
Abstract
Background
Demand on emergency departments (EDs) is rising, at least in part due to patients with conditions suitable for management in primary care. Pain experienced in the back region is a common reason for patients to seek help and much of the established literature on back pain suggests serious pathologies are rare and the majority of patients can be safely treated in primary care. Emerging international data suggests that patients who present to ED complaining of back pain do not reflect those in primary care, with a higher rate of serious pathologies and non-spinal causes. This exploratory study seeks to quantify the prevalence of people attending ED with back pain, to describe their characteristics and the characteristics of their attendance.
Methods
This observational study is a retrospective analysis of patients attending EDs within an NHS Trust in the North East of England presenting with back pain from 1/10/2017 to 30/09/2018.
Results
Of 212,020 attendances, 3872 (2%) patients presented complaining of back pain on arrival. 36% of patients had no official diagnosis recorded, 5% were categorised as having a potentially serious spinal pathology, 22% had a non-spinal pathology diagnosis and 23% were categorised as simple backache. The majority (56%) had no recorded investigations, 19% received plain radiography, 5% received either CT/MRI, 18% had blood investigations and 17% had cardiac monitoring or electrocardiogram. Most individuals self-presented. NHS 111, primary care and community care referrals accounted for 24% of attendances.
Conclusion
Back pain was a relatively common ED attendance and represented a variety of conditions including non-spinal causes. This suggests that the population of patients with back pain attending ED are a different subgroup to those presenting to primary care. Care should be taken applying primary care guidance to this group and there may be a need for emergency care specific back pain guidelines.
Introduction
Increasing pressure on emergency departments (ED) is an international phenomenon. There is increased interest in identifying patients and conditions that can be appropriately managed in primary care and either co-locate primary care services alongside EDs or redirect users to their own primary care provider.1,2 Pain experienced in the back has been identified as one such condition and is recognised as a reason for people to present.3,4 Primary care guidelines for the management of back pain exist;5,6 they focus on reducing referral to specialist services based upon epidemiology suggesting that many patients with back pain do not have a serious or life-threatening pathology.7–9 It is commonly reported that 85%–95% of patients presenting with low back pain have non-specific lower back pain and less than 1% have a serious specific spinal pathology. 10
It has been suggested that the usual care provided in ED for patients complaining of back pain is of low value. 11 Primary care guidelines have been trialled in ED, and initial reports have been positive.12–14 As a comparison, headache is also a common presentation in ED that is frequently suitable for primary care management. The Royal College of Emergency Medicine have specific guidelines for headache 15 and similar specific guidelines might be suitable for back pain. There is emerging evidence that the population with back pain presenting to ED is different to those presenting to primary care and consequently guidelines drawn from other settings might not be suitable for ED.12,16 Patients presenting to ED with back pain may have higher levels of serious spinal pathology, but of equal importance, they may also have higher prevalence of a pathology manifesting as back pain arising from somewhere other than the spine, a category that is rarely discussed within the back pain literature. This work has been conducted outside of the UK.12,16
Very little is known about the use of ED by patients with back pain as such it is very difficult to plan the delivery and management of services. There is no recent UK data on the use of ED by patients with back pain. In a recent systematic review 13 the only UK study was from 2000. 17 A recent study of a UK Ambulance Service in the North East of England 18 found almost half of callers presenting with low back pain were later categorised with a problem elsewhere. Twelve percent were referred to primary care; nearly 70% were transported to an ED. These findings suggest that a relatively large number of patients presenting with back pain are presenting to ED and further exploration of ED use by people with back pain is warranted.
This retrospective observational study analysed attendance at ED with back pain within an NHS Trust in the North East of England. The aim was to quantify the prevalence of people attending ED with back pain, to describe the characteristics of those people and the characteristics of their attendance.
Methods
This study analysed data provided by a single NHS trust in the North East of England drawn from the electronic records of two EDs run by the Trust between 1/10/2017 and 30/09/2018. The data set included chief complaint, diagnosis, age, sex, source of attendance, primary and secondary investigations, primary and secondary treatments, and discharge destination. Data was extracted by a member of the trust staff and patient identifiable data was removed prior to it being received by the research team. The records of all patients who presented with a chief complaint related to back pain were included. The categories included ‘injury of cervical region of back’ to allow for variations in patients’ descriptions. The study received ethical approval from the Health Research Agency (REC ref: 18/SC/0278).
The dataset requested was intended to allow description of demographic characteristics and categorisation of patients’ final diagnosis for comparison to existing literature. The level of imaging used in EDs has been criticised as high compared to evidenced-based guidelines.11,19 The dataset included details of investigations including imaging as well as blood tests and cardiac monitoring that could suggest clinicians were exploring the possibility of other serious pathologies. Sources of attendance could provide data useful for identifying if strategies targeting other healthcare providers could be successful in reducing primary care appropriate attendances. It was expected that not all patients would receive a diagnosis in the ED, discharge destination provides a proxy measure for the seriousness that the attending clinician attached to the case, for example discharge to a ward for further investigations or discharge to home.
In mid-2018, the Trust served a population of 633,546. 20 Publicly available data reported 212,020 attendances at type 1 (major accident and emergency) and type 3 (other accident and emergency/minor injury unit) departments during the study period. 21 It should be noted that the regional major trauma centres are not run by this trust and so patients suffering major spinal trauma in the trust area will not appear in this study.
Age and sex data was described and compared against other published data. Diagnoses were categorised by two of the research team (CR [physiotherapist] and MC [paramedic]) into one of five categories based on Waddell’s 7 four categories plus ‘other’: non-spinal pathology; possible serious spinal pathology (including spinal cord or cauda equina lesion); nerve root problem; simple backache and other (these records were not related to a clinical diagnosis). Investigations were analysed to identify any patterns in imaging, blood tests, urinalysis and electrocardiogram (ECG). Data on treatment recorded were expected to be used to look at analgesia; however, it was determined that there was insufficient information for meaningful analysis. Cardiac monitoring was recorded as a treatment but was included in the analysis as an investigation.
Discharge destination was explored comparing rates of those discharged home and those transferred to another department. Discharged home implied no acute care was required and included residential homes, nursing homes, prisons and police custody.
Results
There were 3872 attendances with a chief complaint of either backache (n = 1923, 49.7%), lower back injury (n = 1645, 42.5%), upper back injury (n = 277, 7.2%) or injury of cervical region of back (n = 27, 0.7%). A broad definition of back pain, including cervical pain, was used to allow for patients’ descriptions of their pain experience. Back pain attendances were 1.8% of total ED attendances.
Figure 1 summarises the demographic data of patients. Median age for all patients was 46 (IQR 30–62) [males 45 (IQR 31–61), females 46 (IQR 30–64)]. Patients were mostly female (female, n = 2141, 55%). Age and sex distribution of back pain attendances at ED. Figure 1 shows the age and sex distribution for adult patients (over the age of 16) who attended an Emergency Department run by CDDFT between 01/10/2017 and 30/09/2018. In the dataset, one patient did not have gender recorded and so was excluded from these figures. ED: emergency departments.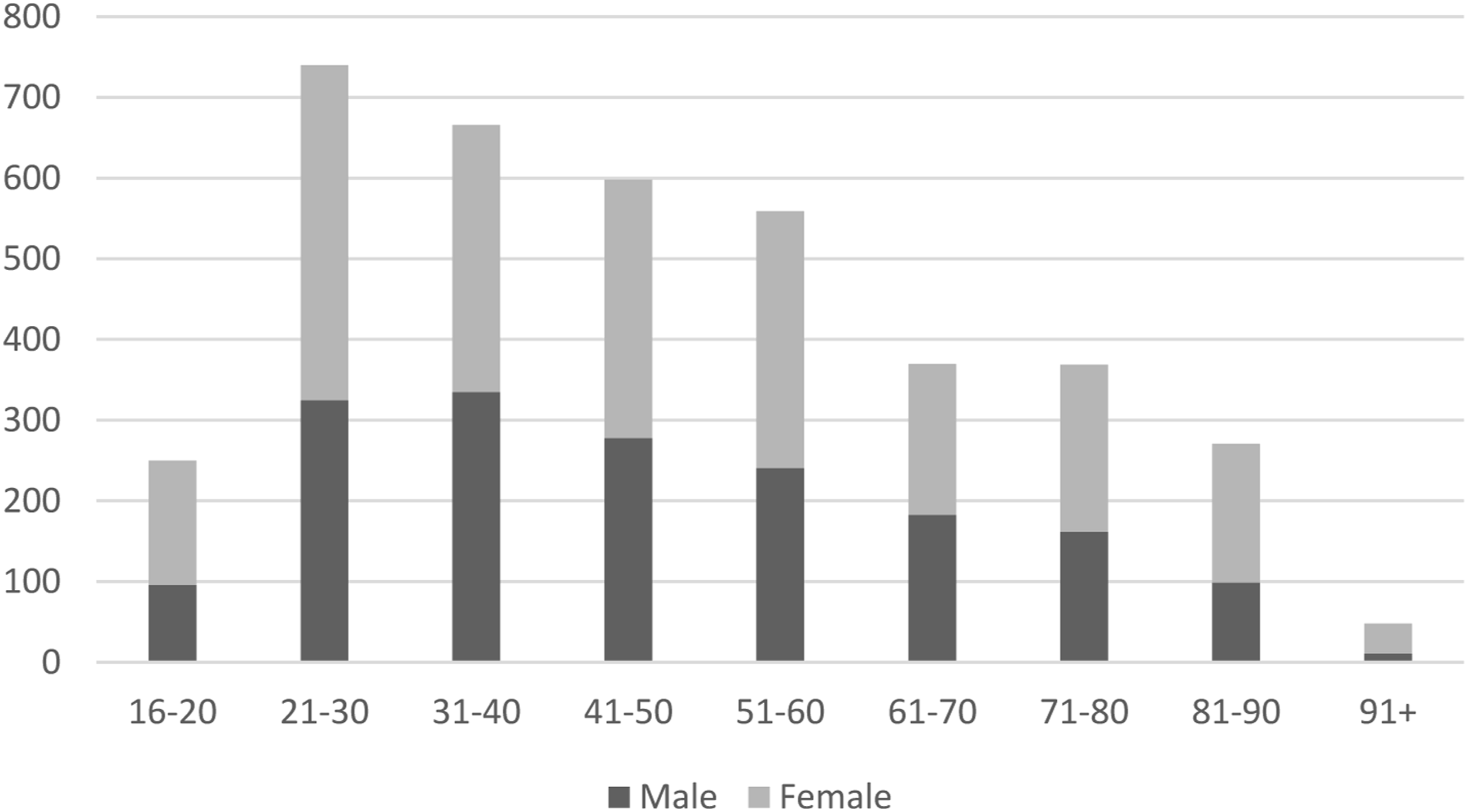
Categorisation of recorded diagnoses.
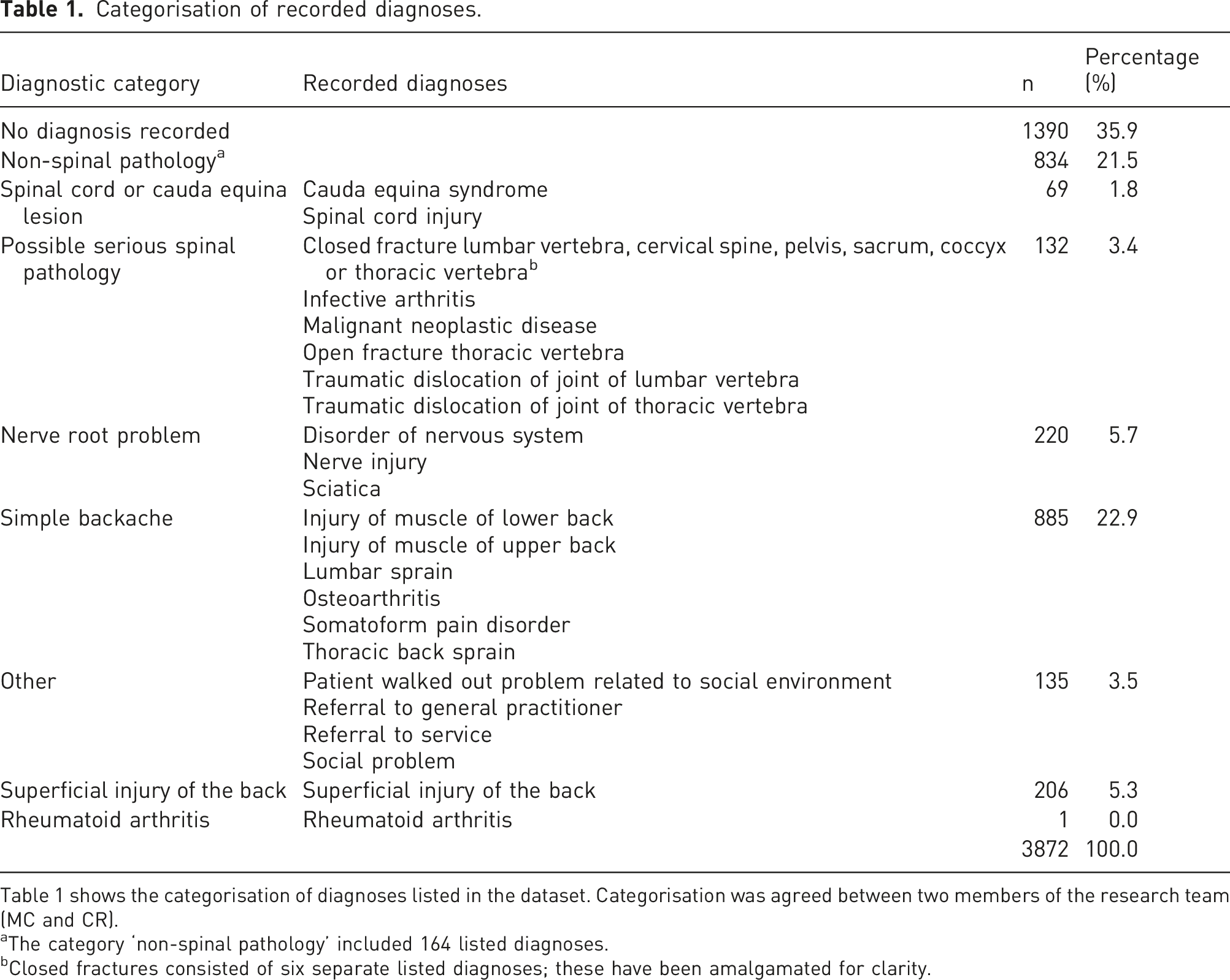
Table 1 shows the categorisation of diagnoses listed in the dataset. Categorisation was agreed between two members of the research team (MC and CR).
aThe category ‘non-spinal pathology’ included 164 listed diagnoses.
bClosed fractures consisted of six separate listed diagnoses; these have been amalgamated for clarity.
Investigations.
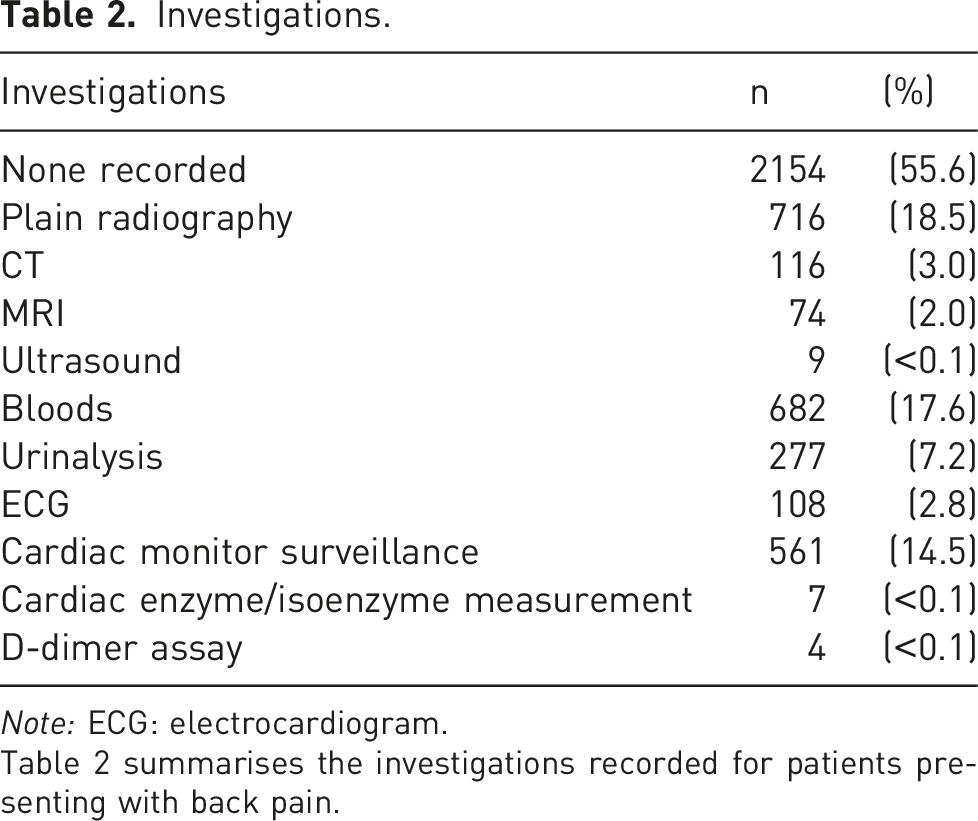
Note: ECG: electrocardiogram.
Table 2 summarises the investigations recorded for patients presenting with back pain.
Source of referral.
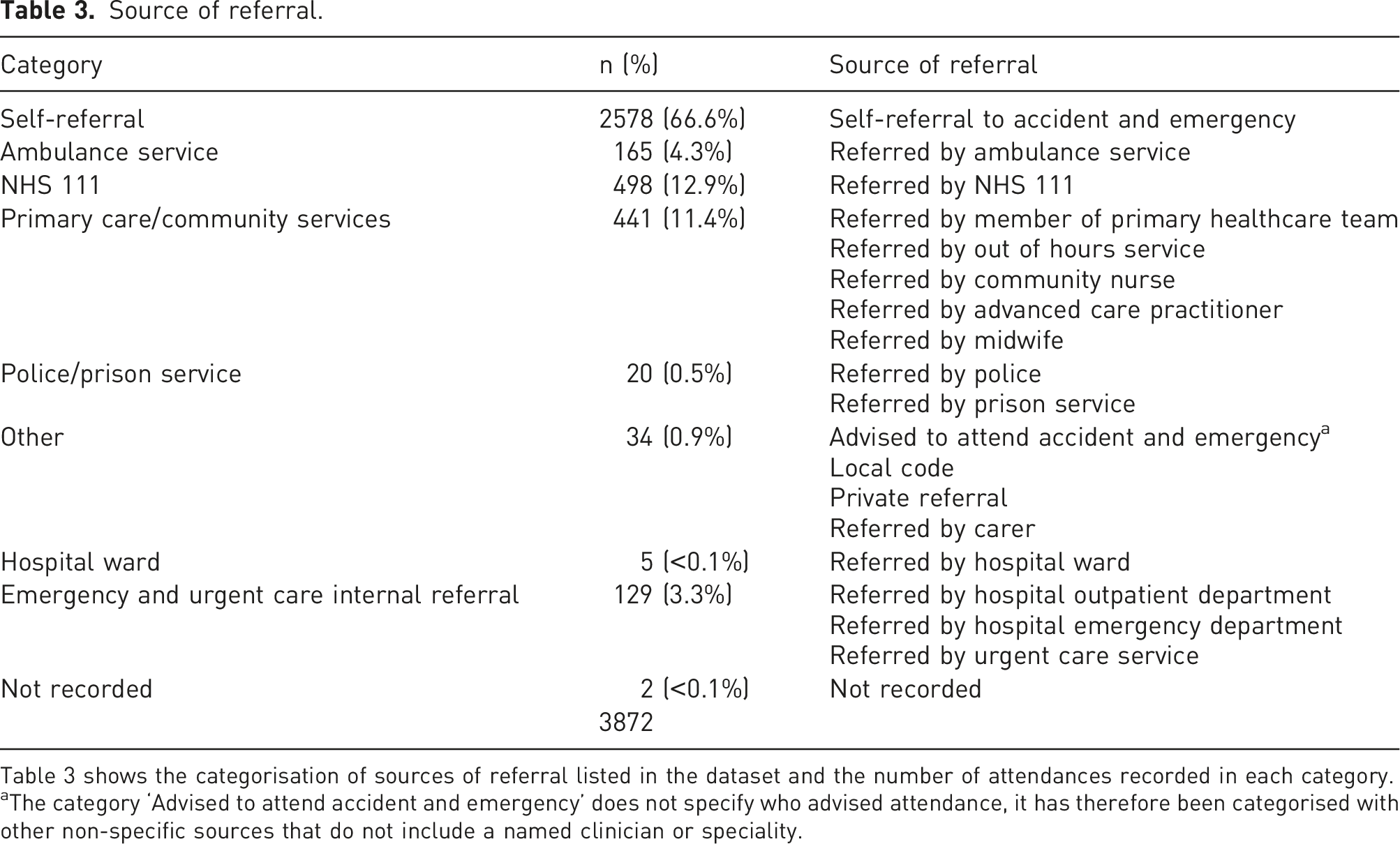
Table 3 shows the categorisation of sources of referral listed in the dataset and the number of attendances recorded in each category.
aThe category ‘Advised to attend accident and emergency’ does not specify who advised attendance, it has therefore been categorised with other non-specific sources that do not include a named clinician or speciality.
Discussion
The aim of this study was to explore emergency department use by people presenting with back pain as their chief complaint. Over 12 months, there were 3872 attendances with back pain accounting for 1.8% of total attendances. One previous UK study 17 looking at back pain at two hospitals over a period of 4 weeks reported prevalence rates in ED of 3.2% and 4.7%., roughly double the rate in our study. It is difficult to draw comparisons as that work was published 20 years ago. The reduced rate in the current study could represent better primary care services or a rise in attendances for back pain may have been eclipsed by an even larger rise in all cause ED attendances. A recent systematic review estimated International attendance rates ranging from 3.7% to 5.2%. 13 However, the heterogeneity of case definitions used internationally limits direct comparison. A recent Canadian study 4 used a similar definition to this study and reported back pain attendances accounted for 3.2% of total attendance. An Australian study, using a similar definition reported an attendance rate of 1.9%. 3 Our prevalence rate is at the lower end by international standards. Comparing figures internationally has the added challenge of differences in health service organisation. Only 165 patients (4.3%) were referred by the ambulance service in our study however a recent study in Australia 16 reported that 35.6% of patients with back pain arrived by ambulance. This notable difference may relate to differences in geography, the organisation of receiving hospitals, more referral opportunities for UK ambulance services or the hospitals in this study may not be representative.
Ages were consistent with other recent international studies conducted in ED4,16 with a median age of 46 (IQR: 30–62). The highest number of callers were in the 21–30 age group (n = 740) with numbers dropping as age increased. This contrasts notably with global back pain prevalence data 8 which peaks amongst 40–80 year olds. It is not clear why presentations are highest for younger age groups however it may reflect the inclusion of all back pain presentations rather than low back pain diagnoses, younger patients using ED rather than their General Practitioner (GP) or older patients being more stoic and either not accessing health care or preferring to use their GP. Sex distribution mirrors Edwards et al. 4 and Shaw et al. 16 with female attendances outnumbering male for all age groups (n = 2141; 55.3%).
It is frequently stated that the majority of low back pain cases, 85%–95%, are non-specific.8,19 However, these figures are beginning to be challenged in emergency care.4,16 Whilst broader inclusion criteria than low back pain were used, this study supports previous findings that the population presenting to ED with back pain is different to those presenting to other settings. Patients categorised without potentially serious pathology (simple backache, superficial injury of the back and no diagnosis recorded) was 64.1% (n = 2481). This is similar to the figure of 60.8% for ‘non-specific/mechanical low back pain no potential nerve root’ reported in Canada, 4 higher than the figure of 43.8% for ‘muscular problem or non-specific back pain’ found in Australia 3 but much lower than the aforementioned commonly cited figure of 85%–95%. Possible serious spinal pathology represented 3.4% of presentations (n = 132) and nerve root problem 5.7% (n = 220). These rates are a little higher than reported in the wider back pain literature 19 but the difference is relatively small. Of particular note is the category of non-spinal pathology. In this study 21.5% (n = 834) of patients presenting to ED with back pain received this diagnosis. Recent work has looked at widening back pain red flags to identify serious non-spinal pathology. 16 It is in this category that there would appear to be a marked difference between ED and primary care presentations and as such, bespoke guidelines for ED services may be warranted. This is particularly important given that existing key back pain guidelines, such as those by NICE, 6 make no reference to the emergency setting.
It has been suggested that many investigations performed in ED are of low value to back pain, especially imaging.11,22 This assertion has been challenged 23 and if back pain presentations in the ED involve higher rates of serious spinal pathology and non-spinal pathology then investigations may be more justified. Lovegrove et al. 3 identified renal colic and urinary tract infection or pyelonephritis as common non-spinal diagnoses for back pain in the ED. They also noted back pain as the presenting symptom for a small number of cases of angina, myocardial infarction and pulmonary emboli. As such urinalysis, ECG and blood analysis may be warranted. Of those patients presenting with back pain 2154 (55.6%) had no investigations recorded. This compares to 54.8% who did not receive investigations in the study by Shaw et al. 16 Recent studies have demonstrated different levels of imaging for patients with back pain in ED. McCaughey et al. 24 reported that imaging was requested in 30% of cases, Shaw et al. 16 reported 19% of patients received X-ray of the lumbar spine and 10% X-ray elsewhere. Plain radiography was the most common investigation in our study (n = 716; 19%). For other investigations, Shaw et al. 16 is the only study that has published figures for comparison. They reported higher rates of blood analysis (35%) and urinalysis (30%); lower rates of cardiac investigations (10%), CT (2%) and MRI (2%); ultrasound use (0.3%) was comparable with our data. Without detailed patient notes it was not possible to assess the appropriateness of investigations for patients presenting to ED complaining of back pain, however, rates of imaging in our study are similar to comparable international studies. Investigations likely to identify non-spinal pathologies are commonly used and may be justified considering the potential for serious non-spinal pathologies.
Self-referral was the most common source of attendances with back pain (n = 2578; 67%) followed by NHS 111 (n = 498; 13%) and primary care/community services (n = 441; 11%). Ambulance referrals were much lower (n = 165; 4%) however as has been noted that the regional major trauma centre and spinal injuries unit are located elsewhere. Capsey et al 18 identified in their study of an Ambulance Trust 2297 patients transported to ED by ambulance in a similar period, when adjusted for population served the expected number of ambulance referrals would be 550. This suggests that ambulance referrals to the units studied may not be representative. By comparison, Shaw et al. 16 reported 36% of the patients with back pain in their study arrived by ambulance. The relatively high referral rate from primary care/community services and NHS 111 may represent the difficulty in confidently diagnosing back pain especially if it is arising from a non-spinal cause. Penson et al. 25 explored the reasons why patients with conditions that could be managed in other settings attend ED, they identified being advised to attend by another healthcare professional as the most frequent reason. The low number of referrals from the ambulance service are hard to interpret. They could be effectively discharging patients on scene, however there are regional major trauma centres and spinal units at hospitals within 20 miles of the two EDs in this study and this must be considered a limitation to the present study. Capsey et al. 18 suggested that ambulance services transport patients with back pain at a similar rate to other conditions. The figures in the current study may underestimate the true rate of referral via ambulance of patients with back pain in the area served by the two EDs.
Most patients were discharged home (n = 3216; 83%) following assessment and treatment. In contrast Shaw et al. 16 reported only 58% were discharged to their usual place of residence. This would suggest lower numbers of immediately life-threatening diagnoses in our study, however of the 132 patients categorised as having a potential serious spinal condition 73 (55.3%) were discharged to a home setting. Without access to patient records it is not appropriate to comment on these decisions as there is no information on whether they were referred to their GP or an outpatient service.
This study provides insight into the extent and nature of ED use by patients which may be of use to help plan the delivery of services. However, there are a number of limitations to this exploratory study. It was a retrospective review of data taken from two EDs’ electronic records and so terms and categories were designed for clinical rather than research purposes. Whilst the focus of the study was back pain, 27 patients initially categorised in the clinical datasets as having ‘an injury of the cervical region’ where included. Without access to patients’ full notes it was not possible to clarify the cause of gaps in the data or to confirm final diagnoses. It was also not possible to identify if any patients attended multiple times. It would have been informative to separate non-spinal pathologies into serious and non-serious. Only primary and secondary investigations were recorded and it is not possible to say if other investigations were undertaken. With only two EDs in the North East of England included, these findings may not be generalisable. The comparatively low number of referrals from the ambulance service suggest the EDs investigated may not be representative. The lack of specialist major trauma or cardiac services in the included hospitals also limits the generalisability to hospitals with those facilities.
In conclusion, the use of ED by patients with back pain is poorly understood. Most research has focused on low back pain in the context of reducing investigations and treatment that has been shown to be of low value. However, the population presenting to ED appears to be different to that reported in the majority of existing back pain literature. Whilst non-specific low back pain still appears to be the most common diagnosis, serious spinal pathology is present at slightly higher rates compared to what is documented in primary care settings. Non-spinal pathologies appear to be markedly more prevalent in the ED setting. Other potentially primary care appropriate conditions have ED specific guidelines. 15 The differences identified suggest bespoke guidelines for back pain in emergency care are needed, or existing guidelines, such as those provided by NICE, 6 need to include consideration of the emergency setting.
Supplemental Material
Supplemental Material - Emergency department use by people with back pain: An investigation
Supplemental Material for Emergency department use by people with back pain: An investigation by Matt Capsey, Cormac Ryan, Jagjit Mankelow, Jenny Alexanders and Denis Martin in British Journal of Pain
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Contributorship
MC wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Ethical approval
Ethical approval to report these cases was obtained from the Health Research Agency, South Central – Hampshire A Research Ethics Committee (REC ref: 18/SC/0278)
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
MC.
Informed consent
Written informed consent was obtained from a legally authorised representative before the study.
Trial registration
The protocol was registered with Clinicaltrials.gov (ID: NCT03762174)
Data availability
All data generated or analysed during this study are included in this published article (and its supplementary information files).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.