
Abstract
Background:
Caregiver hesitancy for their children to receive the COVID-19 vaccine remains due to concerns regarding safety and efficacy, but also due to fear of vaccine administration-related pain and distress. Study objectives were to determine caregivers’ perceptions regarding both their personal and child’s COVID-19 vaccine administration-related stress and fear and relate this to their likelihood to allow their child to receive COVID-19 vaccinations.
Methods:
This study was a secondary data analysis of a multicentre, cross-sectional survey of caregivers presenting to four Canadian pediatric emergency departments. Caregivers were surveyed between December 2020 and March 2021 and completed a digital survey on their own smartphones.
Results:
331 caregivers responded to the survey (mean age 39.9 years [SD 7.71]); 74.2% (245/331) were mothers. Children’s mean age was 8.8 years [SD 5.4]; 49.8% (165/331) were female. 64.1% (209/326) of caregivers were willing to vaccinate their child against COVID-19, while 35.9% (117/326) were not. Greater perceived COVID-19 vaccine administration-related pain (0.88 [0.80; 0.95], p = .003) and stress (0.82 [0.76; 0.89], p = <.001) for their child as well as greater perceived personal stress with their own COVID-19 vaccine administration (0.81 [0.75; 0.88], p = <.001) were associated with caregivers being less likely to vaccinate their child.
Conclusions:
During the time period between COVID-19 pandemic waves 2 and 3, and after the vaccine had been federally approved for adults, one-third of Canadian caregivers surveyed reported being unwilling to vaccinate their child against COVID-19 in the future. Managing children’s and caregivers’ vaccine administration-related fear and stress may improve vaccine uptake for children.
Introduction
Despite approval of the COVID-19 vaccine for children aged 5–17 years,1,2 and its recognized safety by international health organizations,3,4 vaccine hesitancy remains significant during the COVID-19 pandemic.5–7 Parents and other primary caregivers (referred to as ‘caregivers’ henceforth) often decide whether or not their child receives a vaccine, which means caregivers’ decisions can impact their child’s health. 8 Vaccine hesitancy is complex, and caregivers’ decisions to vaccinate themselves and their children include many psychological and societal factors, such as complacency, confidence, and convenience.9–12 Safety and efficacy concerns around risk of harm in the face of rapid development of the COVID-19 vaccine may further add to hesitancy. 13
Fear of needles is common, estimated to affect one quarter of caregivers, almost two-thirds of children and up to half of youth14–16 and may contribute to COVID-19 vaccine hesitancy. 14 While most vaccine-hesitant caregivers are concerned about COVID-19 vaccines’ efficacy and safety, 17 8% of Canadian caregivers state needle fear is the primary reason for overall immunization non-compliance, 16 while 5–7% of caregivers in a recent small Canadian survey mentioned needle fear as a contributing factor to their COVID-19 vaccine hesitancy. 14
By surveying caregivers across four Canadian centres seeking medical care during the COVID-19 pandemic, this study seeks to provide a broader, realistic, and timely understanding of caregivers’ vaccine hesitancy about COVID-19 vaccines. Previous studies have explored caregivers’ vaccine hesitancy; however, to our knowledge, no study has specifically examined caregiver perspectives on COVID-19 vaccine administration-related pain and stress in a multicentre context. We aimed to determine caregivers’ perceptions regarding both their personal and child’s: (a) stress and fear of needle pain related to vaccination and (b) relate this to their likelihood to choose for their child to receive COVID-19 vaccinations.
Patients and Methods
Study Design and Setting
This study was a secondary data analysis of a multicentre, cross-sectional survey of caregivers presenting to four pediatric Emergency Departments (EDs) in Canada (BC Children’s Hospital, Vancouver, BC; Stollery Children’s Hospital, Edmonton, AB; Alberta Children’s Hospital, Calgary, AB; Jim Pattison Children’s Hospital, Saskatoon, SK). Ethics approval was obtained from each participating site’s local Research Ethics Board.
Survey Design
This study is part of a larger COVID-19 Parental Attitude Study (COVIPAS) collaborative of caregivers presenting for emergency care for their children during the era of COVID-19 (See Appendix 1). Modified Burns methodology was utilized for survey development. 18 The study-specific items were developed by the COVIPAS research team.17,19–21 Data collection for this phase of the study took place between December 2020 to March 2021, the time period between COVID-19 pandemic waves 2 and 3 in Canada, after the vaccine had been federally approved for adults, but before COVID-19 vaccine approval for children of any age.1,22
Participants and Recruitment
Using posters placed in waiting areas and patient rooms, as well as direct approach by healthcare team members or research staff, caregivers who arrived to EDs were asked to take part in the survey. For infection control purposes, interested caregivers used their own smartphones to complete the survey by logging into a secure online platform based on REDCap metadata-driven software (Vanderbilt University). Consent was implied once the participant selected their study site within the electronic survey.
Study Outcomes and Measurements
The primary outcomes for this study were caregivers’ personal ratings of their own COVID-19 vaccine administration-related stress and pain as well as that associated with their child receiving the same vaccine. Pain and stress were measured using an 11-point numerical scale (ranging from 0 = no pain/no stress to 10 = the most pain/stress imaginable).
Study Tool
The survey included demographic questions about the caregiver and child, seven questions related to the caregiver’s and child’s COVID-19 vaccine administration-related stress and pain, as well as the child’s prior immunization history. All responses to the survey questions were optional, leading to slight variability for response rates between questions. (See Supplemental material for Survey Questions)
Statistical Analysis
Descriptive statistics and frequencies were used to describe all variables, comparing survey data from caregivers who would vaccinate their children against COVID-19 and those that would not. We used univariable and multivariable logistic regression to assess the possible association between reported COVID-19 vaccine administration-related stress and pain scores for caregivers and their child and caregivers plan to have their child vaccinated. Both scores were measured on an 11-point scale and the model results are presented as odds ratios for willingness to vaccinate per one unit increase in scores with 95% confidence intervals and Wald p-values. The multivariable model included all pain and stress scores, as well as other potential confounding variables including: caregiver education level, caregiver age, whether child had chronic illness and whether childhood vaccines were delayed. All analyses were conducted with R version 3.5.1.
Results
Demographic Characteristics
A total of 331 caregivers were surveyed during the study period, with a mean caregiver age of 39.9 (Standard Deviation (SD) 7.71) years; 74.2% (245/331) were the child’s mother. Children’s mean age was 8.8 (SD 5.4) years and 49.8% (165/331) were females. (Table 1)
Demographic characteristics.
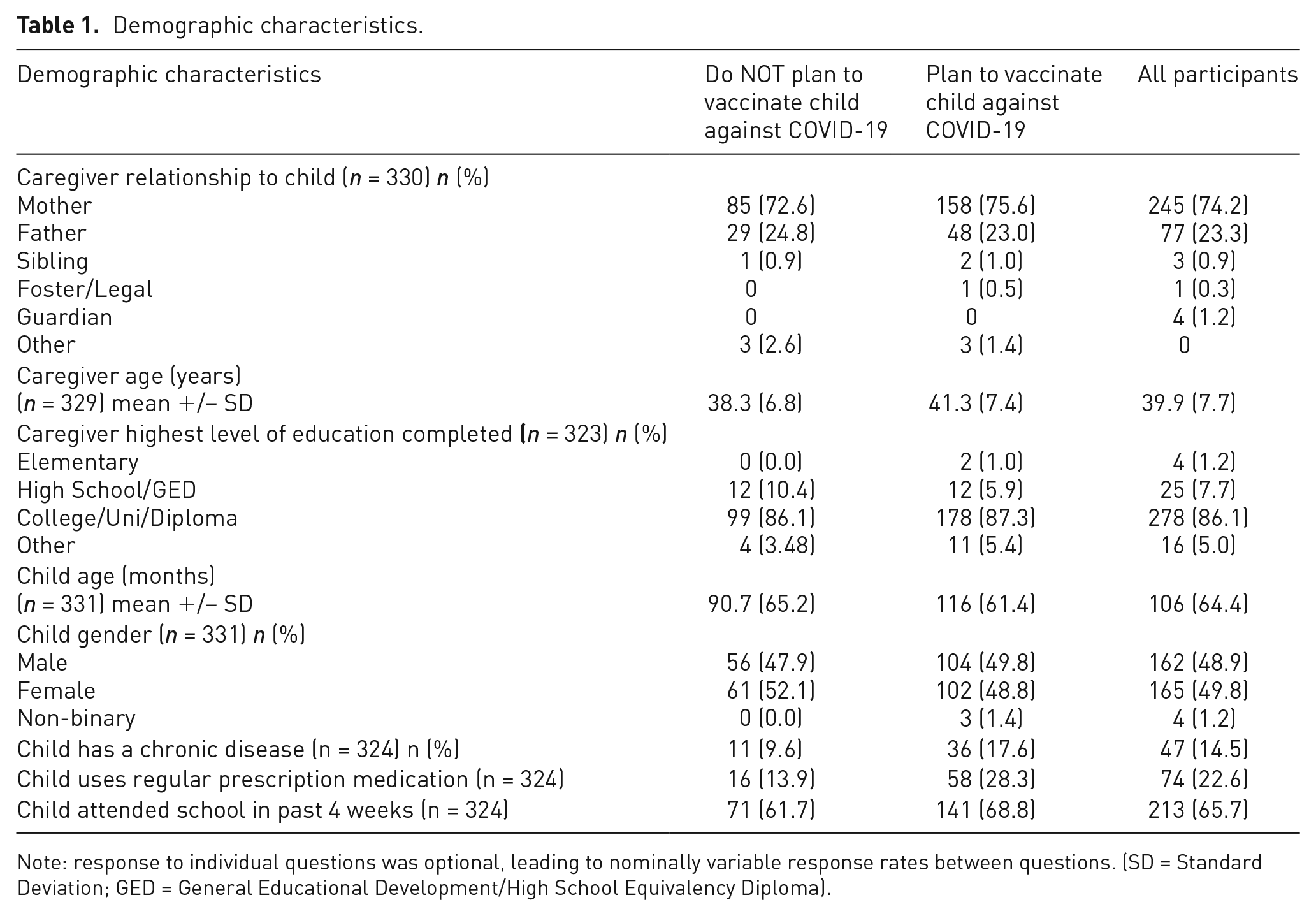
Note: response to individual questions was optional, leading to nominally variable response rates between questions. (SD = Standard Deviation; GED = General Educational Development/High School Equivalency Diploma).
Willingness to Vaccinate
The willingness for caregivers to have their child vaccinated against COVID-19 was 64.1% (209/326), while 35.9% (117/326) were not willing to vaccinate their child against COVID-19.
COVID-19 Exposure
In the previous 6 months, 47.0% (150/319) of caregivers reported that their child’s school had experienced a COVID-19 outbreak. At the time of completing the survey, 12.3% (40/324) had someone at home recently exposed to a COVID positive person. While 5.3% (17/324) of caregivers noted someone in the household being currently sick with respiratory symptoms, only 2.5% (8/323) reported a current COVID positive case in their home. A total of 4.4% (6/136) of respondents reported that their child had previously tested positive for COVID-19, while 43.0% (137/319) said their child had tested negative.
Immunization History
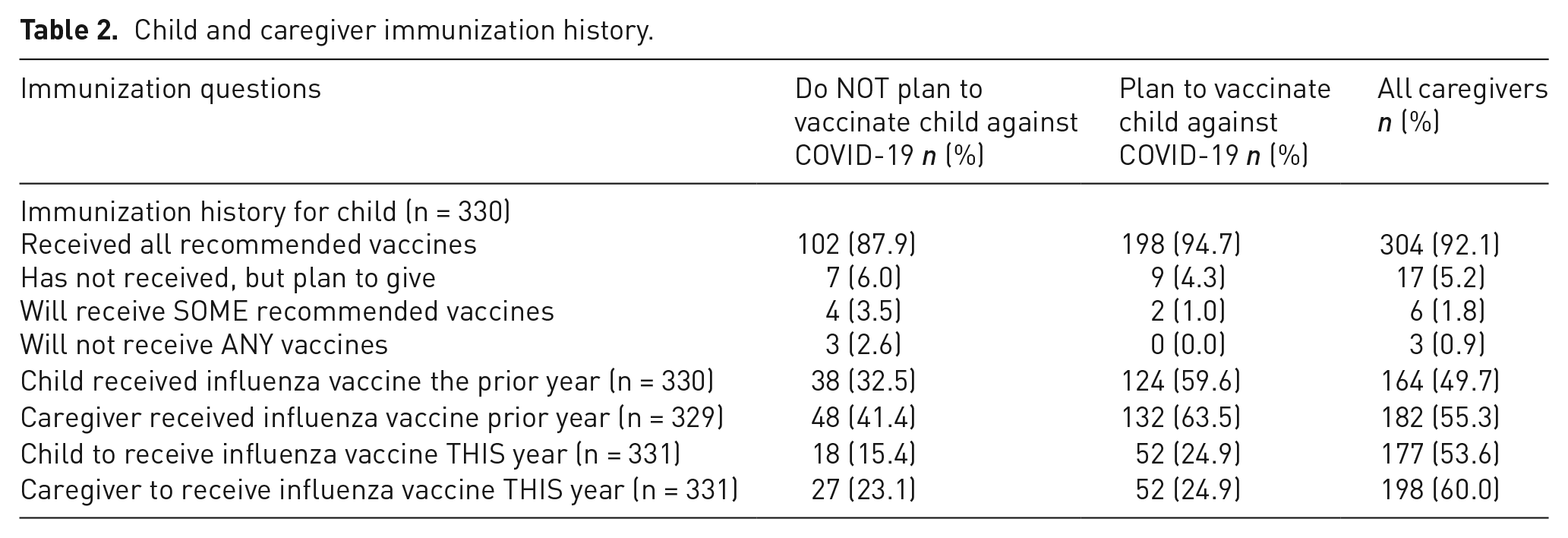
The immunization history of the respondents’ children is presented in Table 2.
Child and caregiver immunization history.
Vaccine, Pain, and Stress
Of those caregivers planning for their child to receive the COVID-19 vaccine, a total of 19.7% (41/209) noted a delay in their child receiving their recommended childhood vaccines, while 27.4% (32/117) of respondents not wanting their child to receive the COVID-19 vaccine noted a delay. Of those caregivers who planned to vaccinate their child against COVID-19, 10.0% (4/41) delayed routine vaccinations due to needle pain, 20.5% (8/41) due to a fear of needles, 27.5% (11/41) due to vaccine-related side effects, and 63.4% (26/41) for other non-specified reasons. For caregivers not planning to vaccinate their child against COVID-19, 6.3% (2/32) expected to delay due to needle pain, 3.1% (1/32) because of a fear of needles, 46.9% (15/32) due to vaccine-related side effects, and 62.5% (20/32) for other non-specified reasons.
Table 3 represents caregivers’ anticipated COVID-19 vaccination administration-related stress and pain for their child and themselves. Caregivers who planned to vaccinate their child against COVID-19 anticipated their child’s pain to be less (mean 3.4, SD 2.5) than those who did not plan to vaccinate (mean 4.3, SD 2.9). Those who planned to vaccinate their child reported less perceived stress for themselves (mean 4.0, SD 3.0) and their child (mean 1.8, SD 2.4) compared to caregivers who did not plan to vaccinate their child (mean 3.6, SD 3.4 for self; mean 5.9, SD 3.3 for child).
COVID-19 vaccine administration-related stress and pain (n = 331).
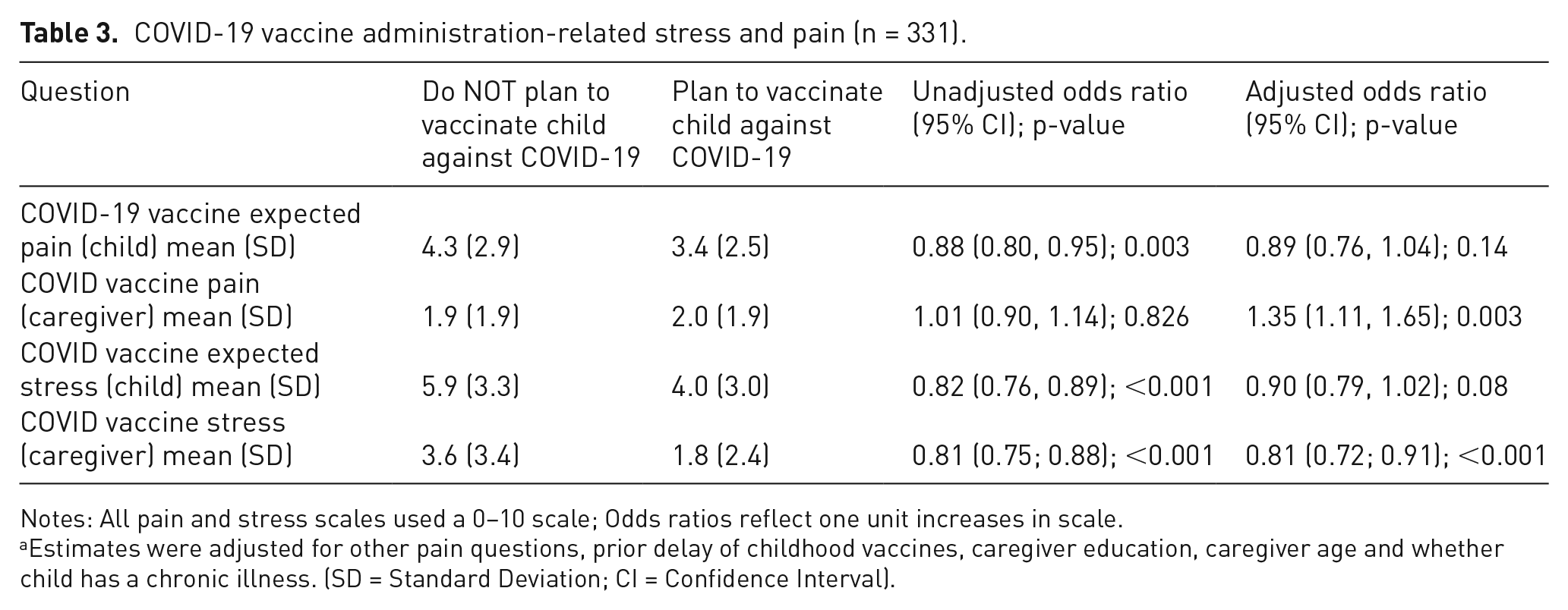
Notes: All pain and stress scales used a 0–10 scale; Odds ratios reflect one unit increases in scale.
Estimates were adjusted for other pain questions, prior delay of childhood vaccines, caregiver education, caregiver age and whether child has a chronic illness. (SD = Standard Deviation; CI = Confidence Interval).
Caregivers who anticipated more pain or stress for their child were less likely to plan to have their child vaccinated against COVID-19 than those with lower scores (OR = 0.88 (0.80, 0.95), p = .003 and OR = 0.82 (0.76, 0.89), p ⩽ .001, respectively). Results were consistent but slightly attenuated upon adjustment for other relevant factors (See Table 3). Increased parental stress with their own personal vaccine was also associated with decreased probability of vaccination for their child, in both unadjusted and adjusted analyses (OR = 0.81 95% CI = −0.75 to 0.88, p < .001). The relationship between caregivers’ own reported COVID-19 vaccine administration-related pain and plan to vaccinate their child was less clear as unadjusted analyses showed a null association, but adjustment yielded an inverse relationship (OR = 1.35, 95% CI = 1.11 to 1.65, p = .003) compared to other scores.
Regression Analyses
In multivariable analysis (Table 4), greater expected child stress with COVID-19 vaccine administration (OR 0.81; 95% CI 0.72–0.89; p = <.001) and younger caregiver age (OR 1.05; 95% CI 1.01–1.09; p = .008) were associated with lack of willingness for caregivers to have their child vaccinated against COVID-19. Caregivers of children with chronic illness were more likely to plan to vaccinate their children against COVID-19 (OR 2.44; 95% CI 1.14–5.64; p = .027).
Multivariable Analysis of Factors Associated with Caregiver Likelihood to Vaccinate their Child against COVID-19.
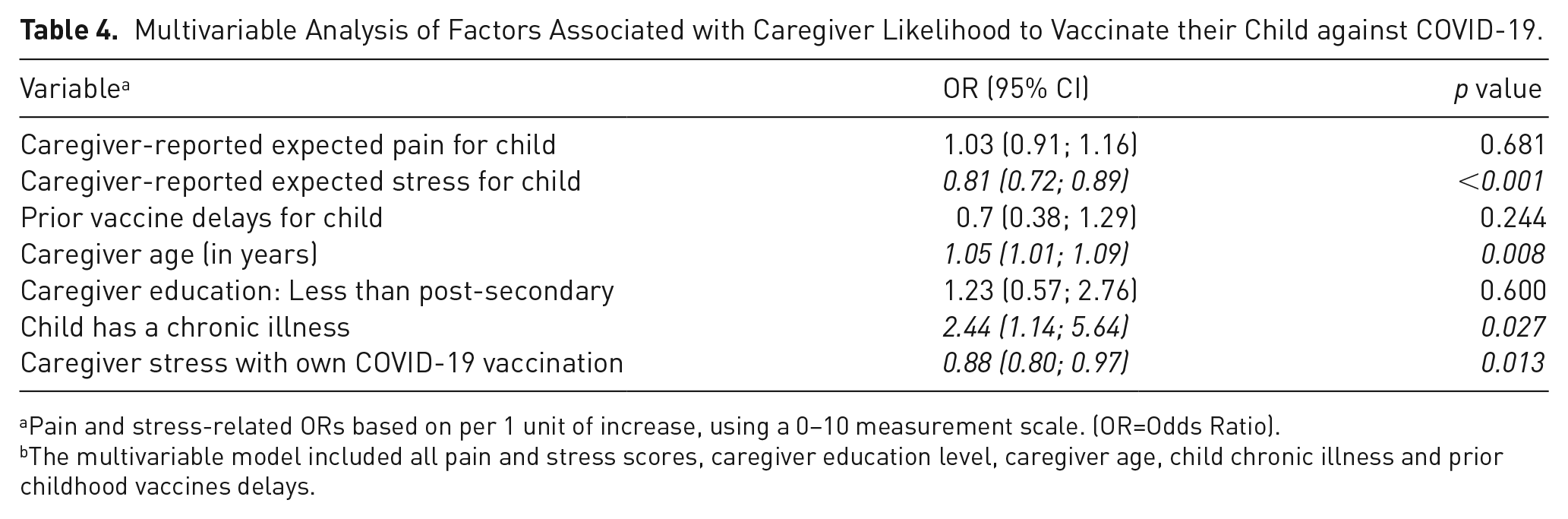
Pain and stress-related ORs based on per 1 unit of increase, using a 0–10 measurement scale. (OR=Odds Ratio).
The multivariable model included all pain and stress scores, caregiver education level, caregiver age, child chronic illness and prior childhood vaccines delays.
Discussion
We report that over one-third of caregivers in four Canadian centres did not plan to vaccinate their children against COVID-19 at the time of study. Caregivers’ expected COVID-19 vaccination-related pain and stress for their child and their personal stress from their own COVID-19 vaccination, were factors associated with a reported lack of willingness to vaccinate their children against COVID-19. Caregivers whose child had a chronic illness were more likely to plan to vaccinate their child against COVID-19.
Vaccine hesitancy is more complex than an individual either accepting or rejecting a vaccination, as it encompasses both an attitude toward vaccinations and behaviour related toward them. 11 In Canada, contributing factors to public vaccine hesitancy include misinformation being shared on the internet and through social media, a mistrust of the pharmaceutical industry, a lack of confidence in the safety or efficacy of a vaccine, and sometimes conflicting communication by different public health authorities. 11 In our study, the vast majority of caregivers who were hesitant for their child to receive the COVID-19 vaccination report being committed to vaccinating their child within the routine childhood immunization schedule. This finding is not surprising, as vaccine hesitancy is a continuum, and it is common for many vaccine-hesitant caregivers to accept some vaccines, but decline or delay others. 9 COVID-19 being a newly developed vaccine likely contributed to caregivers’ hesitancy to vaccinate their children, and may also negatively impact the perceived risk of vaccinating their child for routine childhood immunizations in the future; this may change with increasing vaccine approval in pediatric patients. 23 This lack of confidence in the safety and efficacy of the COVID-19 vaccine is likely one of the primary reasons that individuals may be hesitant to it. 11
Children’s expected COVID-19 vaccine administration-related stress and pain were factors uniformly ranked higher than caregivers’ own COVID-19 vaccine-related pain among both pediatric COVID-19 vaccine accepting and hesitant caregivers. Interestingly, child and caregiver stress had a greater impact on a caregiver’s likelihood to vaccinate their child against COVID-19 than pain. There has been increased attention to children’s experiences when receiving a vaccine. 24 While the historical focus on mitigating pain is critical and influences children’s procedural experiences significantly, direct focus on distress and fear may further improve the vaccine experience. 25 Some evidence suggests that preparation and using distraction tools can mitigate procedure-related anxiety, though more rigorous studies need to be completed in these areas. 26 The results of this study suggest that in order to help address hesitancy to children receiving the COVID-19 vaccine managing caregiver and child stress may need to be prioritized.
While not the primary focus of our study, younger caregivers were less likely to be willing to vaccinate their child against COVID-19. This is consistent with previously published literature in the context of COVID-19 vaccinations, 27 and suggests that strategies to address vaccine hesitancy should be specifically targeted to younger caregivers. The fact that caregivers of children with a chronic illness were more likely to have their child vaccinated against COVID-19 is an acknowledgement that infectious disease may pose a greater threat to their child than others’ children.
Limitations
Our study has several limitations. Due to the small sample size and inherent biases in survey design and implementation, the answers that caregivers gave cannot be considered representative of all caregivers at the study sites and may affect generalizability. Caregivers’ responses in this study about vaccine hesitancy were hypothetical at the time of the survey since the COVID-19 vaccination was not approved for use in children at the time of the study.
Conclusions
Over one-third of caregivers in Canada attending a pediatric ED during the COVID-19 pandemic were currently unwilling to vaccinate their child against COVID-19. Factors that make caregivers’ vaccine hesitancy more likely include the caregiver’s anticipated COVID-19 vaccine administration-related stress for themselves, their anticipated COVID-19 vaccine administration-related pain and stress for their child, and caregivers being of a younger age. In order to increase vaccine confidence in pediatric care, trust needs to be established with the target audience of caregivers. Providing resources and tools to address pain and stress related to vaccine administration for both children and their caregivers may help mitigate this.
Supplemental Material
sj-docx-1-bjp-10.1177_20494637221090452 – Supplemental material for A multicentre Canadian survey of caregiver perspectives on COVID vaccine-related pain and stress for their family
Supplemental material, sj-docx-1-bjp-10.1177_20494637221090452 for A multicentre Canadian survey of caregiver perspectives on COVID vaccine-related pain and stress for their family by Samina Ali, Elise Kammerer, Graham Thompson, Ahmed Mater, Manasi Rajagopal, Jeffrey N Bone, Kathryn A Birnie, Tim Oberlander, Christine T Chambers and Ran D Goldman in British Journal of Pain
Supplemental Material
sj-docx-2-bjp-10.1177_20494637221090452 – Supplemental material for A multicentre Canadian survey of caregiver perspectives on COVID vaccine-related pain and stress for their family
Supplemental material, sj-docx-2-bjp-10.1177_20494637221090452 for A multicentre Canadian survey of caregiver perspectives on COVID vaccine-related pain and stress for their family by Samina Ali, Elise Kammerer, Graham Thompson, Ahmed Mater, Manasi Rajagopal, Jeffrey N Bone, Kathryn A Birnie, Tim Oberlander, Christine T Chambers and Ran D Goldman in British Journal of Pain
Supplemental Material
sj-docx-3-bjp-10.1177_20494637221090452 – Supplemental material for A multicentre Canadian survey of caregiver perspectives on COVID vaccine-related pain and stress for their family
Supplemental material, sj-docx-3-bjp-10.1177_20494637221090452 for A multicentre Canadian survey of caregiver perspectives on COVID vaccine-related pain and stress for their family by Samina Ali, Elise Kammerer, Graham Thompson, Ahmed Mater, Manasi Rajagopal, Jeffrey N Bone, Kathryn A Birnie, Tim Oberlander, Christine T Chambers and Ran D Goldman in British Journal of Pain
Footnotes
Appendix 1
Dr Sarah Ahmed, MD, Tacoma Department of Emergency Medicine, Mary Bridge Children’s Hospital, Tacoma, WA
Dr Samina Ali, MDCM, FRCPC, Department of Pediatrics, Faculty of Medicine & Dentistry, Women and Children’s Health Research Institute, University of Alberta, Edmonton, Alberta, Canada.
Dr Julie C Brown, MD, Seattle Children’s Hospital and University of Washington School of Medicine, Seattle, WA
Dr Simon Craig, MBBS, FACEM, MPE, MPH, School of Clinical Sciences, Monash University, Melbourne, Australia.
Dr Adrienne L. Davis, MD, MSc, Pediatric Emergency Medicine, Hospital for Sick Children and University of Toronto, Ontario, Canada.
Dr Nathalie Gaucher, MD, FRCPC, PhD, Division of Emergency Medicine, Department of Pediatrics, CHU Sainte-Justine, Université de Montréal, Montréal, Québec, Canada.
Dr Gualco Gianluca, MD, Pediatric Emergency Department, Pediatric Institute of Italian part of Switzerland, Ticino, Switzerland.
Dr Ran Goldman, MD, The Pediatric Research in Emergency Therapeutics (PRETx) Program, Division of Emergency Medicine, Department of Pediatrics, University of British Columbia, and BC Children's Hospital Research Institute, Vancouver, British Columbia, Canada.
Dr Mark Griffiths, MD, Division of Pediatric Emergency Medicine, Children's Healthcare of Atlanta, Emory School of Medicine, Atlanta, GA.
Dr Jeanine E. Hall, MD, Division of Emergency and Transport Medicine, Children's Hospital Los Angeles, USC Keck School of Medicine, Los Angeles, CA.
Dr Matt Hansen, MD, MCR, Department of Emergency Medicine, Oregon Health and Sciences University, Portland, OR.
Dr Thomas L. Hurt, MD, MED, Department of Emergency Medicine, Mary Bridge Children's Hospital, Tacoma, WA.
Dr Christopher Kelly, MD, Department of Pediatric Emergency Medicine, New York Presbyterian Brooklyn Methodist Hospital, New York, NY.
Dr Eileen J. Klein, MD, MPH Seattle Children's Hospital and University of Washington School of Medicine, Seattle, WA.
Dr Eran Kozer, MD, Sackler Faculty of Medicine, Tel Aviv University, Be’er Yakov, Israel. Dr Shashidhar Marneni, MD, Department of Pediatric Emergency Medicine, Children’s Medical Center of Dallas, UT Southwestern Medical Center, Dallas, TX. Dr Ahmed Mater, MD, FRCPC, FAAP, Pediatric Emergency Medicine, Jim Pattison Children’s Hospital, and University of Saskatchewan, Saskatoon, Saskatchewan, Canada. Dr Rakesh Mistry, MD, MS, Department of Emergency Medicine, Children’s Hospital Colorado Anschutz Medical Campus, Aurora, CO Dr Cristina Parra, PhD, Hospital Sant Joan de Déu Barcelona, Pediatric Emergency Department, Barcelona, Spain. Dr Naveen Poonai, MD, FRCPC, Departments of Paediatrics, Internal Medicine, Epidemiology & Biostatistics, Schulich School of Medicine & Dentistry, Western University, and Children’s Health Research Institute, London, Ontario, Canada. Dr Arjun Rao, MD, Department of Pediatric Emergency Medicine, Sydney Children’s Hospital, Sydney, Australia. Dr David Sheridan, MD, MCR, Department of Emergency Medicine, Oregon Health and Sciences University, Portland, OR
Dr Naoki Shimizu, MD, PhD, Department of Pediatrics, St Marianna University School of Medicine, Tokyo, Japan.
Dr Esther L Yue, MD, Department of Emergency Medicine, Oregon Health and Sciences University, Portland, OR
Acknowledgements
We would like to acknowledge study coordinator MG and the research assistants at the four sites for their invaluable contribution, as well as the families for their participation in the survey.
Author Contributions
SA, RG, and EK researched literature and conceived the study. SA, RG, AM, and GT were involved in protocol development, gaining ethical approval, patient recruitment and data analysis. MR assisted in acquiring ethical approval, patient recruitment, and survey tool design. JB contributed to the analysis plan and performed statistical analyses. KB, CC, and TO co-developed the survey tool, and contributed to results interpretation. EK wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by Women and Children’s Health Research Institute (generously funded by the Stollery Children’s Hospital Foundation) to support COVID-related research at her institution.
Ethical approval
Ethics approval was obtained from each participating site’s local Research Ethics Board. The ethics board of record is based at University of British Columbia, with a study record number H20-00933.
Informed Consent
Using posters placed in waiting areas and patient rooms, as well as direct approach by healthcare team members or research staff, caregivers who arrived to EDs were asked to take part in the survey. Consent was implied once the participant selected their study site within the electronic survey. Informed consent was not sought for the present study because our ethics boards deemed it reasonable to assume that consent was implicit in the completion of a survey.
Guarantor
SA. The guarantor is the person willing to take full responsibility for the article, including for the accuracy and appropriateness of the reference list. This will often be the most senior member of the research group and is commonly also the author for correspondence.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.