
Abstract
Introduction:
Conditioning is a key mechanism of placebo and nocebo effects in adults, but little is known about these effects in youth. This study investigated whether personalized verbal cues evoking a sense of high or low self-efficacy can induce conditioned placebo and nocebo effects on subjective discomfort of noxious heat in youth.
Methods:
In a structured interview, 26 adolescents (13–18 years) described personal situations in which they experienced a sense of high, low or neutral self-efficacy. Participants were then asked to recall these memories during a conditioning paradigm, in which a high thermal stimulus applied to the forearm was repeatedly paired with a low self-efficacy cue and a low thermal stimulus with a high self-efficacy cue. In a testing phase, high, low and neutral self-efficacy cues were paired with the same moderate temperature. We hypothesized that conditioned high and low self-efficacy cues would induce conditioned placebo and nocebo responses to moderate temperatures.
Results:
Moderate temperatures were rated as more uncomfortable when paired with the conditioned low compared with the neutral self-efficacy cue (nocebo effect). While in the whole-group analysis, there was no significant difference between ratings of moderate thermal stimuli paired with high compared with neutral self-efficacy cues (placebo effect), a sub-group of participants with a greater range of emotional valence between high and neutral self-efficacy cues revealed a significant placebo effect. The strength of the nocebo effect was associated with higher anxiety and lower hope.
Conclusion:
Conditioned associations using internal self-efficacy states can change subjective discomfort of thermal sensations.
Introduction
Noxious heat can be amplified or attenuated by predictive cues, prior experience and verbal suggestions, as demonstrated by placebo and nocebo effects.1–6 While there is a growing body of research investigating the underlying mechanisms of placebo analgesia and nocebo hyperalgesia in adults, studies in adolescents are rare. 7 During adolescence, the brain is undergoing crucial changes in pain regulation regions, possibly affecting the occurrence or magnitude of placebo and nocebo effects.8–10
In adults, expectations of pain relief or pain amplification can induce placebo analgesia and nocebo hyperalgesia. 11 Expectations can be formed by learning processes, such as classical conditioning.
During these learning processes, an individual learns to associate a cue (e.g. a pill, a situation, a smell) with pain relief or pain amplification. For example, in clinical practice, the repeated pairing of a cue (e.g. pill) with pain relief can subsequently induce placebo effects by the presentation of the cue (e.g. placebo pill without intrinsic pharmacological effect). Similarly, it was shown that conditioning can change subjective discomfort of experimentally induced pain.1,2,12–15 In these paradigms, distinct visual1,16 or tactile 15 cues are repeatedly paired with pain or pain relief during a learning phase. In a testing phase, these cues are then presented with a stimulus of the same magnitude of pain. Painful cues increase the subjective discomfort (conditioned hyperalgesia or nocebo effect) and pain relief cues decrease subjective discomfort (conditioned analgesia or placebo effect) associated with the stimulus.1,13,16 Conditioned placebo and nocebo effects can also be induced when cues are presented subliminally (outside of conscious awareness, cues are presented for 12 ms only and then masked by a scrambled image), during the learning phase, during the testing phase or both during learning and testing phases,1,16 suggesting that conscious perception of cue–stimulus associations is not a requirement to experience placebo and nocebo effects.
To date, there are three published studies17–19 investigating the effect of conditioning on thermal sensations in children and youth. Both Wrobel et al. 17 and Gniß et al. 18 induced placebo analgesia in response to thermal pain by applying an inert cream paired with a combination of expectations and conditioning. Wrobel et al. 17 found a significant placebo effect, the magnitude of this effect, however, did not differ between children/youth (10–15 years) and adults. However, in children, but not in adults, the magnitude of the placebo effect was predicted by prior experience. Similarly, Gniß et al. 18 found a significant placebo effect in children (6–9 and 10–13 years) in response to conditioning, but no effect in youth (14–17 years) and adults (>18 years). Effect sizes were also small for youth and adults, and moderate for children. The magnitude of the placebo effect was predicted by prior experience in all age groups, the size of the correlation, however, decreased with age. In our previous study of Neuenschwander et al., 19 we replicated a study done in adults in youth (13–18 years). 1 The study investigated conditioning without expectations by pairing low and high temperatures with neutral visual cues. We found a significant nocebo effect, but no placebo effect. The effect size of the nocebo effect was small compared with the findings in adults.
In the present study, we investigated whether conditioning with personalized verbal cues invoking past feelings of high or low self-efficacy could induce placebo and nocebo effects in youth. Self-efficacy expectations are a person’s belief in their ability to effectively deal with a prospective situation. 20 Increasing self-efficacy reduces pain intensity and unpleasantness in induced pain. 21 Similarly, placebo and nocebo interventions can increase or decrease confidence in pain managing abilities. 22 Here, we used self-reported autobiographical memories to create personalized cues that induced a sense of low or high self-efficacy and paired these cues with high and low temperatures during a conditioning paradigm. Subsequently, we assessed whether conditioned self-efficacy cues could influence subjective perceptions of identical moderate thermal stimuli.
In adults, anxiety measures correlate negatively with placebo and positively with nocebo effects. 23 Optimism and hope are linked to stronger placebo effects and increased pain thresholds, respectively.24–26 To assess whether these associations also exist in youth, we gathered questionnaire-based measures of anxiety, hope and inherent sense of self-efficacy.
We investigated (1) whether thermal perception is modulated by conditioned low and high self-efficacy cues and (2) whether personality traits are associated with placebo and nocebo effects. We hypothesized that moderate temperatures paired with conditioned low self-efficacy/high heat cues would be perceived as more uncomfortable compared with those paired with neutral cues (nocebo effect). Moderate temperatures paired with conditioned high self-efficacy/low heat cues, conversely, would be experienced as less uncomfortable compared with those paired with neutral cues (placebo effect). Furthermore, we hypothesized that lower anxiety, higher hope and higher inherent sense of self-efficacy would be associated with stronger conditioned placebo and lower nocebo effects.
Methods
Participants
An a priori power analysis for a one-way repeated measures, analysis of variance (rmANOVA) was conducted with G*Power 27 to determine the needed sample size. A necessary sample size of n = 25 was estimated, assuming a large effect size of f =.43 and a correlation of r =.16 between the measurements as found by Jensen et al., 1 α = .05 and a 95% chance of detecting an effect. We therefore included n = 26 adolescents aged 13–18 years (53.8% girls, M = 16.13 years, SD = .84) from a local high school. Individuals with any chronic illness or medication use that would potentially interfere with the study, such as a previously diagnosed psychiatric disorder, medication that can influence cognition or emotional processing (i.e. sleep medication, antidepressants, anticonvulsants or opioids), were excluded from the study. Three participants were excluded because of technical issues (n = 1) or because they were not able to adequately differentiate low and high thermal stimuli in the reversed conditioning trials (n = 2, see description of reversed conditioning trials below).
Procedure
The study was approved by the University Research Ethics Board and the Hospital Research Review Committee. Written informed consent was obtained from adolescents and their parents. First, participants completed an autobiographical memory recall task to create individual low, high and neutral self-efficacy cues (detailed below). Then, they completed the thermal sensation paradigm, consisting of a calibration phase, a conditioning phase and a testing phase, in which participants were asked to rate thermal stimuli applied to the underside of their lower forearm. Finally, they were asked to fill out the personality questionnaires. Participants were reimbursed with a CAN$20 gift card. After the completion of the study, participants were debriefed in groups in the form of an interactive presentation at their high school. The procedure and study design are visualized in Figure 1.
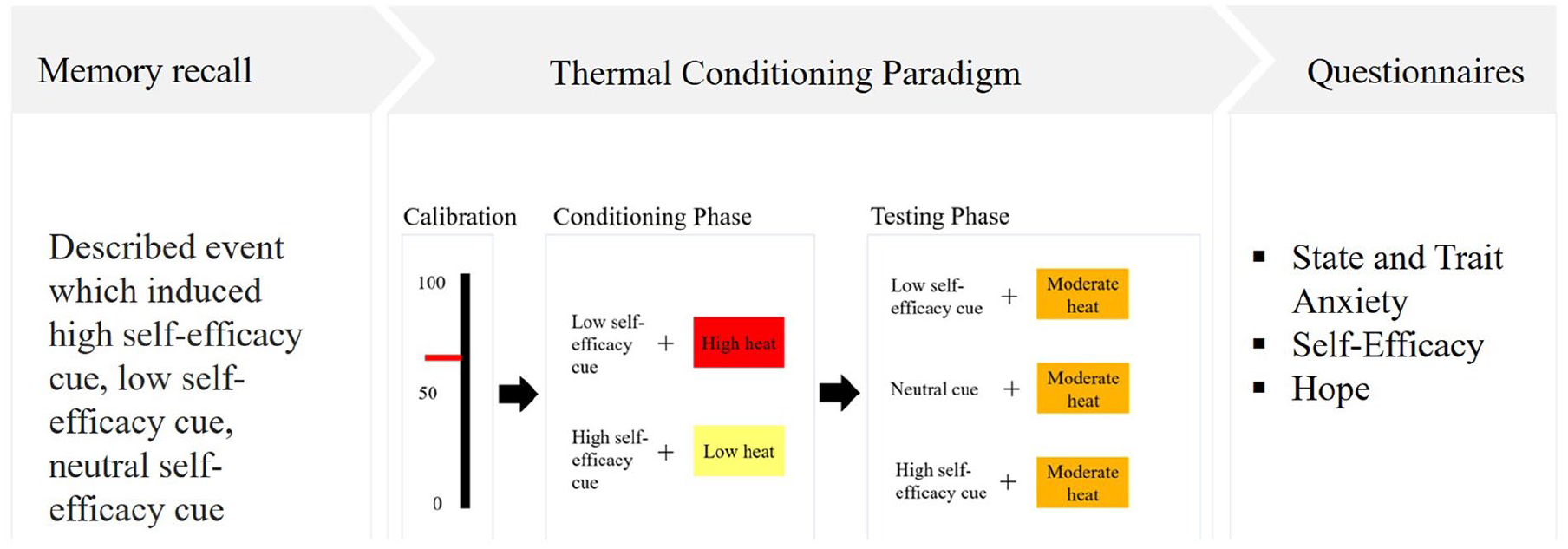
Procedure and study design.
Material
Memory recall
During the memory recall task, participants were asked to recall and write about memories in which they felt high, low and neutral self-efficacy. Memories of each kind were triggered by generic statements adapted from the general self-efficacy scale, including, ‘I was able to rely on my coping abilities’ (high), ‘I didn’t handle a difficult situation’ (low) and ‘I experienced an unforeseen event’ (neutral). 28 Furthermore, participants were instructed to write down a personal keyword (e.g. person, object, place, associated with the recalled situation) to help them to recall each of their unique memories during the thermal stimulation paradigm. At the end of the study, we also asked participants to indicate the quality of memory recall during the thermal stimulation paradigm in terms of recall success (‘During the task how often were you able to recall your memory when the sentence was presented on the screen?’, I was able to recall the memory in ___ % of time they were shown.), emotion induction (‘Were you able to feel the emotions that you felt during the recall?’, 0 = not at all, 1 = somewhat, 3 = moderately so and 4 = very much so) and difficulty (‘How difficult was it for you to recall the different memories?’, 1 = very difficult, 2 = difficult, 3 = moderate, 4 = easy and 5 = very easy).
Thermal conditioning
The thermal conditioning paradigm was adapted from previous studies by Jensen et al.1,16 It consisted of a calibration phase, a conditioning phase and a testing phase. Thermal sensations were induced with the Thermal Sensory Analyzer, using a 3 × 3 cm probe (Medoc Advanced Medical Systems, Rimat Yishai, Israel; Biomedical Engineering Device) on their left volar forearm. For each trial, thermal stimuli were presented for 4 seconds with a ramp up and ramp down of 8 degrees per second. Participants first completed a calibration phase in which a personalized high and low thermal stimulus was determined. Calibration started at 36°C. Each temperature was presented three times and then raised 1°C. After each sensation, participants were asked to rate their discomfort on a visual numeric scale between 0 (‘no discomfort’) and 100 (‘worst imaginable discomfort’). The high temperature stimulus was selected based on a subjective discomfort rating of 60 on the visual scale. In alliance with our local ethics committee, we told participants that we do not want the sensation to cause any pain and asked them to verbalize if the stimulus was getting painful. The average temperature for the high heat stimulus was 44°C (SD = 1.98°C). The low heat stimulus for each participant was determined by subtracting 3°C from their high heat stimulus. The moderate heat stimulus was determined as halfway between the two.
During the conditioning phase, the high heat stimulus was repeatedly paired with the low self-efficacy cue (low self-efficacy statement with their personalized memory keyword below). The low heat stimulus was repeatedly paired with the high self-efficacy cue (high self-efficacy statement with the individual keyword below). After each sensation, participants were asked to rate their discomfort by moving the cursor on a computerized visual numeric scale, with the computer mouse.
The conditioning phase consisted of two blocks with a total of 48 cue stimulus-heat parings, of which 36 trials were matched (18 high self-efficacy/low heat and 18 low self-efficacy/high heat), eight were reversed-pairing trials (four high self-efficacy/high heat and four low self-efficacy/low heat) and four were catch trials (two high self-efficacy/low heat and two low self-efficacy/high heat presented in green). Reversed-pairing trials had the aim of adding some uncertainty about the actual temperature and thus promoting greater attention to the heat stimulus. In catch trials, the self-efficacy cue was presented in green (as opposed to white), and participants had to press a button as fast as possible, to focus participants attention to the cues on the screen. Both reversed and catch trials were excluded from the analyses. Cues were visible for the entire duration of the thermal stimulus (4 seconds).
During the testing phase, moderate temperatures were presented with low, high and neutral self-efficacy cues. The testing phase consisted of a total of 66 trials, of which 48 were cue/moderate heat pairing trials (14 high self-efficacy cue/moderate heat, 14 low self-efficacy/moderate heat and 20 neutral self-efficacy/moderate heat), 12 were booster trials (six high self-efficacy cue/low heat and six low self-efficacy/high heat) and six were catch trials (two low self-efficacy/moderate, two high self-efficacy/moderate and two neutral self-efficacy/moderate). The booster trails were used to prevent extinction. The first trial for each block, the booster trials and catch trials were excluded from the analyses. For both conditioning and testing phases, the intertrial interval varied randomly from 3 to 5 seconds. Between blocks, participants were able to take a short break.
Questionnaires
State and trait anxiety was measured with the State Trait Anxiety Questionnaire (STAI). 29 It consists of 40 items, with an internal consistency ranging from .86 to .95 and test–retest reliability from .65 to .75. Each item was rated by participants on a 4-point Likert-type scale. The general self-efficacy scale (internal consistency ranging from .76 to .90) was used to measure an individual’s general sense of self-efficacy, and will herby referred to as inherent general self-efficacy. 28 It consists of 12 items, each rated on a 5-point Likert-type scale. Hope was measured with the hope scale. 30 This scale conceptualizes hope within the framework of goal setting, with high hope defined as successful determination of goals as well as the ability to generate pathways to meet the goals. Its internal consistency ranges from .74 to .84. It consists of eight relevant self-report scale items and four filler items. Each item is rated on an 8-point Likert-type scale, indicating how true (definitely true to definitely false) a statement is. In our study, internal consistency, as measured with Cronbach’s alpha, was α = .90 for the state anxiety scale and α = .93 for the trait anxiety scale of the STAI, α = .64 for the general self-efficacy scale and α = .84 for the hope scale.
Outcomes
The main outcome variable in the present study was subjective discomfort rated on the visual numeric scale. For the conditioning phase, mean discomfort was calculated independently for low and high heat stimuli. Sensory discrimination was defined as the difference in mean discomfort between high and low heat. In the testing phase, mean discomfort of moderate temperatures paired with high, low and neutral self-efficacy cues was calculated. The magnitude of the placebo effect was estimated by the difference in mean discomfort between the same moderate temperature paired with neutral and high self-efficacy cues. The magnitude of the nocebo effect was estimated by the difference in mean discomfort between a moderate temperature paired with low and neutral self-efficacy cues. The magnitude of the conditioning effect was calculated by the difference in discomfort between a moderate temperature paired with high or low self-efficacy cues.
Results
Statistical analyses were performed using the statistical software R, Version 3.6.1. 31 RmANOVAs were calculated with the package ezANOVA, 32 and graphics were compiled with ggplot2. 33
Memory recall
On average, participants reported that they were able to recall the memory in 78.5% of the trials. Most participants reported that they were ‘moderately’ able (65.4%, rating 3 on a 4-point scale) or ‘very much’ able (11.5%, rating 4) to feel their emotions while recalling their personal memories. Some rated their emotional recall ability as ‘somewhat’ (19.2%, rating 2). One participant was ‘not at all’ able to feel the emotion (3.6%, rating 1). In terms of the difficulty recalling the memories, 11.5% of participants found it difficult, 34.6% found it moderate, 46.15% found it easy and 7.7% found it very easy to recall different memories.
Thermal sensory discrimination
The difference between discomfort ratings associated with low and high heat stimuli is defined as sensory discrimination. To test whether participants could reliably differentiate low and high temperature stimuli, a one-way rmANOVA with temperature (low versus high) as a within-subjects factor was conducted on discomfort ratings acquired during the conditioning phase. Participants rated the low heat stimulus as significantly less uncomfortable (M = 12.85, SD = 14.95) compared with the high heat stimulus (M = 53.75, SD = 16.99), F(1, 25) = 149, p < .001, indicating that participants were able to discriminate between the different temperatures.
Thermal conditioning
Changes in subjective thermal perception caused by conditioning were assessed with a one-way rmANOVA on discomfort ratings acquired during the testing phase, with cue type (high, low or neutral self-efficacy) as a within-subjects factor. There was a significant main effect of cue type, indicating differences in discomfort ratings across the three cue types, F(1, 25) = 25.23 p < .001 (Figure 2). Standard errors were corrected for between-subject variability according to Cousineau. 34 Pairwise Bonferroni-corrected post hoc t-tests showed a significant overall conditioning effect (Mdiff = 6.40, p < .001), indicating that participants rated moderate thermal stimuli as more uncomfortable when paired with a conditioned low self-efficacy cue compared with a conditioned high self-efficacy cue. Furthermore, there was a significant nocebo effect (Mdiff = 5.66, p < .001), indicating that participants rated moderate thermal stimuli as more uncomfortable when paired with a conditioned low self-efficacy cue compared with a neutral self-efficacy cue. There was no significant placebo effect (Mdiff = .74, p = .930), indicating that there was no statistical difference between discomfort ratings for conditioned high and neutral self-efficacy cues.
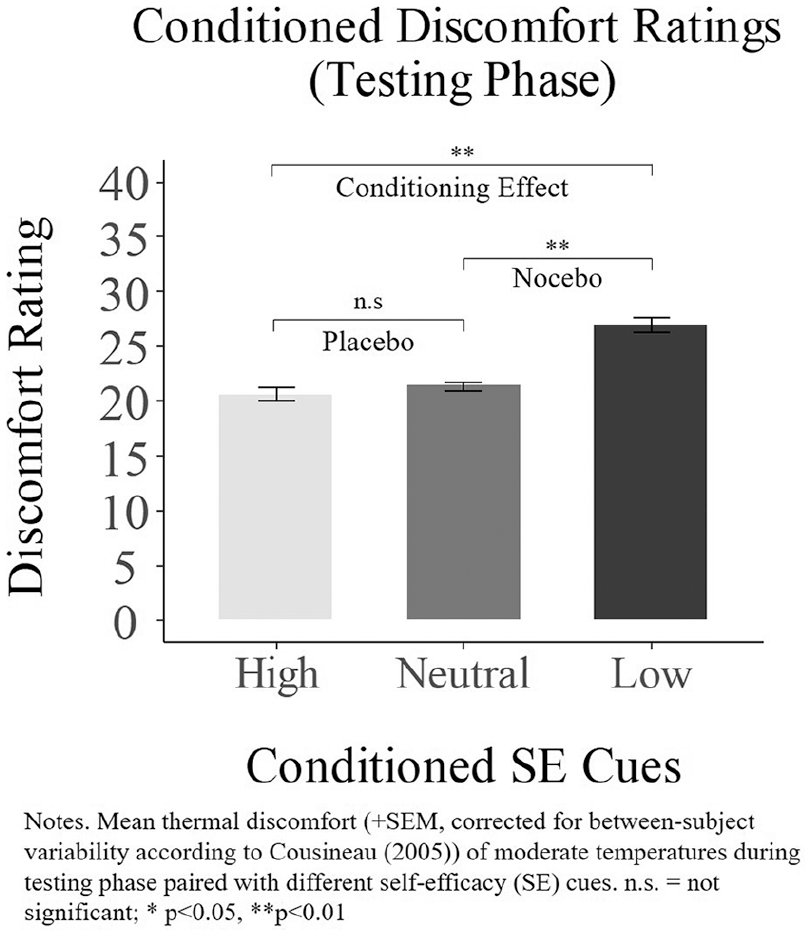
Discomfort of moderate temperatures paired with conditioned self-efficacy cues.
Given the absence of the hypothesized placebo effect, we tested whether the range in emotional valence between high and neutral self-efficacy cues may have weakened potential placebo conditioning. During the memory recall, participants were asked to recall different memories associated with an experienced sense of low, high or neutral self-efficacy. All of the high self-efficacy states were usually described as negative situations that were turned to a positive outcome by the participant. For the neutral self-efficacy memory, we used the sentence ‘I experienced an unexpected situation’. The emotional valence of memories recalled for the neutral situations varied greatly between participants. Some were more positive (‘I found money’) and others were more negative (‘My group members . . . didn’t turn up’). Positive neutral experiences might have masked any placebo effect by decreasing discomfort ratings, to a level similar to ratings in response to high self-efficacy cues. To test this possibility, we asked two blinded independent raters to rate the emotional valence of the neutral memories (5-point Likert-type scale: 1 = ‘very positive’, 2 = ‘positive’, 3 = ‘neutral’, 4 = ‘negative’ and 5 = ‘very negative’). There was a strong significant inter-rater correlation (r = .83, p < .001). We then reran rmANOVA on discomfort ratings acquired during the testing phase, excluding seven participants whose neutral self-efficacy memories were rated as positive or very positive. For this subsample (n = 19), we again found a significant main effect of cue type, F(2, 36) = 18.74, p < .001 (Greenhouse–Geisser-corrected). Bonferroni-corrected post hoc paired t-tests additionally revealed a significant placebo effect, indicating that moderate temperatures paired with the conditioned high self-efficacy cue were rated as less uncomfortable compared with the neural self-efficacy cue (Mdiff = 1.31, p = .037). Both conditioning (Mdiff = 6.54, p < .001) and nocebo effects (Mdiff = 5.24, p < .001) also remained significant.
We also conducted a subsequent analysis to investigate whether the ability to engage in emotional recall as well as the valence of the neutral self-efficacy states influenced conditioned nocebo and placebo effects. Participants showed a significant positive correlation between the self-reported emotional engagement (‘Were you able to feel the emotions that you felt during the recall?’, 0 = not at all, 1 = somewhat, 3 = moderately so, 4 = very much so) during the study and the strength of the conditioned nocebo effect (spearman’s rho = .60, p = .001), suggesting that the ability to induce an emotional state of self-efficacy influenced the magnitude of the nocebo effect.
To test whether better discrimination between low and high heat sensations in the conditioning phase predicted the strength of the conditioning effect observed in the testing phase, we computed a Pearson correlation between sensory discrimination (high–low temperature rating during conditioning) and the conditioning effect (low–high self-efficacy cue rating). There was no significant correlation between sensory discrimination and the conditioning effect (r = .17, p = .399), presented in Figure 3.
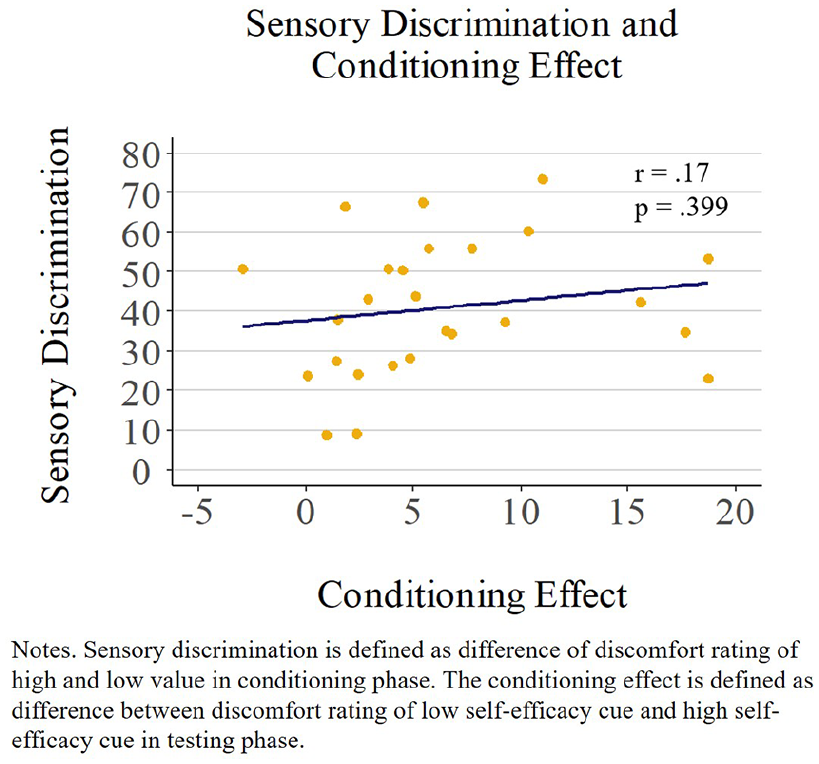
No significant association between sensory discrimination and the conditioning effect.
Effect sizes
To compare the strength of the effects with previous studies in adults, we calculated the effect size (Cohen’s d) for the conditioning effect (testing phase). In this current study, differences in discomfort between low and high conditioned cues were moderate d = .37. In contrast, effect sizes were larger in the adult conditioning study mentioned previously, with d = .86 for supraliminal cue presentation (Exp. 1) and d = .58 for subliminal cue presentation (Exp. 2). 1
Personality traits
A multiple regression analysis was conducted to identify unique contributions of individual differences in personality traits (hope, self-efficacy and anxiety) to the magnitude of conditioned placebo and nocebo effects. This analysis, however, revealed high multicollinearity between factors, as presented in Table 1.
Correlation matrix of trait and state anxiety, self-efficacy and hope.
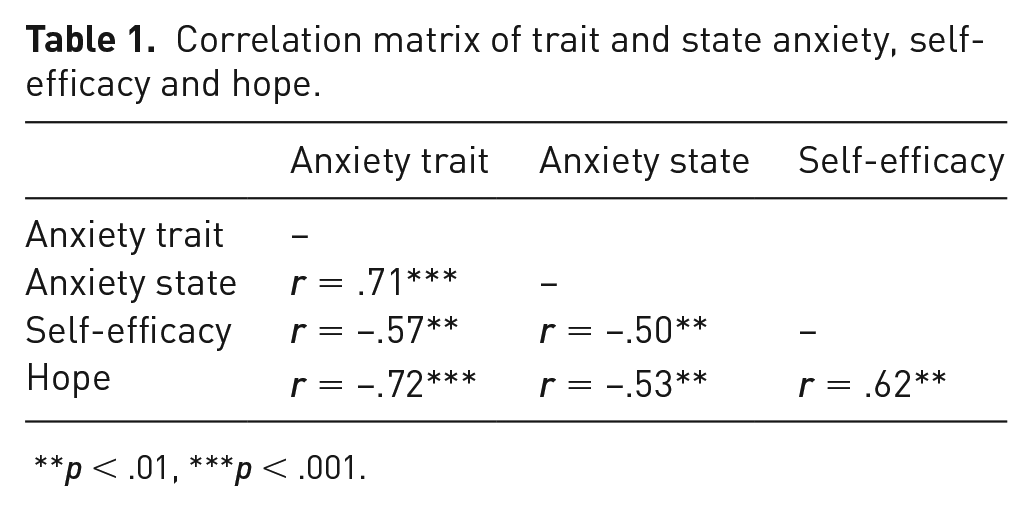
p < .01, ***p < .001.
We therefore calculated the correlation of each personality variable with the magnitude of the conditioned nocebo effect independently. As can be seen in Figure 4, trait anxiety (r = .46, p = .018), but not state anxiety (r = .18, p = .391), correlated significantly with the conditioned nocebo effect, meaning that participants with a higher general (trait) level of anxiety, but not a higher level of transient (state) anxiety, showed a stronger nocebo effect. There was also a negative correlation between hope and the magnitude of the nocebo effect (r =−.48, p = .012) indicating that participants with lower general measures of hope showed a higher nocebo effect. Inherent general self-efficacy did not correlate significantly with the magnitude of the nocebo effect (r =−.12, p = .576). Thus, both trait anxiety and hope predicted the magnitude of the nocebo effect. When both factors were included in a regression analysis, the regression model significantly explained 19.6% of the variance in the magnitude of the nocebo effect (F(2, 23) = 4.06, p = .031). None of the predictors, however, reached significance (trait anxiety: β = .09, p = .369; hope: β = −.18, p = .235). As anxiety and hope are strongly, negatively correlated, this might suggest that the factors explain the same amount of variance related to the magnitude of the nocebo effect, and hence do not reach significance if included in the same regression model.
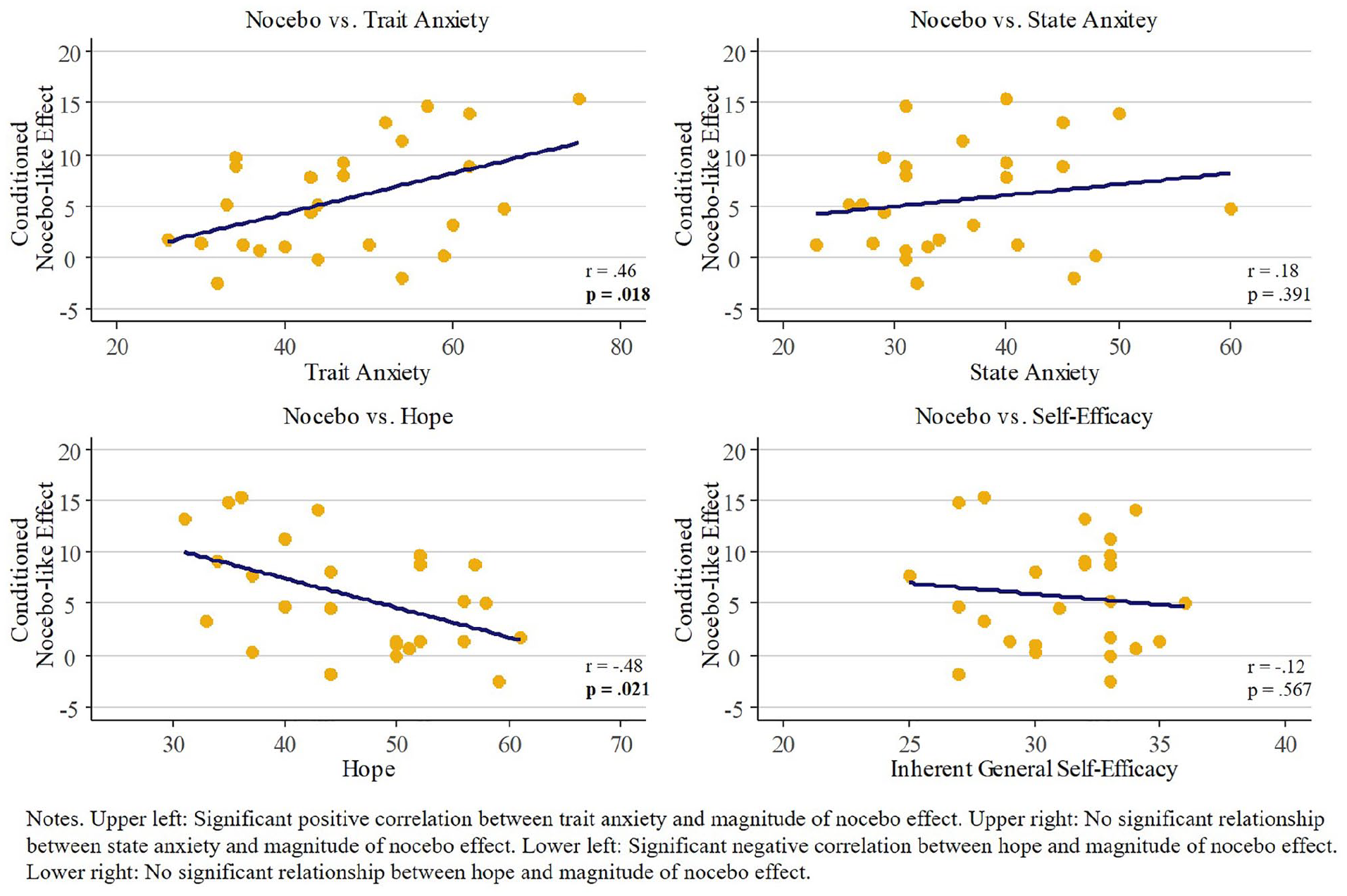
Correlations between different personality traits and the magnitude of the nocebo effect.
There were no significant correlations between the magnitude of any of the personality traits and the whole-group placebo effect (inherent general self-efficacy (r =−.19, p = .351), hope (r = .16, p = .416) and anxiety (trait: r = .15, p = .446; state: r = .36, p = .07)). This is not surprising given that no significant placebo effect was observed in the whole-group data.
Discussion
Conditioning with personalized self-efficacy cues can induce nocebo effects on thermal sensations in youth. Furthermore, the magnitude of the conditioned nocebo effect was associated with higher anxiety and lower hope. There was also evidence from a follow-up analysis that conditioned positive self-efficacy cues can induce placebo effects if there was a large enough range in emotional valence between high and neutral self-efficacy cues.
In adults, predictive cues, as established by conditioning paradigms, can amplify or attenuate subjective thermal discomfort. While there is a growing body of research investigating the underlying mechanisms and moderators of placebo analgesia and nocebo hyperalgesia in adults, studies in adolescents are rare. In this study, we adapted a study design previously shown to induce placebo analgesia and nocebo hyperalgesia in adults 1 and to influence thermal discomfort in youth. 19 Instead of using inherently meaningless visual cues, we utilized personalized autobiographical memory cues designed to evoke states of low, high and neutral self-efficacy. In the conditioning phase, high self-efficacy cues were paired with low temperatures, and low self-efficacy cues were paired with high temperatures. In the testing phase, these conditioned cues as well as a neutral (unconditioned) self-efficacy cues were presented with moderate temperatures. Adolescents rated moderate thermal sensations as more uncomfortable when paired with conditioned high heat (i.e. low self-efficacy) cues compared with a conditioned low heat (i.e. high self-efficacy) cues. Furthermore, as seen in a previous adult study, we found a significant nocebo effect, showing that adolescents rated moderate temperatures as more uncomfortable when paired with the conditioned low self-efficacy cue compared with the neutral self-efficacy cue. The placebo effect, while not significant in the whole-group analysis, was present for a sub-group of participants for whom the difference in emotional valence between high and neutral self-efficacy memories was larger.
Previous studies investigating conditioned placebo effects in youth show conflicting results. Wrobel et al. 17 and Gniß et al. 18 induced placebo analgesia in response to thermal pain by applying a placebo analgesic cream paired by a combination of expectations and conditioning. While Gniß et al. 18 did not find significant placebo effects in youth, but in children, the placebo analgesia in Wrobel et al.’s 17 study did not differ between youth/children and adults. In our previous study, we found a significant nocebo effect, but no placebo effect, with a smaller effect size compared with studies with adults. 19
Successful conditioning requires integrating conditioned and unconditioned stimuli, as well as establishing a predictive mental model to create a strong expected contingency between them. Wrobel et al. 17 explicitly instructed participants about the association between the conditioned cue and pain relief, and reinforced this expectation by conditioning a placebo analgesic cream with lower temperature thermal stimulation and thus lower experienced pain. In our present study, youth had to establish the predictive model implicitly during the conditioning paradigm. Thus, it seems that our implicit conditioning procedure (i.e. no explicit verbal suggestions to induce expectations were given), was overall only effective to induce nocebo, but not placebo effects. One explanation could be found in protective or survival mechanisms, whereby the need for self-protection from experiencing pain may have more easily turned participants into nocebo responders.
In addition, other developmental and/or methodological factors may account for differences in our findings in youth compared with findings in adult samples. Thillay et al. compared the performance of adults and adolescents in a visual predictive task. In this task, participants were presented a visual target that could be predicted by a known sequence of stimuli. 35 In their study, adolescents did not differ from adults in their reactions to the visual target, demonstrating that adolescents are able to utilize predictive cues. However, they found that the temporal brain mechanisms related to sustained attention, which was associated with better performance in the cue detection task, are still maturing during adolescence. Furthermore, the ability to distinguish between threat and safety cues is still maturing in youth. 36 Differences in the strength of conditioning between adults and youth might therefore be heightened when the predictive model linking cues and stimuli has to be established implicitly, and might also be dependent on the used cues. It is also possible that more trials are needed in youth to induce a similar magnitude of placebo and nocebo effects as in adults. Interestingly, in adults, fewer trials are necessary to induce conditioned nocebo effects compared with placebo effects, 37 which might also explain why we found a significant nocebo, but not placebo effects in the whole-group analysis.
Typically, the range in subjective ratings between low and high temperature stimuli during the conditioning phase predicts the magnitude of conditioned placebo and nocebo effects in response to impersonal conditioned cues.1,17 Here, however, we did not find this relationship. Rather, our findings suggest that the nature of the conditioned cues themselves, such as their emotional valence, may influence the strength of the conditioning effects. In line with this, subsequent analyses showed that the self-reported ability to recall the emotional states during the thermal perception paradigm correlated positively with the nocebo effect. In these subsequent analyses, we also found that significant placebo effects in a subsample of adolescents for whom the neutral self-efficacy states were truly neutral (as opposed to positively biased). Thus, controlling for the emotional valence of the neutral self-efficacy states strengthened our conditioning paradigm. While previous research did not find an effect of what type of visual cues were used during conditioning of placebo and nocebo effects (images, faces and words), 38 it is well known that pain can be modulated by emotional states.39,40 Negative emotional states increase pain, whereas positive emotional states decrease pain, independent of the arousal induced by these distinct emotional states. 40 Interestingly, in a study by Valentini et al. 41 , the induction of conditioned placebo effects was dependent on the emotional content added to the predictive cues. Similarly, Williams and Rhudy 42 found, in a fear conditioning paradigm, that fearful cues associated with a painful stimulus decreased pain thresholds in a subsequent testing phase, whereas, happy cues associated with a painful stimulus did not decrease pain thresholds. Suggesting, in line with the preparedness theory, 43 that intuitive associations have a stronger effect on the manipulation of sensory perception.
We furthermore investigated whether the magnitude of placebo and nocebo effects was predicted by individual differences in personality traits. Both higher trait anxiety and lower hope, but not state anxiety or inherent general self-efficacy, were associated with a greater nocebo effect. Trait anxiety and hope were strongly negatively correlated, and our regression model suggested that both variables explained the same variance rather than having independent additive effects. Our findings are in line with previous studies in adults, showing that stronger nocebo effects could be induced in high compared with low anxiety individuals. 22 In a series of studies, Benedetti et al.,44,45 Colloca and Benedetti 46 and Rotzinger and Vaccarino 47 have shown that nocebo effects can be blocked by the inhibition of the neurotransmitter, cholecystokinin (CCK), which is associated with anxiety-related behaviour and can facilitate pain. CCK antagonists can block nocebo effects suggesting that anxiety or autonomic arousal might moderate nocebo effects.46,48 However, the magnitude of the nocebo effect in our study was associated with (general and possibly attentional-related differences in) trait anxiety, but not with (transient and possibly arousal-related differences in) state anxiety. We assessed state anxiety after the thermal conditioning paradigm, thus, trial by trial ratings of state anxiety might reveal different results, possibly capturing arousal-related differences reflected in state anxiety.
As predicted, hope was negatively correlated with the magnitude of the nocebo effect. This is in line with previous studies linking high hope to increases in pain tolerance. 25 Pulvers and Hood 26 suggest that personality traits might influence pain perception by engaging constructive thinking styles and counteract pain catastrophizing. This may be reflected by the negative correlation between anxiety and hope in our data set. The reason why inherent general self-efficacy was not associated with the nocebo effect remains speculative. Possibly, variance in nocebo effects associated with this personality trait was already explained by the conditioning cues (i.e. high and low self-efficacy memories).
There were no significant associations between any of the personality traits with the magnitude of the placebo effect. These findings, however, need to be interpreted with caution, as the placebo effect did not reach significance in the whole-group analysis.
Future studies
Conditioning can induce nocebo effects on thermal perception in youth. While the effect size was stronger in this study of self-efficacy compared with previous studies using visual conditioning cues in youth, 19 the perceived difference in discomfort was small, and thus not likely to have direct clinical utility without further investigation into potential applications. Our study suggests that either the emotional valence of our predictive cues or the duration of the cue presentation may have enhanced the magnitude of the conditioned effects. Future studies addressing emotional valence, duration and number of trials are needed to understand differences in conditioned placebo and nocebo effects between youth and adults. We furthermore suggest replicating the study with a different neural self-efficacy sentence, as the recalled memories varied greatly among participants. Although a more subtle distinction, it also remains unclear whether conditioned nocebo effects were observed as a result of truly evoking mental states of low self-efficacy with the autobiographical memory cues or rather as a result of their more negative emotional valence of the recalled memories. Future studies could use a different approach to induce low and high states of self-efficacy and add a control group with other salient emotional predictive cues. It may also be of interest to investigate the influence of pain-related self-efficacy cues on thermal sensations, for example, the explicit expectation of being able to overcome or influence pain. Finally, our main outcome variable was self-reported thermal discomfort, which can be subject to demand effects. That is, participants’ responses may have been biased towards what they inferred was the hypothesized effect, artificially increasing ratings for warmer temperatures and vice versa. While we implemented catch trials, reversed conditioning and reminded participants to focus on what they feel during on their report, this possibility cannot be ruled out entirely. Adding more objective measures of genuine subjective experience, such as skin conductance, facial expression or contingent negative variation measured by electroencephalography, 5 might contribute to more reliable estimates of placebo and nocebo effects.
Finally, we would like to suggest adding other age groups (e.g. children, adults and elderly) in future studies. This will allow to understand developmental aspects of conditioned placebo and nocebo effects more specifically.
In this study, a conditioning paradigm was used to investigate mechanisms underlying placebo and nocebo effects on thermal perception in youth. Our study demonstrated that evoking low and high self-efficacy mental states using personalized autobiographical cues induced can induce significant conditioned nocebo and placebo effects on somatosensory perception. Higher anxiety and lower hope were associated with the magnitude of the nocebo effect. The longer term goal of this line of research is to understand the mechanisms of placebo and nocebo effects in youth, and how to harness the first and avoid the latter in the clinical setting.
Footnotes
Acknowledgements
The authors thank all adolescents for their participation, teachers and principals for their support during data collection.
Author contributions
All authors have discussed the results and commented on the article. Thus, our authorship is based on (1) substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data; (2) drafting the article or revising it critically for important intellectual content and (3) final approval of the version to be published. E.W. was responsible for the research question, designing the study, data collection and analysis, and wrote the first version of the article. R.N., K.J. and T.F.O. contributed to the design of the study. C.T. was responsible for overseeing the development of research design and research question, data analysis and article preparation. All authors contributed to article revision, read and approved the submitted version.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
The study was approved by the University of British Columbia Behavioural Research Ethics Board or University of British Columbia Clinical Research Ethics Board and the BC Women’s Hospital Research Review Committee, certificate number: H16-01192.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by an M.I.N.D. Theme Catalyst Grant from BC Children’s Hospital Research Institute to C.T. and T.F.O., an Investigator Establishment Award to C.T. and a postdoctoral fellowship from Brain Canada/NeuroDevNet to R.N.
Guarantor
T.F.O. is the guarantor of this article.
Informed consent
Written informed consent was obtained from the parents or legal guardians, as well as written informed assent from participants themselves for their anonymized information to be published in this article.