
Abstract
Background
Chronic pain is a disabling condition. Many people with chronic pain seek informal support for everyday activities of daily living (ADL). However, there remains uncertainty on the type of people with chronic pain who access this support, what types of support they need and who provides such support. The purpose of this analysis was to answer these uncertainties.
Methods
Data from the Health Survey for England (HSE) and English Longitudinal Study of Ageing (ELSA) were accessed. People who reported chronic pain (moderate or above for minimum of 12 months) were identified. From these cohorts, we determined if individuals self-reported receiving informal care. Data on caregiver profiles and caregiving activities were reported through descriptive statistics. Logistic regression analyses were performed to compare health status outcomes between people with pain who received and who did not receive informal care.
Results
2178 people with chronic pain from the ELSA cohort and 571 from the HSE cohort were analysed. People who received care were frequently female, older aged with several medical morbidities including musculoskeletal diseases such as arthritis. People with chronic pain received informal care for several diverse tasks. Most frequently these related to instrumental activities of daily living (IADL) such as shopping and housework. They were most frequently provided by partners or their children. Although they reported greater disability and symptoms (p < 0.001), people who received care did not report differences in health status, loneliness or wellbeing (p = 0.27; p = 0.46).
Conclusions
Whilst it may be possible to characterise people living in chronic pain who receive informal care, there is some uncertainty on the impact of informal caregiving on their health and wellbeing. Consideration should now be made on how best to support both care recipients and informal caregivers, to ensure their health and quality of life is promoted whilst living with chronic pain.
Introduction
Chronic pain is a disabling condition for all ages of people. 1 It has been defined as pain that persists or recurs for more than 3 months. 2 Chronic pain may arise from several sources including musculoskeletal (bone, joint, muscle), or neurological origins, cancer or infection. Many people have more than one body region affected. 3 Globally, chronic pain is a leading cause of years lived with disability in people aged 70 years and over. 4 Low back pain (LBP) is a top 10 leading cause of disability worldwide. 4 Approximately 9.1 million people live with long-term back pain in England. 5 Chronic pain poses a personal cost to the individual and their friends and family and adds a burden onto health and social care services.6,7 Accordingly, national and international policies on chronic pain management are currently focused on a multimodal approach, increasing self-management skills, reducing opioid use and prioritising non-pharmacological treatments for pain were possible.8–12
Chronic pain is a common problem among older people. 13 Whilst conflicting evidence exists related to differences in pain processing and treatment response in older compared to younger people with chronic pain, 14 there has been limited evidence exploring different treatment approaches between age-groups. However, because of medical comorbidities and associated polypharmacy, managing symptoms in older people with pharmacological and non-pharmacological approaches, can be challenging. 15 Furthermore, chronic pain increases falls-risk for older people. 16 Given fall-injuries are a leading cause of death in older adults, 16 this is a particularly important health challenge for an ageing population.
People living with chronic pain, whether younger or older, frequently have difficulties managing symptoms and everyday activities to maintain independence and quality of life. 17 Consequentially, they often access support for tasks such as: washing and dressing, preparing meals, eating, housework or shopping.18,19 This caregiving may be formal or informal. Formal care is the provision of care by someone who is paid. Informal care is provided without direct financial payment.
There remains uncertainty over the profile of people living with pain who access informal care, and what care provision constitutes for them. Accordingly, the purpose of this study was to determine, in a representative cohort in England: (1) the profile of people with chronic pain who receive informal care (2) who provides informal care for people living with chronic pain (3) how much informal care people with chronic pain receive (4) which activities do people with chronic pain receive support (5) whether there is a difference in health status between people with chronic pain who receive informal care compared to those who do not.
Materials and methods
We conducted a comparative prospective cohort study reported using the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 20
The characteristics and profile of people resident in England, who reported moderate chronic pain or greater, from two published cohorts, were analysed. These cohorts were: (a) The English Longitudinal Study of Ageing (ELSA). This commenced in 2002 and is an ongoing study of the health, social and economic lives of a cohort of people aged 50 years and older in England.
11
It is a nationally representative household survey that monitors trends in the population’s health every 2 years.
21
(b) The Health Survey for England (HSE). This is an annual survey administered since 1991 to monitor trends in national health and to estimate the prevalence of specific health conditions. This collects data during an interview on sociodemographic characteristics, employment, health conditions and clinical measurements.
English Longitudinal Study of Ageing and HSE data are publicly available and were downloaded from the UK Data Service (https://ukdataservice.ac.uk/). Both cohorts were selected as they provide data on caregiving and care receipt for people with moderate pain or greater and offer different measures of health status to indicate the broader impact of caregiving on health and wellbeing.
Wave 7 (June 2014 to May 2015) ELSA data and the HSE (January 2019 to March 2019) data were identified as the most pertinent and contemporary to offer the required cross-sectional variables on caregiving and pain data to answer our research questions.
Participants
From each dataset, we identified people who self-reported with moderate pain or greater. English Longitudinal Study of Ageing categorised this as individuals with self-reported moderate or severe pain; HSE categorised this as a self-report of moderate, severe, or extreme pain. To provide greater certainty that self-reported pain reflected the intended ‘chronic pain’ population, we compared the responses against the visual analogues scale (VAS) assessment of LBP, hip, knee and foot pain (0–10 point scale). To ensure participants were those who experienced persistent symptoms (12 months minimum), all participants were required to report pain severities of moderate or greater at both the analysed and previous ELSA/HSE data collection interval to be included in our analysis.
To determine whether a participant received or did not receive informal care, we determined care receipt, for each dataset, as a composite of the response to (1) the number of informal caregivers assisting (ELSA/HSE), (2) requirement for assistance responses (ELSA) and (3) whether they received help with activities of daily living (ADLs) such as washing, dressing, eating or instrumented ADLs (IADLs) such as shopping, travelling and managing medicines (HSE). These were considered appropriate as reflective of the wide-range of activities an informal caregiver may offer an individual they support.17–19
Variables
Variables selected to answer the four a priori research questions from the ELSA/HSE informal caregiving analysis.

ELSA– England Longitudinal Study of Ageing; HSE– Health Survey of England; LBP– Low Back Pain; VAS– Visual Analogue Scale
Statistical analysis
Analyses were performed as complete case analyses in each cohort separately. English Longitudinal Study of Ageing longitudinal weights are only available for core sample participants. Applying longitudinal weights to our analysis would have resulted in a reduction in analytical sample size and therefore reduced statistical power. Consequently, we used the unweighted sample for our analyses.
We performed descriptive analyses on the characteristics of care recipients using means and 95% confidence intervals (CI), medians and inter-quartile ranges (IQR) or frequencies with percentages to answer the research questions: (question 1) description of the profile of people with chronic pain who receive informal care; (question 2) who provides informal care for people living with chronic pain; (question 3) how much informal care do people with chronic pain require; and (question 4) for which activities do people with chronic pain frequently require support. We presented the duration of informal caregiving, by the individual providing the care, using stack bar charts.
To assess whether there is a difference in health status between people with chronic pain who receive informal care compared to those who do not (research question 5), we performed logistic regression analyses for dichotomous data presented with odd ratios (OR) and 95% CI and linear regression analyses presented as mean differences (MD) and 95% CI for continuous data. All p-values generated from the analyses were considered statistically significant if p < 0.05.
Analyses were performed using Stata/MP 17.0 for Windows (StataCorp LLC, Texas 77845, USA).
Results
Sample characterises
Figure 1 illustrates the derived and analysed cohorts from the Wave 7 ELSA and HSE 2018 datasets. As this illustrates, from the 9666 respondents in the ELSA cohort, 1045 people with moderate or severe pain received informal care compared to 1133 respondents who did not. From the 10,250 HSE cohort, 1361 participants reported moderate, severe or extreme pain. Of these, 356 received informal care whereas 215 did not. Flow chart illustrating cohort composition from respective datasets.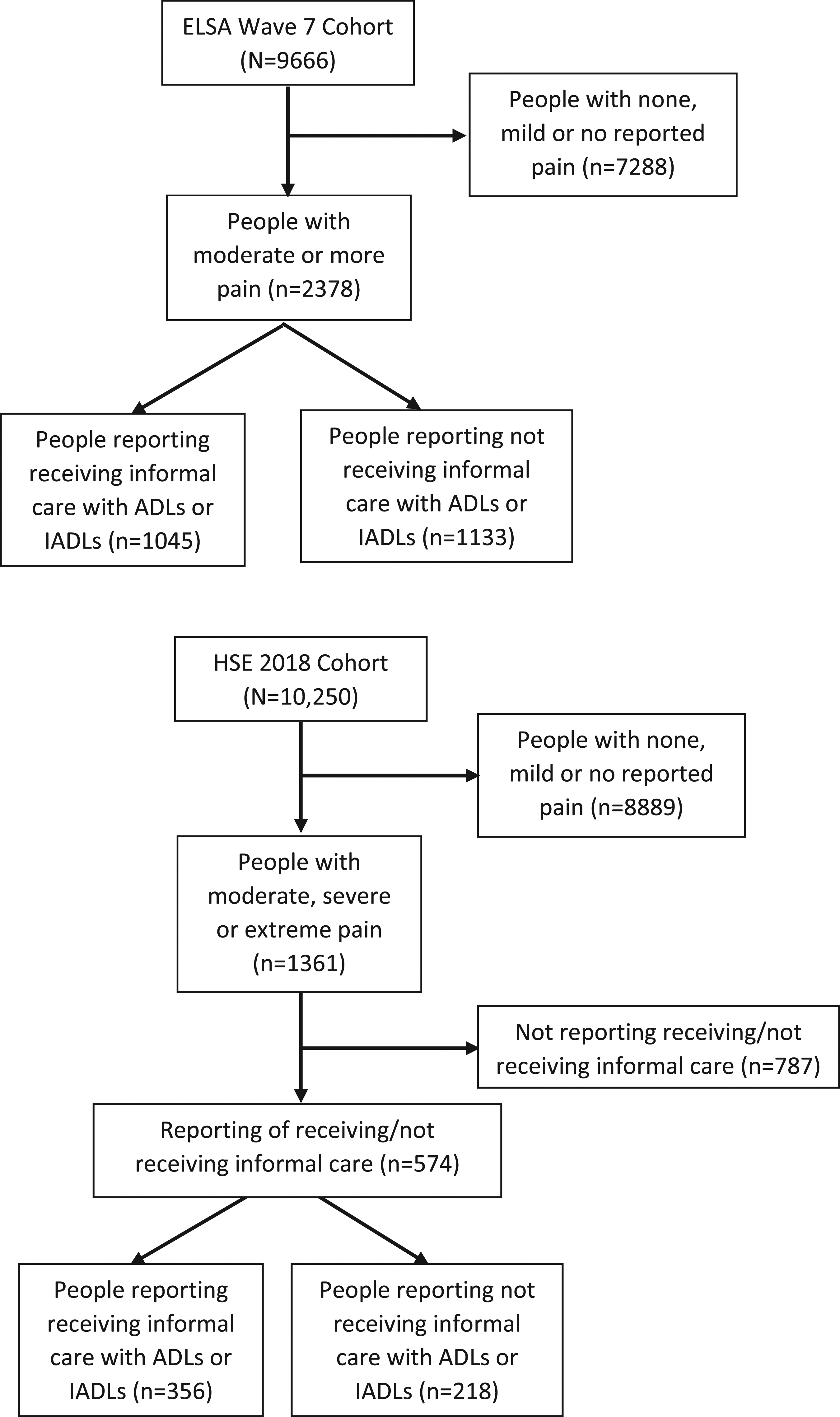
Wave 7 ELSA
Profile of people with chronic pain receiving informal care
Table illustrating the profile of people with moderate to severe chronic pain in the ELSA Wave 7 cohort who receive informal care.

CI – confidence intervals; LBP – low back pain; N – number of participants; OA – osteoarthritis; RA – rheumatoid arthritis; SD – standard deviation; UCLA – University of Los Angeles.
Profile of informal care provision
Table illustrating the care provision for individuals with moderate to severe pain in the ELSA Wave 7 cohort who receive informal care.

IQR - inter-quartile range; N – number of participants; SD – standard deviation.
Most frequently, informal caregivers were partners (50%), daughters (25%) or sons (19%). Nonetheless, various individuals were reported as caregivers, including friends (10%) and neighbours (4%). The median number of different caregivers’ participants reported having was one (IQR: 1–2), with 26.2% of participants reporting two or more caregivers.
Figure 2 illustrates the time provided for assistance to care recipients per week. The most frequent duration was one to 4 h per week. Partners and daughters most frequently provided the highest duration of support at 100 h or more per week. Stack bar chart of hours of informal care provided by caregiver for person with moderate to severe pain reported in the Wave 7 ELSA cohort.
Health status of people with chronic pain who receive informal care compared to those who do not
Table illustrating the comparison in clinical status characteristics between individuals with moderate to severe pain in the ELSA Wave 7 cohort who receive informal care versus do not receive informal care.
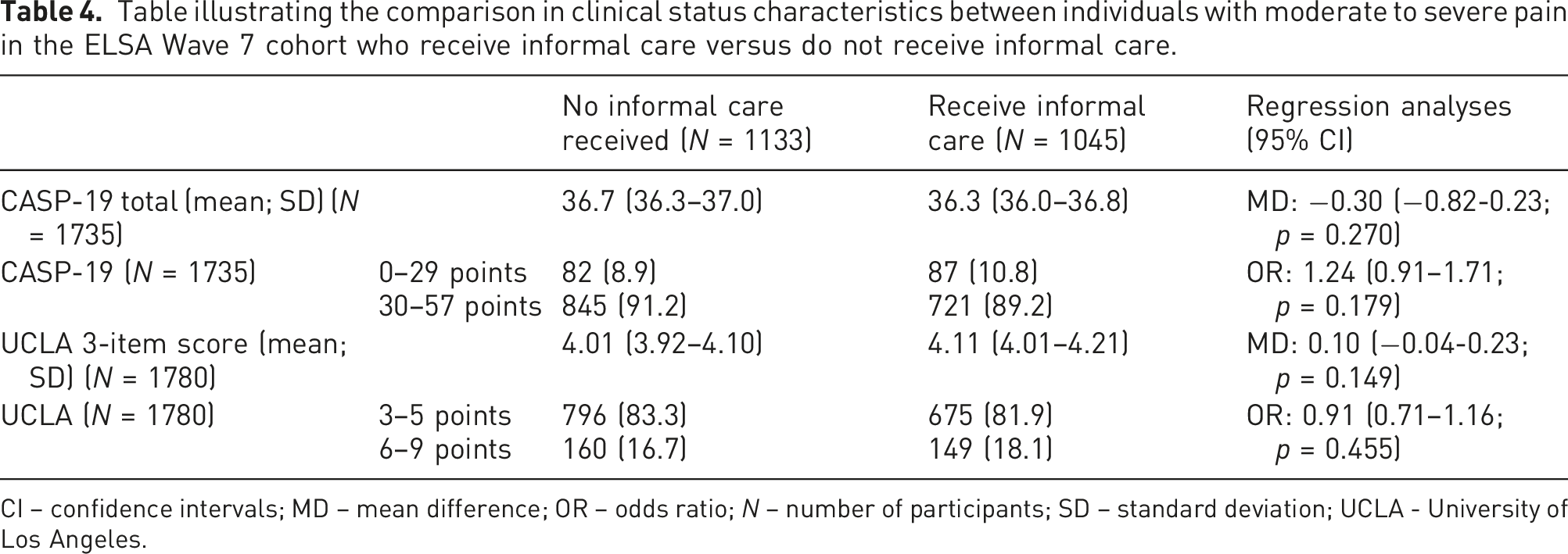
CI – confidence intervals; MD – mean difference; OR – odds ratio; N – number of participants; SD – standard deviation; UCLA - University of Los Angeles.
Health survey for England
Profile of people with chronic pain receiving informal care
Table illustrating the comparison in characteristics between individuals with moderate to severe pain in the 2018 Health Survey for England cohort who receive informal care versus do not receive informal care.
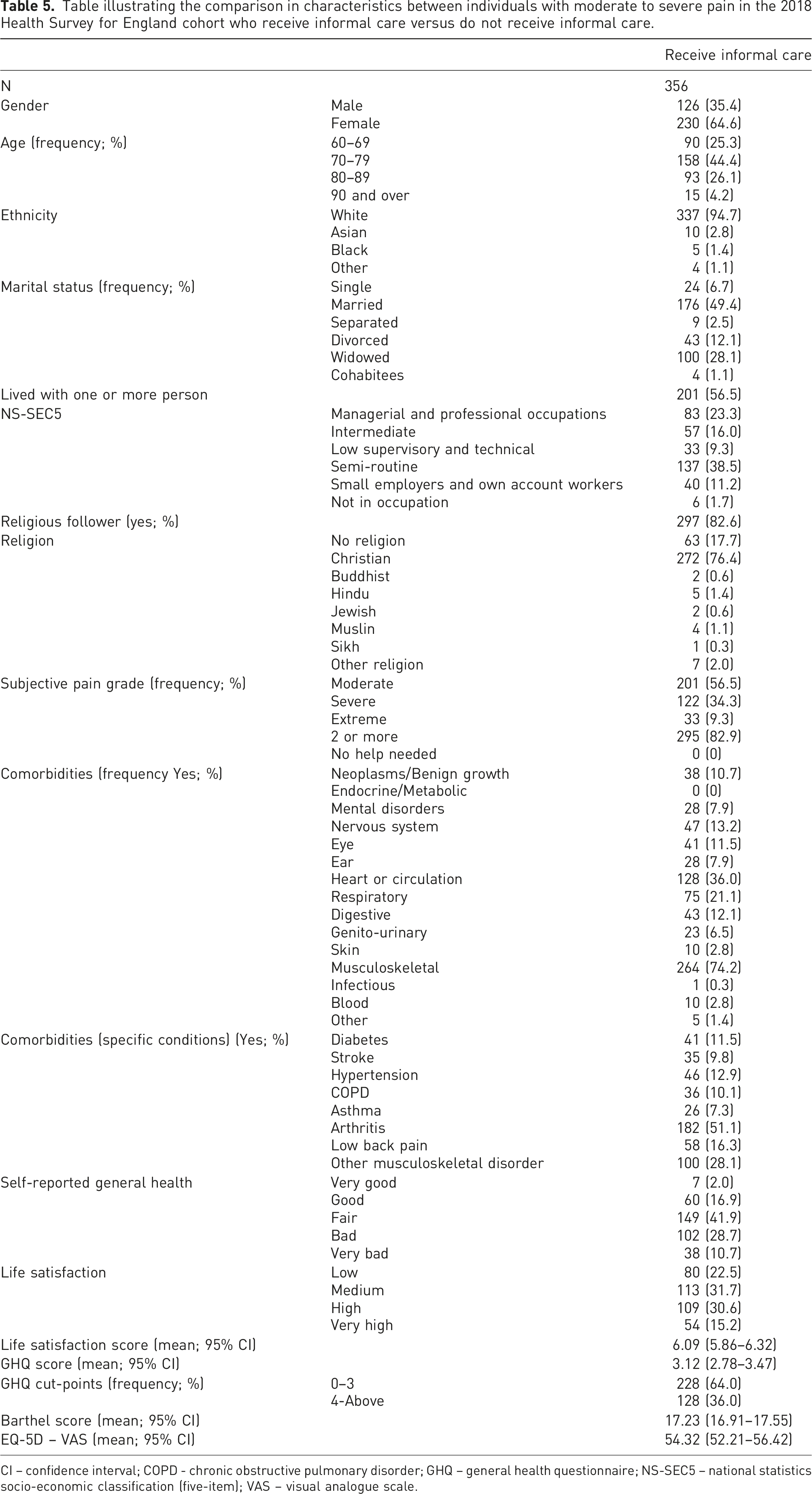
CI – confidence interval; COPD - chronic obstructive pulmonary disorder; GHQ – general health questionnaire; NS-SEC5 – national statistics socio-economic classification (five-item); VAS – visual analogue scale.
Profile of informal care provision
Table illustrating the care provision for individuals with moderate to severe pain in the 2018 Health Survey for England cohort who receive informal care.

N – number of participants.
The most frequent informal caregivers were partners (25%), daughters (24%) or sons (12%). Outside the family network, friends provided informal caregiving for eight percent of the cohort and neighbours for three percent.
Figure 3 illustrates the time provided for assistance to care recipients per week. For all providers, the most frequent duration was one to 4 hours per week. Partners provided the greatest frequency of 100 h or more support.
Health status of people with chronic pain who received informal care compared to those who do not
Table illustrating the comparison in clinical status characteristics between individuals with moderate to severe pain in the 2018 Health Survey for England cohort who receive informal care versus do not receive informal care.

CI – confidence intervals; GHQ – general health questionnaire; MD – mean difference; OR – odds ratio; VAS – visual analogue scale.

Stack bar chart of hours of informal care provided by caregiver for person with moderate to severe pain reported in the 2018 Health Survey for England cohort.
Discussion
The findings of this analysis indicate that people who receive care are frequently female, older aged with several medical morbidities including musculoskeletal diseases such as arthritis. People with self-reported moderate, severe or extreme intensities of chronic pain receive informal care for several diverse tasks. Most frequently these relate to IADLs such as shopping and housework. They are most frequently provided by a partner or their children. However, many also receive support from friends and neighbours. Although they demonstrate greater disability and symptoms, people who receive care do not demonstrate differences in health status either physically or mentally than those who do not.
The analysis of two nationally representative cohorts, as performed in this study, has been helpful in identifying similarities and discrepancies between the two datasets. For example, there appears consistency that care recipients who live with chronic pain are most frequently older people, females and frequently experience pain from musculoskeletal disorders. However, there are also inconsistencies between these two cohorts. For instance, care recipients from the ELSA cohort were more likely to report better self-reported general health, whereas this was lower for care recipients in the HSE cohort. Similarly, whilst perceived wellbeing was no different between care recipients and non-recipients in the ELSA cohort, care recipients reported lower life satisfaction, greater mental distress and poorer HRQoL compared to non-recipients in the HSE cohort. Previous literature offers similar uncertainties on the relationship between chronic pain and health outcomes. Bjornsdottir et al. 31 and Vartiainen et al. 32 reported that individuals with chronic pain had increased risk of reduced HRQoL. However there remains limited evidence to understand what the impact of receiving informal care is to mediate this.
This paper contributes to understanding on the care needs of people with chronic pain. Hermsen et al. 33 found that older adults with joint pain and comorbidities reported on average four care needs using the Camberwell Assessment Need for the Elderly (CANE) tool. They suggest that psychosocial needs were often unmet. 33 We were unable to explore psychosocial roles which informal caregivers or care recipients may have as data were not reported in this way by these datasets. Identifying the scope of unmet psychosocial care needs for both members in this dyad, with strategies to improve psychosocial wellbeing of these individuals, may be an important avenue for future study.
Usual UK care offers patient-centred interventions to support long-term management of pain and disability.10–12 These are either through structured programmes such as the ESCAPE-Pain programme 34 or non-structured programmes incorporating elements of education, exercise, pain relief and psychological interventions, as supported by NICE.10–12 However, in both instances, neither include caregiver interventions to support patients’ symptom management. Smith et al. 35 reported the outcome of caregiver interventions to support people with chronic pain. They reported moderate-quality evidence that caregiver interventions were effective in reducing pain in the short-term (effect size (ES): 0.16; 95% CI: −0.29 to −0.03) and low-quality evidence they could improve social functioning in the short (ES: 0.20; 95% CI: 0.02–0.38) and medium-term (ES: 0.35, 95% CI: 0.10–0.61). There was low-quality evidence that caregiver interventions improved patient-perceived coping in the short-term (ES: 0.81; 95% CI: 0.39–1.23). This importantly suggests that caregiver interventions, when offered, may confer benefit on the recipient of informal care. 35 The findings from this study have provided insights into the profile of people with chronic pain who need (and receive) informal care. Health professionals may therefore be cognisant of their potential role in discussing care and support needs, not only with patients but also with caregivers, who may support people living with chronic pain.
The analyses performed were based on cohorts from England. Whilst there is some diversity in the national population, there was limited diversity reported in these cohort. For instance, less than two percent of this cohort were from non-white ethnicities. This is an important consideration in relation to ethnicity, culture and beliefs when the national average of non-white people in England is 14%. 36 People with differing beliefs about pain and its management may express this symptom differently.37,38 Similarly, some cultures have contrasting views on the responsibility of family and friends to caregiving 39 and be more likely to live nearby to family members which may facilitate caregiving. 40 Such analyses to explore the relationship between cultural differences and caregiving for pain would be valuable.
The results offer important research implications. Firstly, there remains uncertainty as to what can be offered as informal care to support people living with chronic pain. The results indicate a need to better support these individuals. Currently the JOINT SUPPORT trial 41 has begun to investigate a caregiver intervention for people with chronic musculoskeletal pain. This is aimed to better understand whether a caregiver programme can modify outcomes both for individuals with pain and their caregivers. Secondly, the findings offer a ‘mixed’ interpretation on the health status of people living with chronic pain who receive or do not receive informal care. Whilst our findings indicate that those who receive informal care often have greater disability to require assistance in activities, these individuals, based on the ELSA cohort, have similar health and wellbeing outcomes to individuals who do not receive assistance. Conversely the HSE cohort suggests that those who receive informal care, with equal levels of disability, have poorer health outcomes. Interpretations can be offered for where effective informal caregiving may ‘equal out’ the perceived poorer health status, thereby providing comparable health status. The HSE cohort may be interpreted to have greater disability and pain severity reported by people receiving care, reflected in poorer health status. In that instance, the provision of informal care appears not to modify this. Given this variability in outcome, further longitudinal evaluation of diverse health and wellbeing outcomes, is warranted.
From a clinical perspective, this epidemiological study highlights that people with chronic pain frequently receive support on a wide variety of activities, at varying intensities. Whilst management programmes frequently focus on ‘patients’, clinicians should also consider those who support them. Where appropriate, educating caregivers on management skills and treatment regimens to promote patient adherence and understanding, should be considered. As highlighted, further research is being undertaken, 41 to provide an evidence-base on-which to implement such programmes.
This analysis offers several strengths. Firstly, this is the first analysis of informal care receipt for people with chronic pain. It is based on two large and representative English cohorts, thereby offering generalisable findings to this population. The interpretation of two cohorts provides the ability to assess for similarities and differences to make firmer conclusions on the research question. However, the study also presents with four weaknesses. Firstly, there were limited data to determine whether individuals who received care required this principally for chronic pain or whether this was for another condition. Whilst the comorbidity data indicates that musculoskeletal pain and disorders were the most prevalent medical presentation in both datasets, medical conditions such as respiratory, neurological, or mental health conditions may have impacted on the reasoning why people needed informal care. Secondly, it was not the purpose of this analysis to assess whether care receipt changed over time. Whilst this would be helpful to determine whether this challenge is static or progressive, the use of the latter phases of data collection waves for the respective cohorts meant a longitudinal analysis was not feasible. Thirdly, the data reported were self-reported, therefore offering potential issues in recall or social desirability bias. 42 There remains stigma regarding how people report the level of care they provide or receive. 43 Further prospective means of assessing caregiving requirements and receipt would be helpful to determine such potential biases. Finally, whilst assessments were made on socio-economic status, religion and ethnicity, there was limited data provided through the datasets on culture and attitudes to caregiving. Given these may influence the types of activities, frequency and relationship with care recipients,44,45 future assessment in indicated to consider these potentially important factors.
Conclusions
People living with chronic pain frequently receive informal care and support from an array of different people. This is a diverse level of support both in the types of tasks supported and the time commitment offered by informal caregivers. This analysis has indicated that whilst it may be possible to characterise people living with chronic pain who receive informal care, there is uncertainty on the impact of informal caregiving on their health and wellbeing. There is valuable learning to be now made on how best to support both care recipients and informal caregivers, to ensure their health and quality of life is promoted whilst living with this long-term condition.
Footnotes
Contributorship
All authors contributed to the design, conduct, analysis and preparation of the drafts of this paper. TS and AC lead the analysis. All authors approve the final version of the paper.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
ELSA Wave 7: South Central – Berkshire Research Ethics Committee on 23rd September 2015 (Reference: 15/SC/0526). HSE2019-HSE2019: East Midlands Nottingham 2 Research Ethics Committee in 2015 (Reference no. 15/EM/0254).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Received as part of the REC approval.
Guarantor
TS. The corresponding author will act as guarantor. They had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Data availability statement
All data are under the supervision of the corresponding author and can be made available on reasonable request.