
Abstract
Aims:
The purpose of this study was to determine (a) the ability of serial high-sensitivity cardiac troponin T measurements to rule out acute myocardial infarction and (b) the ability of a single high baseline high-sensitivity cardiac troponin T measurement to rule in acute myocardial infarction in patients presenting to the emergency department with acute chest pain.
Methods and results:
Embase, Medline, Cochrane, Web of Science and Google scholar were searched for prospective cohort studies that evaluated parameters of diagnostic accuracy of serial high-sensitivity cardiac troponin T to rule out acute myocardial infarction and a single baseline high-sensitivity cardiac troponin T value>50 ng/l to rule in acute myocardial infarction. The search yielded 21 studies for the systematic review, of which 14 were included in the meta-analysis, with a total of 11,929 patients and an overall prevalence of acute myocardial infarction of 13.0%. For rule-out, six studies presented the sensitivity of serial measurements <14 ng/l. This cut-off classified 60.1% of patients as rule-out and the summary sensitivity was 96.7% (95% confidence interval: 92.3–99.3). Three studies presented the sensitivity of a one-hour algorithm with a baseline high-sensitivity cardiac troponin T value<12 ng/l and delta 1 hour <3 ng/l. This algorithm classified 60.2% of patients as rule-out and the summary sensitivity was 98.9% (96.4–100). For rule-in, six studies reported the specificity of baseline high-sensitivity cardiac troponin T value>50 ng/l. The summary specificity was 94.6% (91.5–97.1).
Conclusion:
Serial high-sensitivity cardiac troponin T measurement strategies to rule out acute myocardial infarction perform well, and a single baseline high-sensitivity cardiac troponin T value>50 ng/l to rule in acute myocardial infarction has a high specificity.
Introduction
In recent years, increasing number of hospitals worldwide have adopted the high-sensitivity cardiac troponin T (hs-cTnT) assay as the reference marker of myocardial necrosis. These new cardiac biomarkers have proven to be more sensitive and faster in detecting myocardial damage. 1
These features are especially desirable in patients who present at the emergency department (ED) with non-differentiated acute chest pain, where a timely diagnosis is essential. Acute chest pain is the second most common reason for visits to the ED.2,3 Only 10–20% of these patients are eventually diagnosed with acute myocardial infarction (AMI). However, missing this diagnosis may have grave consequences.1,4 Various strategies have been suggested for safe and early discharge of patients based on serial or a single low value of hs-cTnT balanced with the clinical presentation. In conjunction with these rule-out strategies, a direct rule-in strategy has also been proposed for patients with highly abnormal baseline hs-cTnT values. 5
The aim of this systematic review and meta-analysis was to determine (a) the ability of serial hs-cTnT measurements to correctly rule out AMI and (b) the ability of a single high baseline hs-cTnT measurement to correctly rule in AMI in patients presenting to the ED with acute chest pain.
Methods
We conducted a systematic review and meta-analysis of the literature in agreement with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 6
Search strategy
The following databases were searched on 12 April 2017: Embase, Medline Ovid, Cochrane CENTRAL, Web of Science and Google scholar, without a restriction on the publication date. Only articles in English were included. The strategies for the literature search are provided in the Supplementary Material Table S1. Reference lists of relevant papers including systematic reviews were hand searched for potentially relevant additional studies.
Study inclusion
Titles and abstracts were independently screened by two investigators (MA and EAD) and selected for further evaluation if they met the following criteria: (a) the publication was a prospective cohort study published in a peer-reviewed journal; (b) patients were adults; (c) patients presented to the ED with symptoms suggestive of an acute coronary syndrome; (d) the diagnostic accuracy of the Roche Elecsys hs-cTnT was evaluated; (e) the primary endpoint was an admission diagnosis of AMI based on the universal definition of AMI. 7 Full-text articles were then retrieved and independently screened for inclusion by both investigators (MA and EAD). In case of disagreement, a consensus was reached by joint reading. There were no restrictions on the type of troponin assay used as part of the reference standard. Studies were excluded if they missed diagnostic accuracy data relevant to our research questions or if there were insufficient data for the derivation of 2×2 contingency tables. The screening process was performed with the reference manager Endnote X7 using the method proposed by Bramer et al. 8
Methodological quality assessment
The methodological quality of the included articles was independently assessed by two investigators (MA and EAD) using the Quality Assessment of Diagnostic Accuracy Studies (QUADAS-2) tool. 9 In case of disagreement, consensus was reached by joint reading or by consulting a third investigator (AD).
Data extraction and statistical analysis
Using a standardised data extraction form, one investigator (MA) extracted relevant details concerning the study design (e.g. study population, inclusion period, target condition and reference standard), the patient characteristics and study results relevant to our research questions. The extracted data were then verified by two investigators (EAD and AD).
First, we were interested in the capability of serial hs-cTnT measurements to correctly rule out AMI. For studies reporting the diagnostic accuracy of serial measurements, the timing of the troponin measurements and the reported cut-offs were extracted. Subsequently, the extracted data were assessed on appropriateness for quantitative analysis. If appropriate, 2×2 contingency tables were constructed for the individual studies and thereafter the sensitivity was calculated with 95% confidence intervals (CIs). In the case of overlapping samples, only the publication with the largest cohort was included in the quantitative analysis.
Second, we were interested in the capability of a single high baseline measurement to correctly rule in AMI. A single high baseline measurement was defined as a baseline hs-cTnT value> 50 ng/l. This cut-off was chosen because it resembles the cut-off point for direct rule-in recommended by the European Society of Cardiology (ESC). 5 After constructing 2×2 contingency tables, the specificity for each study was calculated with 95% CI.
Statistical analysis
Because of our dual research question, we were primarily interested in obtaining the summary estimate of sensitivity of serial hs-cTnT measurements to rule out AMI, and the summary estimate of specificity of a single high hs-cTnT value to rule in AMI. In addition, we also calculated the other parameters of diagnostic accuracy for both research questions, i.e. negative predictive value (NPV), specificity and positive predictive value (PPV) for serial hs-cTnT measurements; and PPV, sensitivity and NPV for a single high baseline hs-cTnT value. To this end, a meta-analysis for proportions was performed by applying random effects models. Briefly, the Freeman-Tukey double arcsine method was used to transform the sensitivity, NPV, specificity and PPV estimates for each study.10,11 These were then used to calculate weighted summary estimates and their 95% CIs under the random effects model. 12 Heterogeneity was assessed with the I2 statistic.13,14
Due to the limited number of studies in the quantitative analyses (<10), subgroup analyses and meta-regression were not performed. Publication bias was not investigated, because of suboptimal performance of standard tests and funnel plots in diagnostic test accuracy (DTA) studies and little evidence of the existence of publication bias in DTA studies to this date. 15 All statistical analyses were performed using Microsoft Excel 2010 (Microsoft Corporation, Redmond, Washington State, USA) and MedCalc statistical software version 18 (MedCalc Software bvba, Ostend, Belgium).
Results
The systematic literature search generated 625 potentially relevant citations. An additional article was identified through a hand search of reference lists of relevant papers. After titles and abstracts screening, 539 studies were excluded. The remaining 87 articles were assessed in full-text, after which 66 studies were excluded for various reasons (Figure 1). Of the 21 articles discussed in the present systematic review (Table 1),16–36 14 studies were included in the meta-analysis with a total of 11,929 patients and an overall prevalence of AMI of 13.0% (range 3.6–56%)17,19,20,24–27,29–33,35,36
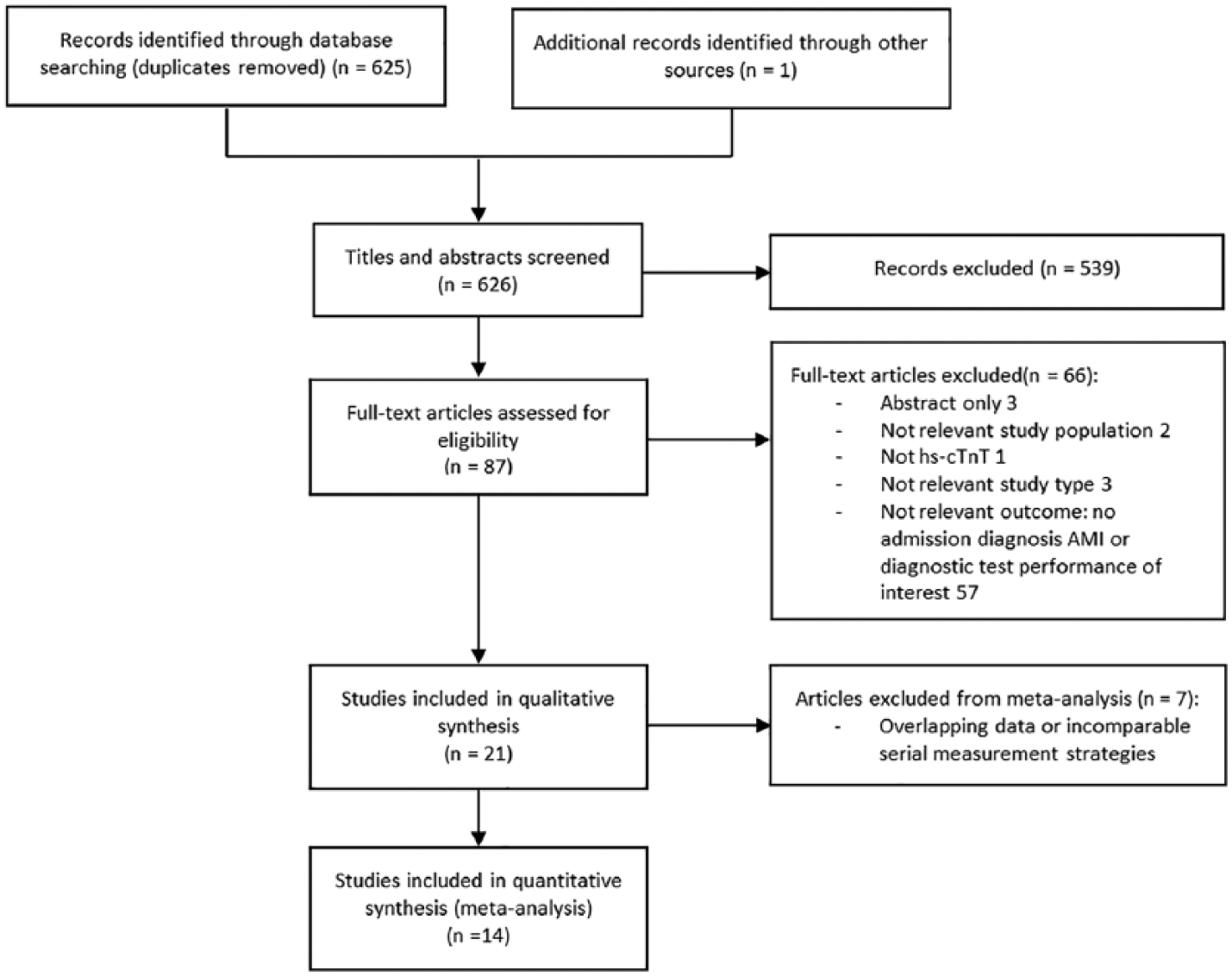
Flow diagram: study inclusion process for the systematic review and meta-analysis.
Study and patient characteristics of all studies included in the systematic review.
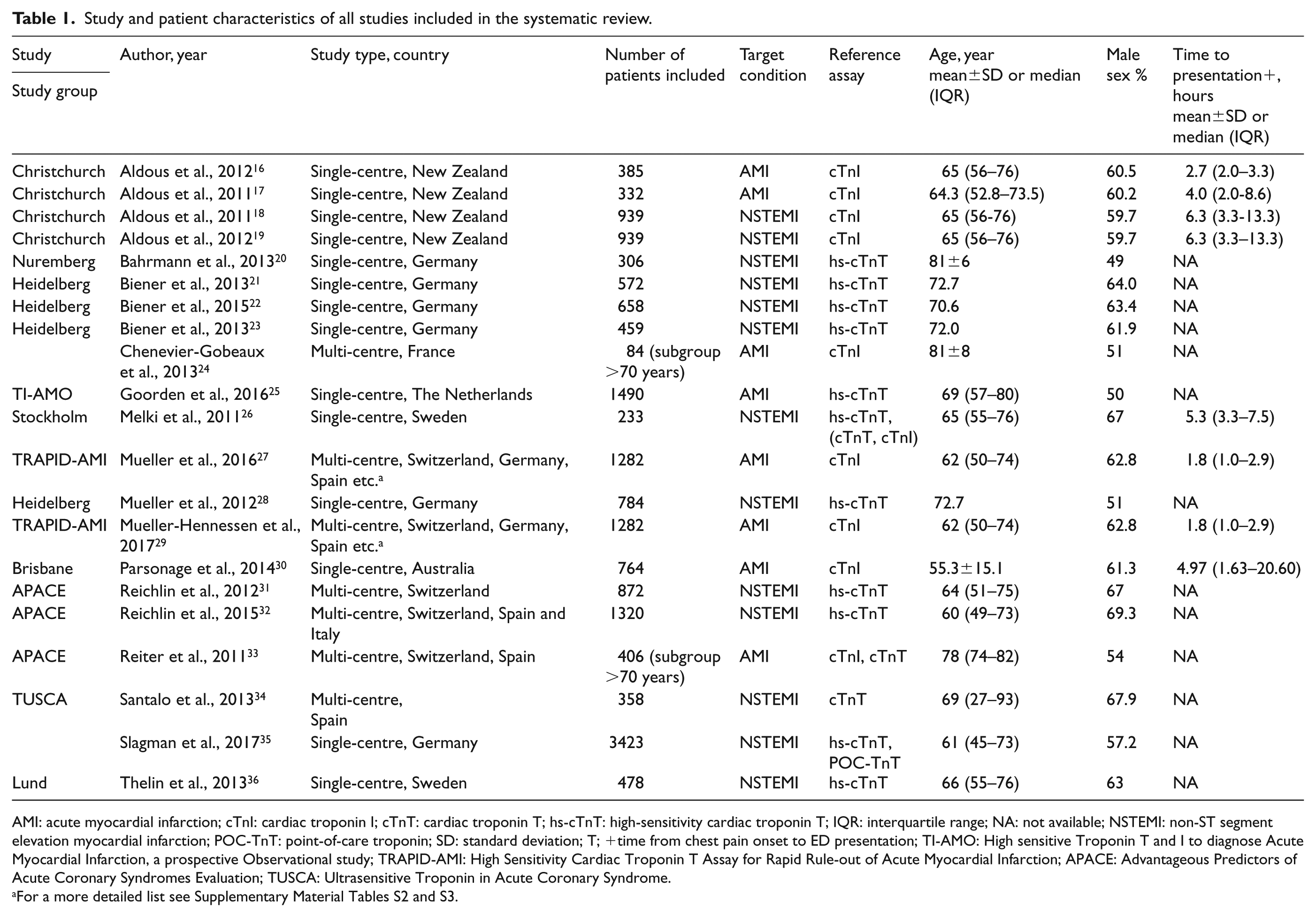
AMI: acute myocardial infarction; cTnI: cardiac troponin I; cTnT: cardiac troponin T; hs-cTnT: high-sensitivity cardiac troponin T; IQR: interquartile range; NA: not available; NSTEMI: non-ST segment elevation myocardial infarction; POC-TnT: point-of-care troponin; SD: standard deviation; T; +time from chest pain onset to ED presentation; TI-AMO: High sensitive Troponin T and I to diagnose Acute Myocardial Infarction, a prospective Observational study; TRAPID-AMI: High Sensitivity Cardiac Troponin T Assay for Rapid Rule-out of Acute Myocardial Infarction; APACE: Advantageous Predictors of Acute Coronary Syndromes Evaluation; TUSCA: Ultrasensitive Troponin in Acute Coronary Syndrome.
For a more detailed list see Supplementary Material Tables S2 and S3.
Study and patient characteristics
In studies that reported time to presentation, the median time to presentation ranged from one hour 27 to 6.3 h (Table 1).18,19 The proportion of women varied from 30.7% 32 to 51%. 20 Fourteen out of 21 studies excluded patients with ST-segment elevation myocardial infarction (STEMI) from the analysis. Four studies had a hs-cTnT threshold>14 ng/l as part of their inclusion criteria21–23,28 (see Supplementary Material Table S2). Eleven studies used the hs-cTnT assay as part of their reference standard.20–23,25,26,28,31,32,35,36 Additional characteristics of all included studies, such as the reported cut-offs and the timing of the troponin measurements for serial measurement strategies can be found in Supplementary Material Tables S2, S3 and S5.
Methodological quality assessment
The results of the QUADAS-2 methodological quality assessment are provided in Supplementary Material Table S4. Eight studies consecutively enrolled patients presenting to the ED.17,20–24,34,35 Eleven studies used the hs-cTnT assay as part of their reference standard and were considered as high risk for incorporation bias.20–23,25,26,28,31,32,35,36 Seven studies did not exclude STEMI patients,16,17,25,27,29,30,33 thus raising concerns about applicability. All studies formally re-adjudicated the final diagnoses, except the study by Slagman et al. 35 in which the initial clinical diagnosis was used to establish the endpoints. Reference assay cut-offs used for defining the endpoint differed between the various papers that used a standardised adjudication process (see Supplementary Material Table S4).
Meta-analysis
Serial measurements of hs-cTnT for rule-out of AMI
Out of the 14 studies that were included in the meta-analysis, nine studies reported the diagnostic accuracy of serial measurements.17,19,20,26,27,30–32,36 Six of these studies presented the sensitivity of serial hs-cTnT measurements <14 ng/l (99th percentile).17,19,20,26,30,36 The median time of serial troponin measurement was 2.5 h (range, two to 6–24 h). The prevalence of AMI ranged from 7.3–56%. Applying the 99th percentile as cut-off classified 60.1% (range, 32.0–77.7%) of patients as rule-out (see Supplementary Material Table S6). The summary sensitivity of serial hs-cTnT measurements <14 ng/l was 96.7% (95% CI: 92.3–99.3; I2=82.1) (Figure 2). The NPV’s of the individual studies varied from 94.7% to 100% (see Supplementary Material Figure S1). For completeness, the summary estimates of NPV, specificity and PPV are provided in Supplementary Material Figures S1–S3.
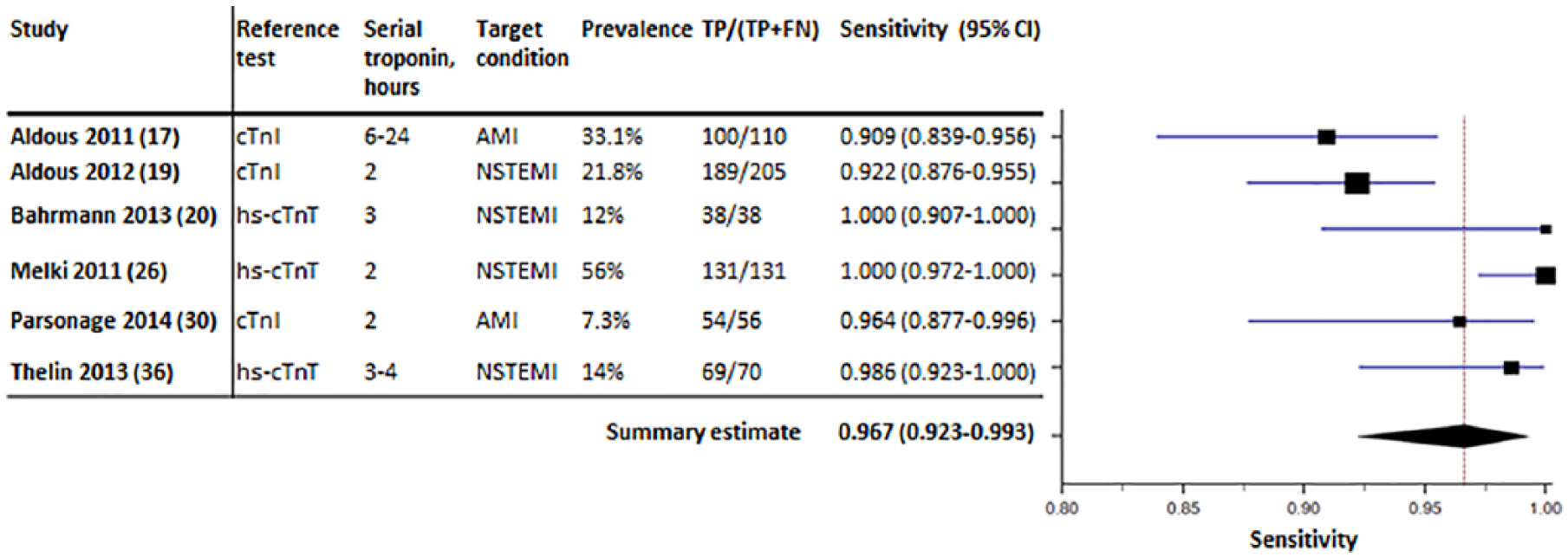
Forest plot displaying the summary estimate of sensitivity of serial high-sensitivity cardiac troponin T (hs-cTnT) measurements <14 ng/l (99th percentile).
The remaining three studies used a one-hour algorithm for serial measurements and presented the sensitivity of a baseline hs-cTnT value<12 ng/l and delta (Δ) 1 h<3 ng/l.27,31,32 The prevalence of AMI was comparable between the studies, ranging from 16.6–17.3%. The one-hour algorithm classified 60.2% (range, 56.3–63.4%) of patients as rule-out (see Supplementary Material Table S6). The pooled sensitivity for this algorithm was 98.9% (95% CI: 96.4–100; I2=77.5%) (Figure 3). The NPV’s of the individual studies varied from 99.1% to 100% (see Supplementary Material Figure S4). For completeness, the summary estimates of NPV, specificity and PPV are provided in Supplementary Material Figures S4–S6.
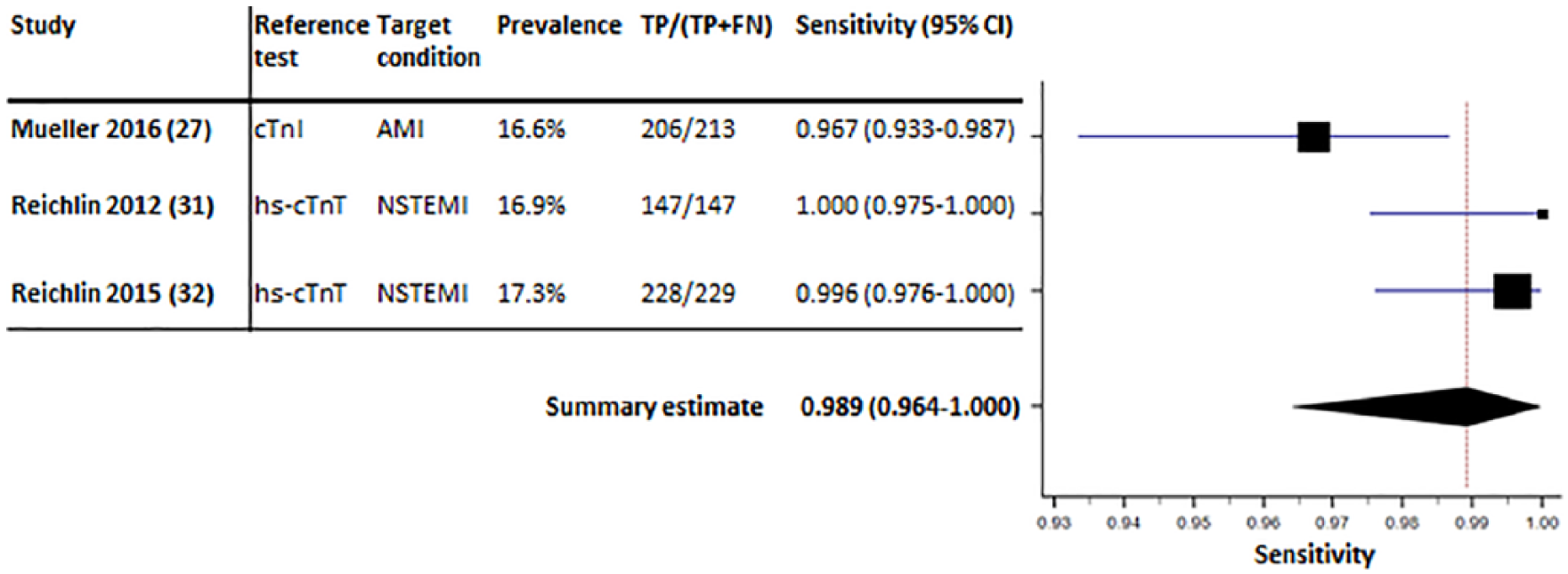
Forest plot displaying the summary estimate of sensitivity of high-sensitivity cardiac troponin T (hs-cTnT) <12 ng/l and Δ1 h<3 ng/l.
Single high baseline measurement of hs-cTnT for rule-in of AMI
Six out of 14 studies reported the specificity of a single high baseline measurement24,25,29,32,33,35 (Figure 4). The prevalence of AMI differed considerably between the studies, ranging from 3.6–24%. The pooled specificity of a high baseline hs-cTnT value was 94.6% (95% CI: 91.5–97.1; I2=95.5%). Sensitivity analysis, performed by removing the two studies that used cut-offs other than 50 ng/l, produced a pooled specificity of 95.2% (91.6–97.9%). The PPV’s of the individual studies varied from 28.3–86.5% (see Supplementary Material Figure S7). For completeness, the summary estimates of PPV, sensitivity and NPV are provided in Supplementary Material Figures S7–S9.
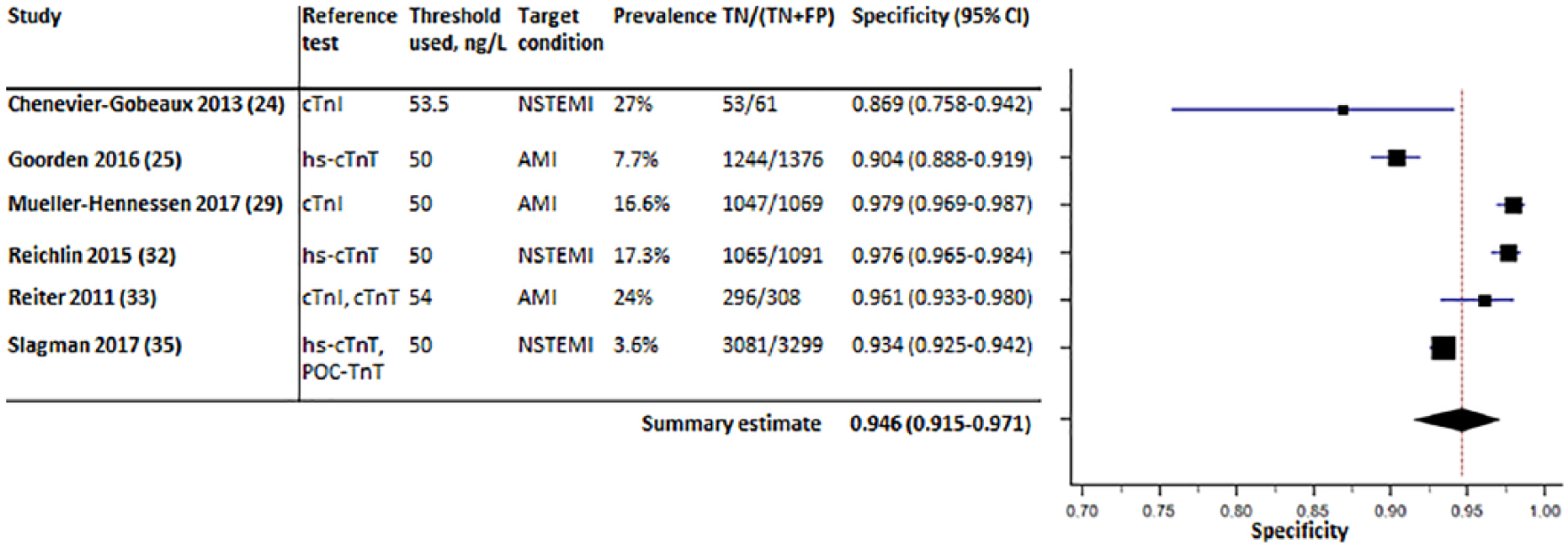
Forest plot displaying the summary estimate of specificity of a baseline high-sensitivity cardiac troponin T (hs-cTnT) value>50 ng/l.
Discussion
Novel cardiac biomarkers such as the hs-cTnT have become increasingly important in the diagnostic pathway and risk stratification of patients presenting with acute chest pain to the ED. They are a central part of clinical decision algorithms recommended by the current ESC guidelines. 5 The present systematic review and meta-analysis demonstrates that: (a) the two most frequently reported serial hs-cTnT measurement strategies have a high sensitivity to rule out AMI, while triaging a similarly large proportion of patients towards rule-out and (b) a direct rule-in strategy with a single baseline hs-cTnT value>50 ng/l has a high specificity.
Serial measurements for rule-out of AMI
Several meta-analyses have previously assessed the ability of a hs-cTnT assay to rule out AMI. Four articles examined a single baseline hs-cTnT measurement for rule-out of AMI at various diagnostic cut-offs.37–40 The 99th percentile was shown to have modest sensitivity for rule-out of AMI,37,39,40 however when the cut-off for rule-out of AMI was set below the limit of detection, i.e. <5 ng/l for the hs-cTnT assay, the sensitivities were generally high.38–40 It has been suggested that serial measurement of hs-cTnT is more accurate and informative than a single measurement for rule-out of AMI. As serial measurements provide information on rise and fall patterns, they are more informative for discrimination of acute from chronic myocardial injury. 19 A serial measurement strategy is particularly necessary in early presenters as they might have normal initial troponin values due to the time dependency of troponin release.41,42 A subgroup analysis performed by Mueller et al. showed that in early presenters (chest pain onset to presentation <2 h) the one-hour algorithm reached a NPV comparable to late presenters (chest pain onset to presentation ⩾2 h) to the emergency room. 27 Adding copeptin, a marker which is released very early after onset of symptoms, to hs-cTnT has also been suggested for early presenters in particular. 43 A recent meta-analysis by Shin et al. showed that adding copeptin to hs-cTnT improved the sensitivity for rule-out of AMI. 44
Our meta-analysis exclusively investigated the ability of the hs-cTnT assay to rule out AMI with the two most frequently reported serial measurement strategies. We found similar diagnostic accuracy for rule-out of AMI with serial high-sensitivity troponin measurements <99th percentile compared to the study by Lipinski et al. 37
Recently, Badertscher et al. directly compared the one-hour algorithm with the three-hour algorithm, which uses a fixed cut-off (the 99th percentile) at presentation and three hours in conjunction with clinical criteria (Global Registry of Acute Events (GRACE) score <140 and the requirement to be pain free). While both ESC recommended algorithms had comparable NPVs for rule-out, the one-hour algorithm allowed the rule-out of significantly more patients. 45 Contrastingly, the results of our study do not suggest a difference between the two rule-out strategies in the proportion of patients that are triaged towards rule-out. However, it is important to note that the serial measurement strategy with a fixed 99th percentile cut-off described in our study lacked the clinical criteria which are a key part of the ESC three-hour algorithm. 5
It is important to highlight that the majority of the studies, including the studies in this meta-analysis, have only examined the performance of the hs-cTnT assay in patients presenting with acute chest pain and free from major comorbidities. Few prospective studies have assessed the performance of this assay in lower-risk patients, e.g. women presenting with atypical symptoms, and higher-risk patients, e.g. patients with renal failure, to better reflect the cohort of patients in clinical practice. Biener et al. demonstrated that in patients presenting with atypical symptoms the sensitivity of a rule-out strategy with hs-cTnT was lower than in patients with typical chest pain. 22 Twerenbold et al. showed that in patients with renal failure a rule-out strategy based on hs-cTnT had a comparably high sensitivity and NPV to patients without renal failure, however they found that the efficacy of the strategy was substantially lower. 46 The underlying cause is the increased baseline troponin value in patients with renal failure, which decreases the possibility of a rule-out when using the same cut-off values. 47
Single high baseline measurement for rule-in of AMI
To our knowledge, this is the first systematic review and meta-analysis to report the specificity and PPV of a direct rule-in strategy with baseline hs-cTnT value>50 ng/l. The prevalence of AMI differed considerably between the studies; in the study by Slagman et al. the prevalence of AMI was 3.6%, whereas in the study by Reiter et al. the prevalence was 24%.33,35 The specificity of the direct rule-in strategy was consistently high between the individual studies. At the same time the PPV differed considerably; in studies with a low prevalence of AMI, we observed a lower PPV, which is in concordance with the theorem of Bayes. 48 We conclude that the applicability of a direct rule-in strategy with baseline hs-cTnT value>50 ng/l is highly dependent on the pre-test probability of disease and this stresses the importance of assessing the individual pre-test probability for clinicians. Patients with a low pre-test probability or a very atypical presentation might suffer from other conditions that also give rise to hs-cTnT. In such cases, serial hs-cTnT measurements can increase the probability of AMI when a rise and fall pattern is present. 49 If after serial sampling AMI is deemed unlikely, other causes of troponin elevations should be investigated as elevated troponins are associated with an unfavourable prognosis even in the absence of an AMI. 50
Recommendations for further research
The 2015 ESC one-hour algorithm has distinct cut-offs for ‘rule-out’ and ‘rule-in’ and patients not meeting these criteria are placed in the ‘observational zone’. This concerns a considerable number of patients (20–30%) who are known to have an unfavourable prognosis. 51 They are now faced with prolonged observational periods in the hospital, with or without invasive testing. Further research is needed to determine the optimal diagnostic approach. It has been suggested that advanced cardiac imaging may be useful for better risk stratification in these patients.52,53
Study limitations
Our study has several limitations. The studies included in the current analysis had different methods for adjudication of the final diagnosis. Some used conventional assays, whereas others used high-sensitivity assays for the reference standard. In addition, studies that used the same assay frequently had different cut-offs for adjudication of the final diagnosis. The use of high-sensitivity assays as opposed to conventional assays as the reference standard can influence the diagnostic accuracy parameters of the test being evaluated. Because of its higher sensitivity, the high-sensitivity assay detects more patients with myocardial injury not due to NSTEMI when compared to conventional assays. Moreover, we were not able to validate and examine the performance of the official ESC 0/1 hour algorithm for rule-out and rule-in, because of the limited number of distinct cohorts that were in studies with this algorithm. Due to lack of individual patient data and the limited number of studies we could not perform meta-regression or subgroup analysis to investigate the effects of certain patient and study characteristics, such as age, cardiac risk factors, target condition, time of chest pain onset to obtaining the first blood sample, assay used for reference standard and prevalence of AMI.
Conclusion
Serial hs-cTnT measurement strategies to rule out AMI perform well and can classify 60% of patients for rule-out, while a direct rule-in strategy with a baseline hs-cTnT value >50 ng/l has a high specificity.
Supplemental Material
ACC819421_supplementary_material – Supplemental material for Serial high-sensitivity cardiac troponin T measurements to rule out acute myocardial infarction and a single high baseline measurement for swift rule-in: A systematic review and meta-analysis
Supplemental material, ACC819421_supplementary_material for Serial high-sensitivity cardiac troponin T measurements to rule out acute myocardial infarction and a single high baseline measurement for swift rule-in: A systematic review and meta-analysis by M Arslan, A Dedic, E Boersma and EA Dubois in European Heart Journal: Acute Cardiovascular Care
Footnotes
Acknowledgements
The authors would like to thank Wichor Bramer (Biomedical Information Specialist, Erasmus MC) for his aid in the development and implementation of the search strategy.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This work was supported by a research grant from the Erasmus MC Thorax Foundation (project grant B4).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.