
Abstract
Electrical storm is characterised by a state of severe electrical instability that occurs in a rare combination of circumstances, and may lead to multiple implantable cardioverter defibrillator shocks and haemodynamic instability, and possible death. The main goal of treating electrical storm is to eliminate the trigger and modify the substrate of the arrhythmia. The aim of this educational review is to provide information for a better understanding of the underlying mechanisms and therefore help to improve the treatment of electrical storm patients.
Introduction
Electrical storm is a state of electrical instability and is characterised by several episodes of ventricular tachycardia (VT) or ventricular fibrillation (VF). The implantable cardioverter defibrillator (ICD) can effectively terminate ventricular arrhythmia (VA); however, it will not eliminate or modify the trigger or substrate of electrical storm. 1 Electrical storm patients usually present as a severe medical emergency characterised by multiple ICD shocks and haemodynamic instability. Because of the infrequent nature and unpredictability of electrical storm associated with a potential lethal outcome many physicians feel uncertain in the acute setting.
Mortality in the early and subacute phase is high.2,3 Several factors are associated with a negative outcome in electrical storm patients: severely impaired left ventricular ejection fraction (LVEF), 4 pre-existing advanced New York Heart Association class, cardiogenic shock 5 and older age.
Electrical storm can be a distressing experience for patients and their families, leading to significant psychological consequences. Effective management of electrical storm is crucial, and a collaborative hospital network with a dedicated electrical storm team has been suggested as beneficial.6,7 Treatment of electrical storm can be very complex and consists of the administration of anti-arrhythmic drugs (AADs), suppression of sympathetic tone, device re-programming and sometimes urgent catheter ablation (Table 1).
Definition of electrical storm: diversity in the literature
The clinical syndrome of electrical storm has been defined empirically. In the past a variety of definitions were used. In those early definitions the VT episodes ranged between two and 20 within 24 hours.5,8 At present, in the era of ICDs the most commonly accepted definition is three or more separate arrhythmia episodes leading to ICD therapy occurring over a single 24-hour time period. 9 The episodes of VT must be separate, meaning that the persistence of VT following unsuccessful ICD therapy is not considered as a second episode. 10 Incessant VT is a condition in which a sustained VT resumes within 5 minutes after successful ICD therapy and continues for over 12 hours. No study to date has determined a certain threshold burden of ICD therapy that begins to confer an adverse outcome.
Mechanisms underlying electrical storm
Crucial for the occurrence of electrical storm is an interplay between the autonomic nervous system, cellular milieu and a predisposing electrophysiological substrate. Both the trigger and the substrate may change over time influenced by the progression of scarring, left ventricular remodelling and the progression of heart failure. The critical role of an increased activation of the sympathetic nervous system in initiating and maintaining electrical storm is demonstrated in electrical storm patients who have exacerbation of heart failure. 11
Electrical storm: disease or symptom
Although electrical storm directly affects the patients’ prognosis, by preventing the next episode of electrical storm the mortality does not necessarily decrease. 12 Electrical storm often represents part of the natural history of advanced cardiac disease and may predict a serious deterioration in the underlying processes. It can even be debated if electrical storm is a marker for mortality in the near future and accordingly functions as a major bystander. This raises the question of whether all electrical storm patients would be potential candidates for catheter ablation. It is also a valid question as to whether a severe disbalance in the cellular milieu could outweigh a modification of the substrate? At the other end of the spectrum is those presenting with a first episode of electrical storm, who may benefit much more from a catheter ablation intervention and have a possible survival benefit. 13 Therefore, every patient that presents with even a single ICD shock should be considered as a possible electrical storm, whereas it may be preceded by multiple episodes of VT successfully treated by antitachycardia pacing (ATP).
Treatment of electrical storm: corresponding to the mechanism and trigger
Searching for and correction of reversible factors
In the majority of cases, no clear cause for electrical storm can be identified. Triggers such as electrolyte imbalance, acute ischaemia, exacerbation of heart failure, adjustment of or non-compliance to anti-arrhythmic medication 1 and recent introduction to biventricular pacing have been identified. 14 They should be actively searched for and promptly corrected in each electrical storm patient. Flow limiting coronary artery disease and volume overload should be adequately treated. Decreased left ventricular wall stress can be achieved with non-invasive and invasive haemodynamic support including a left ventricular assist device (LVAD), venoarterial extracorporeal membrane oxygenation (ECMO) and continuous flow percutaneous ventricular assist devices. Fever is a more rare trigger of electrical storm, and is especially important in patients with Brugada syndrome, in whom unsuppressed fever may lead to medically resistant incessant polymorphic and possibly fatal VT. 15
Device programming
Shocks delivered for self-limiting haemodynamically tolerable arrhythmias ought to be avoided.
Detection time can be prolonged and ATP can be given as an initial therapy. 16 Augmentation of ATP attempts, when feasible, is encouraged especially when shown previously to be successful. 17 During an electrical storm an effort should be made to avoid further conscious shocks, 18 and temporary disabling of shock therapy may be considered.
Anti-arrhythmic drugs
Frequently, the first step in the treatment of electrical storm is the administration of beta-blockers. Beta-blockers play a fundamental role in the management of electrical storm by blocking the sympathetic system. Adding beta-blockers intravenously in electrical storm patients already on oral beta-blocker therapy may help to keep an electrical storm episode under control. 19 Propranolol, a lipophilic unselective beta-blocker that penetrates the central nervous system, has been demonstrated to be effective in suppressing VAs as compared to metoprolol and amiodarone. 20 In the presence of structural heart disease amiodarone is one of the most frequently used drugs for the treatment of electrical storm. Procainamide, a class 1C AAD, has demonstrated its superiority compared to amiodarone for the treatment of haemodynamically tolerated monomorphic VT in the PROCAMIO trial. 21 However, it has been investigated only in patients without manifest heart failure and without severely depressed LVEF, in whom it is considered safe. The incidence of IV-amiodarone-refractory electrical storm is approximately 30%. IV-amiodarone-refractory VT storms are frequently induced by triggering premature ventricular contractions (PVCs) with a narrow QRS complex, 22 and may be successfully suppressed with additional administration of mexiletine, a class 1B AAD. 23 Reperfusion often leads to the development of automaticity or delayed afterdepolarisations originating from the Purkinje network, 24 which in fact is sodium channel mediated. 25 Lidocaine, a class 1B AAD is used in the setting of acute ischaemia. 26
There is no consensus on the optimal drug treatment for refractory malignant VA, and AADs may be given in a manner of trial and error. Drug combinations are sometimes necessary to alter electrical instability. AADs carry the risk of decreasing the cycle length of re-entry VAs and make VT more stable, which may precipitate to incessant VT. AADs should be given individually, taking into account not only the efficacy but also the increased risk of drug-related pro-arrhythmia and other side effects.
Overdrive pacing and sedation
Temporary (atrial) overdrive pacing may help to interrupt an incessant or re-occurring VA, especially in conditions such as Brugada and early repolarisation syndrome. 26 Overdrive pacing helps by preventing PVCs from occurring and reduces early afterdepolarisation. 27
As the sympathetic nervous system plays a major role in the initiation but also the maintenance of VAs, 11 sedation and/or intubation may be needed in order to suppress the sympathetic tone. A complete sympathetic blockade can be performed by left cardiac sympathetic denervation. 28
Radiofrequency catheter ablation
In the majority of electrical storm patients the episodes are characterised by a monomorphic VT based on re-entry. Therefore catheter ablation, targeting the substrate in which re-entry has formed, is an important treatment option for electrical storm.
Learning objective.
AAD: anti-arrhythmic drug; ICD: implantable cardioverter defibrillator.
In a pooled meta-analysis 29 of 471 electrical storm patients who underwent catheter ablation, catheter ablation had a high success rate with a low rate of recurrent electrical storm. Acute procedural success was 72% and procedural failure was 9%. During a follow-up of 15 months, 60% of patients were free of VA recurrences and 94% were free of electrical storm. Since then ablation of VT has evolved, and new approaches and technologies, such as the substrate approach, 30 remote magnetic navigation, 31 and a combined endo-epicardial substrate ablation, 32 have improved the outcome of VT ablation (Table 2). 33
Outcome of ventricular tachycardia ablation in electrical storm patients.
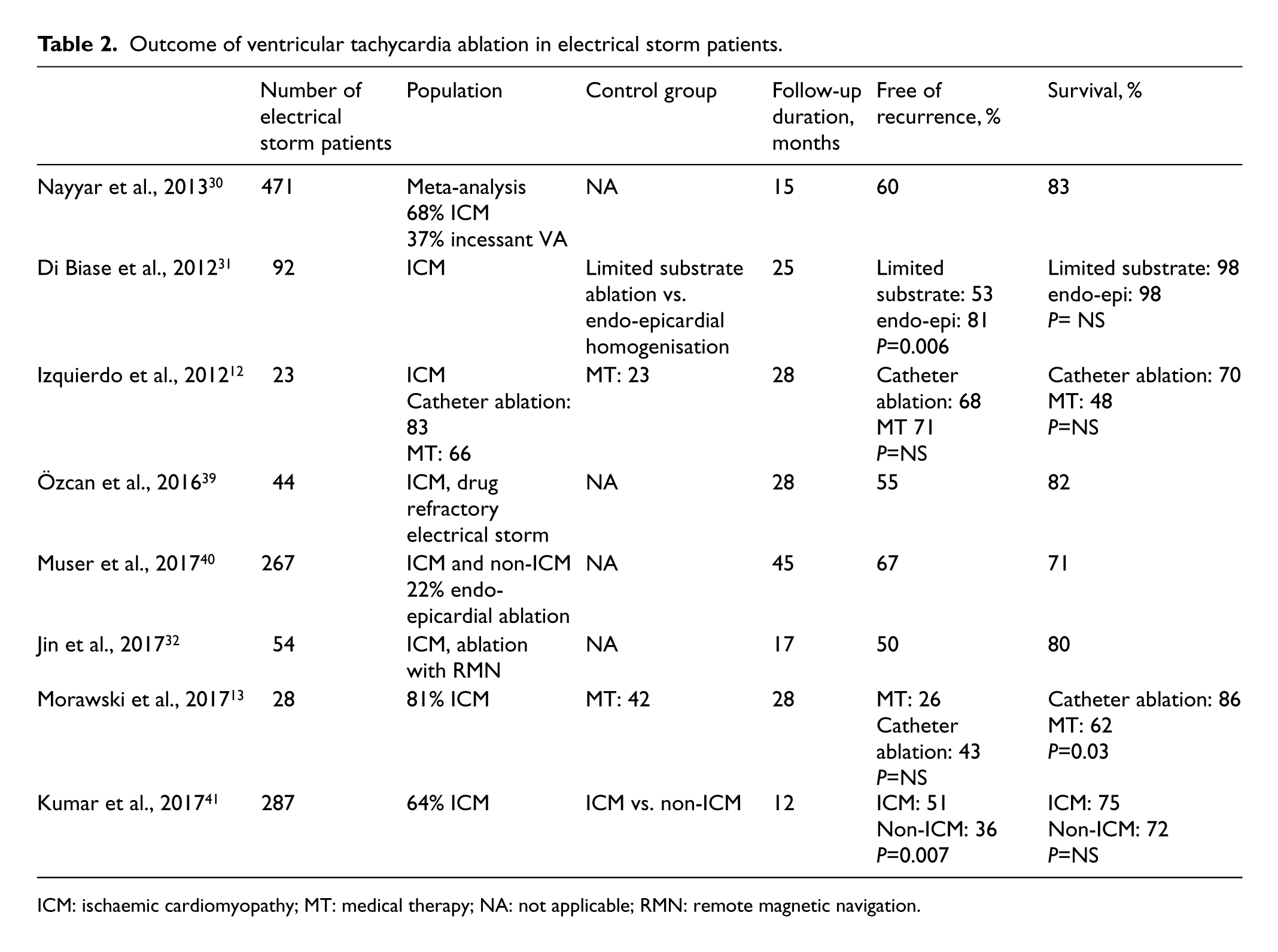
ICM: ischaemic cardiomyopathy; MT: medical therapy; NA: not applicable; RMN: remote magnetic navigation.
There is also a role for catheter ablation in patients who suffer from recurrent VF episodes. In 29 patients with ischaemic heart disease, recurrent VF was triggered by monomorphic ventricular extrasystole that originated from the fibrous peri-infarction zone. In eight patients with drug refractory electrical storm, ablation of the ventricular extrasystole was successfully performed, and control of electrical storm was achieved. 34
Compared to medical therapy catheter ablation reduces the number of subsequent VT episodes especially when VT ablation is performed within one month of electrical storm. 35 VT ablation in patients with a LVEF of 25% or greater is shown most beneficial. 12 Freedom from recurrent VT after catheter ablation has been associated with an improved survival.13,36 Morawski et al. 13 showed that in a first time electrical storm population, VT ablation was significantly more effective than any other form of therapy in reducing death at any time, even though the recurrence rate was not lower in the catheter ablation group. Yet, it is also known that patients with electrical storm have an increased risk of non-cardiac death. In other studies a mortality benefit from VT ablation in electrical storm patients was not shown. 12 This underlines the importance of the selection of patients as potential candidates for ablation.
The timing of catheter ablation, the approach and support should be tailored. Patients with incessant drug refractory VT who fail on haemodynamic support can benefit from a rescue VT ablation. 37 Patients with advanced heart failure and unstable VTs are at highest risk of haemodynamic collapse during the ablation procedure; they can benefit from mechanical support during catheter ablation. 38 Alternatively, the ablation can be confined to a substrate approach only. Consequent fluid overload related to irrigated catheter ablation may precipitate acute decompensation, 39 and preventive measures such as LVAD or ECMO may still be indicated in patients with severely depressed left ventricular function. In a small proportion of patients there is such a limited reserve in cardiac output that limited ablation should be aimed for, targeting only the critical isthmus of the clinical VT.
Conclusion
Electrical storm is a critical condition and even after successful catheter ablation patients continue to bear an increased burden of morbidity and mortality. Early recognition and referral to a tertiary electrophysiology centre is mandatory. Electrical storm should be treated by a team that offers a structured and tailored approach.
Key points
Early recognition of electrical storm and referral to a tertiary electrophysiology centre is mandatory.
Electrical storm should be treated by an experienced team that offers a structured and tailored approach.
An increased activation of the sympathetic nervous system is critical in the initiation and maintenance of electrical storm.
Electrical storm often represents part of the natural history of advanced cardiac disease and may be a predictor of serious deterioration of the underlying disease.
By treating electrical storm we attempt to eliminate the trigger and modify the substrate of the ventricular arrhythmia.
Treatment of electrical storm is complex and consists of the administration of anti-arrhythmic drugs, suppression of sympathetic tone, device re-programming and catheter ablation.
Anti-arrhythmic drugs should be given individually, taking into account not only the efficacy but also an increased risk of drug-related pro-arrhythmia and other side effects.
Electrical storm is a critical condition and even after successful catheter ablation patients continue to bear an increased risk of morbidity and mortality.
Footnotes
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.