual discussion.
Data synthesis and analysis
The current study intended to generate the pooled risk-estimate and the moderating effects of various demographic and clinical factors on development of OUD with PTSD among CNCP cohort using appropriate statistical analysis and potential meta-analytical intent.
Results
Study selection
Study selection is shown in the PRISMA flow-chart in Figure 1. After removing duplicates, 1211 studies were screened for title and abstract. Of the 162 studies that were full text screened, 158 studies were excluded for reasons due to no relationship between PTSD and OUD, cohort being non-CNCP, no OUD or PTSD measures and duplicate data set. Four eligible studies were included for extraction and analysis.19,35–37 The reviewers had high proportionate agreement (Cohen's kappa coefficient: title and abstract screening (k) = 0.86: full text review (k) = 0.86). No additional studies met the selection criteria in the second round of the systematic search. PRISMA flowchart outlining the study selection process.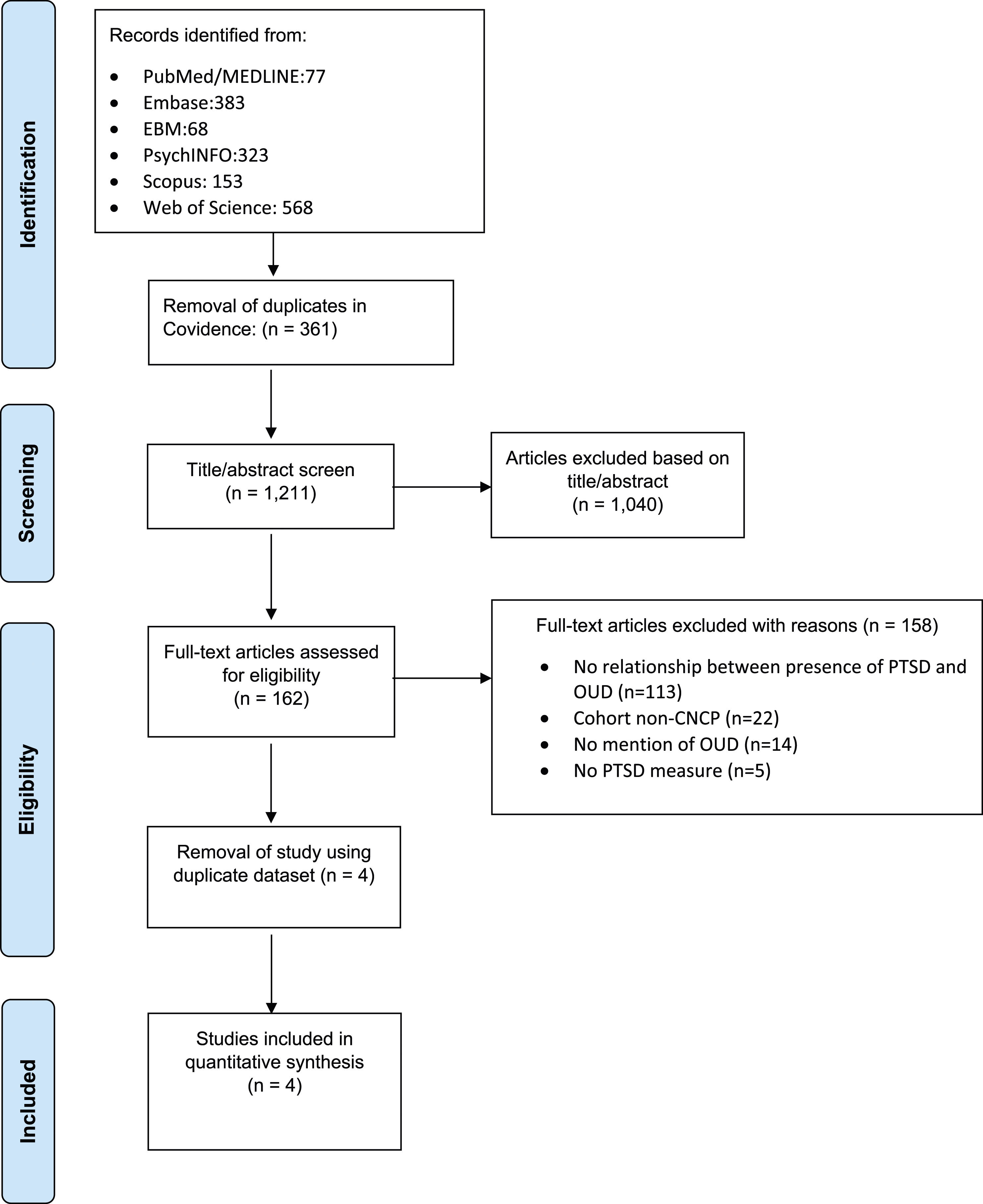
Study characteristics
Summary table of included studies reporting relationship between PTSD and OUD among subjects with CNCP only.
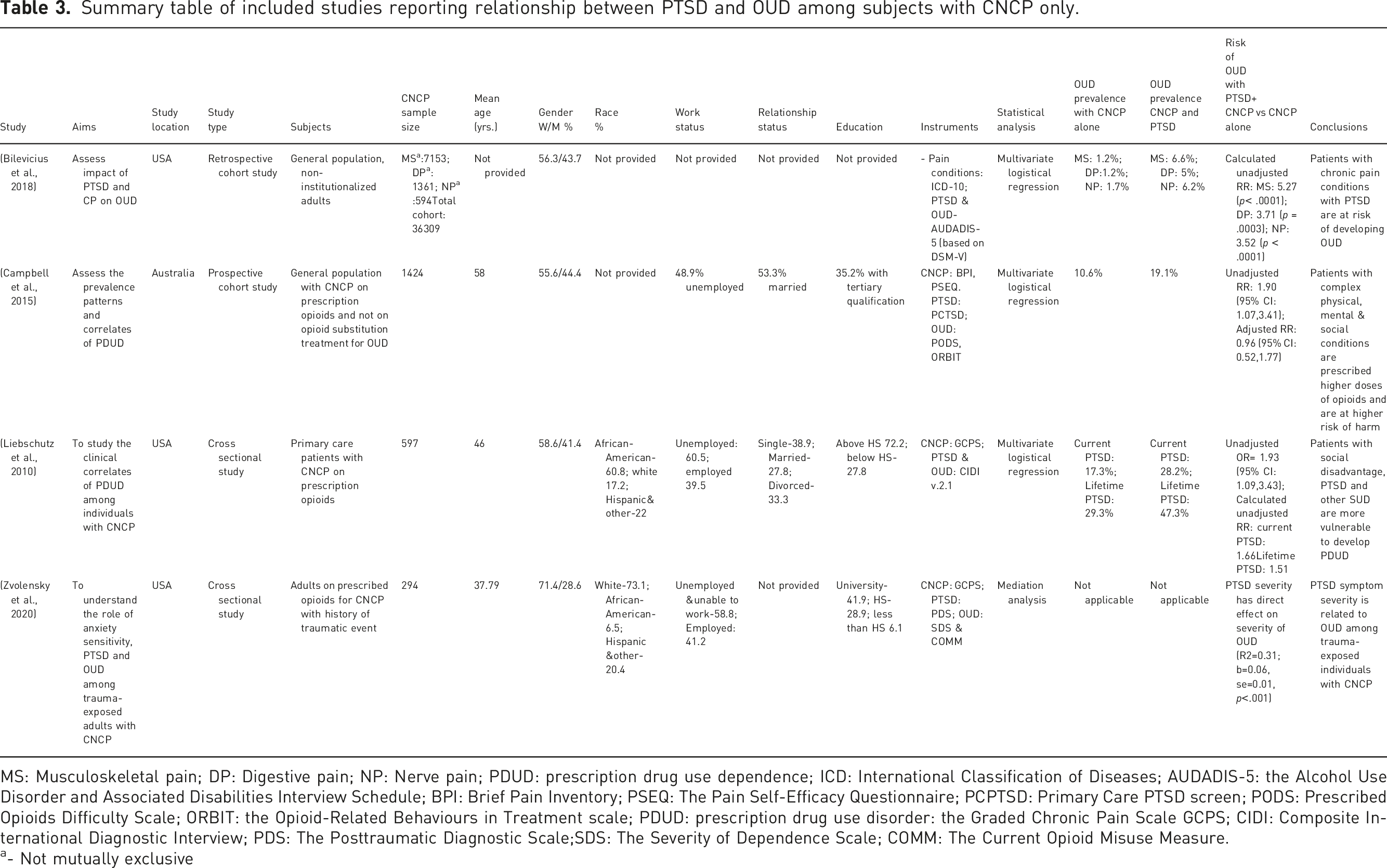
MS: Musculoskeletal pain; DP: Digestive pain; NP: Nerve pain; PDUD: prescription drug use dependence; ICD: International Classification of Diseases; AUDADIS-5: the Alcohol Use Disorder and Associated Disabilities Interview Schedule; BPI: Brief Pain Inventory; PSEQ: The Pain Self-Efficacy Questionnaire; PCPTSD: Primary Care PTSD screen; PODS: Prescribed Opioids Difficulty Scale; ORBIT: the Opioid-Related Behaviours in Treatment scale; PDUD: prescription drug use disorder: the Graded Chronic Pain Scale GCPS; CIDI: Composite International Diagnostic Interview; PDS: The Posttraumatic Diagnostic Scale;SDS: The Severity of Dependence Scale; COMM: The Current Opioid Misuse Measure.
a- Not mutually exclusive
Three studies were conducted in the USA19,35,37 and one in Australia. 36 The studies were published between 2005 and 2018 and all the studies involved had general populations. The CNCP sample size in Bilevicius et al. (2018) for the three non-exclusive CNCP categories ranged from 594 to 7153, and in other three studies19,36,37 ranged from 294 to 1424. The study samples were predominantly females (total mean of 60.4%: range 55.6%–71.4%). Other demographic characteristics of the samples are described in Table 3.
All studies utilised structured or semi-structured clinical interviews based on DSM or ICD to diagnose CNCP, PTSD and OUD. Three studies19,36,37 used brief pain inventory (BPI) or graded chronic pain scale (GCPS) for CNCP and only one study 19 measured the PTSD severity using the posttraumatic diagnostic scale (PDS) and the severity of dependence scale (SDS) for OUD.
Risk of OUD among individuals with CNCP and PTSD
The prevalence of OUD with comorbid PTSD and CNCP ranged from 5% to 47.3%, highest prevalence occurred in those with lifetime PTSD. The RR of having OUD among individuals with PTSD and CNCP compared to CNCP alone, varied from 0.96 to more than 5-times, with the highest risk being associated with musculoskeletal CNCP conditions. The unadjusted models in the three-studies35–37 reported RR ranging from 1.51 to 5.27 (statistically significant). However, adjusted RR (adjusted for sociodemographic variable) reported by one study 36 was 0.96 (statistically non-significant). One study 19 reported a direct correlation between severity of PTSD symptoms with the severity of OUD (bivariate correlation: SDS total score-PDS total score: 0.494; p<.001).
Correlates of OUD among people with CNCP and PTSD
Only one study, Zvolensky et al. (2020), 19 reported impact of sociodemographic measures on development of OUD with PTSD and CNCP, and reported a direct correlation between severity of OUD with younger age (0.162: p<.001) and females (0.218; p<.001). Higher odds of developing OUD with CNCP alone were reported with younger age by one-study 36 and with males by two-studies.36,37 Among PTSD and CNCP cohort, only one-study 19 reported a direct association between severity of OUD with the pain intensity (0.219; p<.001).
Quality assessment
Risk of Bias as per Risk of Bias in non-randomized studies of interventions (ROBINS-I).
Discussion
This systematic review examined the risk of OUD with PTSD among individuals with CNCP. Four studies were identified as eligible for inclusion and were rated to have acceptable methodology and quality. Three studies19,35,37 on unadjusted models found there to be a higher risk of development of OUD with PTSD among CNCP cohort (unadjusted RR range: 1.51–5.27; statistically significant), but this association was not evident in the fourth study 36 (adjusted RR: 0.96; statistically non-significant) when adjusted for sociodemographic variables. This variation may be due to variability in sample and methodological characteristics including variation in the instruments used to measure each construct. Our findings expand on those reported by the recent systematic review 28 examining the association between PTSD, CNCP, and opioid prescribing even though our study demographics were contrasting. Our review had three studies from the USA, one from Australia, and included participants from the general population and were predominantly females. This compared to the systematic review 28 where all included studies were conducted in USA and had predominant male and veteran participants.
We found that those with chronic musculoskeletal pain conditions and PTSD had the higher risk of OUD (more than 5-times), while those with nerve pain conditions and PTSD had the lowest (unadjusted RR: 3.52), compared to those with CNCP alone. This has been highlighted in other studies.18,39,40 Individuals with musculoskeletal pain conditions and PTSD, may have a higher burden of trauma-associations and pain-memories which could create a bigger reward deficit and later higher euphoric effects with opioids. It is hypothesised that the reward deficit and the euphoric effects with opioids may be significant contributors to the development of OUD.35,39,40 Neuro-imaging studies demonstrate that individuals with PTSD show changes in brain function in regions of the hippocampus, anterior cingulate cortex, and medial prefrontal cortex in the form of increased levels of noradrenaline and decreased levels of dopamine, both of which prime the individual towards heightened opioid related cues and subsequent development of OUD. 39 Further studies are needed to examine the impact and modifiers of this correlate on development of OUD among individuals with CNCP and PTSD. This will help in developing a better understanding of the trauma-pain relationship and is likely to assist in development of trauma-informed care in pain-management. Trauma-informed care is based on the foundational premise of accepting the ubiquitous prevalence and lifelong impact of trauma on an individual living with CNCP and utilises a biopsychosocial approach to provide a safe and trustful environment to empower the individual towards a holistic pain-management treatment. 41 Our findings are also in line with those of four other studies42–45 that examined the relationship between CNCP, PTSD and non-medical use of prescription opioids (not diagnosable as OUD and hence these studies did not meet the eligibility criteria for this review). These identified four-studies42–45 reported a significant association between PTSD and non-medical use of prescription opioid among the CNCP individuals. These studies recommended need for further systematic studies to quantify the high-risk opioid behaviours in people with PTSD and CNCP and how the risks compare to OUD in other contexts, including an examination of clinical correlates that may assist in identifying at-risk individuals.
This review found that few studies examined clinical correlates for development of OUD among CNCP and PTSD, especially in view of the finding by Campbell et al., (2015), 36 where adjusted model did not show the association. While there is limited evidence pointing at the relationship of female sex with the severity of OUD among patients with PTSD and CNCP 19 , more studies are needed examining the role of sex. It is pertinent considering that multiple studies have pointed out that female sex is more likely to be independently associated with both CNCP and PTSD.46–48 The impact of various sociodemographic background factors such as race, level of education and income, on development of OUD with PTSD and CNCP, remains inconclusive and further studies are needed. Also, the combined impact of OUD, PTSD and CNCP on an individual’s psychosocial functioning and quality of life needs further exploration. Similarly, there is some indication that individuals with OUD, PTSD and CNCP suffer higher pain intensity, which has also been reported by Lopez et al. (2019) 28 among individuals with CNCP and OUD. However further studies both cross-sectional and longitudinal are needed to elucidate the added impact of PTSD on various health related disabilities with OUD and CNCP.
Our study has some limitations: firstly, due to significant heterogeneity between studies in relation to demographic characteristics, outcome measures and results, a meta-analysis to assess the risk of OUD with PTSD among the CNCP cohort was not possible. Based on our synthesis, the association between OUD with PTSD among CNCP cohort is indicative but not yet conclusive. Secondly, we have been unable to establish any specific correlates for development of OUD with PTSD and CNCP; however, demographic measures especially sex needs further evaluation.
Consequent to our review, we would like to highlight various gaps in the existing literature, which could be addressed in future studies. Firstly, there is need for further research to explore the impact of PTSD on development of OUD among CNCP cohort for more conclusive findings to be derived. Secondly, there is lack of uniform definition and measures for CNCP among studies which reduces the research consistency. Thirdly, there are significant challenges with diagnosing OUD with prescription opioids for CNCP. It has been strongly proposed49,50 that the mere presence of neuroadaptation to opioids (tolerance, withdrawal symptoms and strong desire to avoid withdrawal symptoms by repetitive use), should not be considered enough for diagnosing OUD, which is now also highlighted in the DSM-5. 7 Fourthly, there are significant gaps in understanding of the role and the impact of the sociodemographic and psychological correlates on development and maintenance of OUD with CNCP. And lastly, the longitudinal impact of this triad in terms of disability and burden on an individual is still unclear.
Conclusion
Although there is substantial evidence suggesting a clear and bi-directional association between OUD and PTSD,25–27,51,52 this relationship is not clear among people with CNCP due to limited research in this area. However, the predominance of research to date suggests that PTSD is associated with OUD among people with CNCP. Further studies are needed to understand the relationship between PTSD and OUD among the CNCP cohort and the consequent health burden. Trauma-informed care 41 for CNCP individuals may help to prevent the development of OUD and may also help in reducing the disability and the burden with CNCP.
Footnotes
Author contributions
All authors equally contributed to this paper and read and approved the manuscript. AK & JW were involved in study screening and data extraction.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Contributorship
All authors equally contributed to this paper and read and approved the manuscript. Authors-AK & JW were involved in study screening and data extraction.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Trial registration
ROSPERO Identifier: CRD42021289900