
Abstract
In today's world, high variability of body mass index (BMI) is known as a significant global health problem that can lead to many negative impacts on the cardiovascular system, including atrial fibrillation (AF) and coronary heart disease. The current systematic review aims to elucidate the effect of variability in BMI on the risk of cardiovascular outcomes. Four databases, including PubMed, Scopus, MEDLINE, and CENTRAL, were searched. All related articles up to 10 June 2022, were obtained. Titles, abstracts, and full texts were reviewed. After screening abstracts and full texts, four articles were included in our study. In these four cohort studies, 7,038,873 participants from the USA and South Korea were involved. These articles generally considered the BMI and outcomes including cardiovascular disease, AF, and coronary heart disease. All these articles reported an association between the variability of BMI and increased risk of cardiovascular outcomes. Due to the negative impact of the high variability of BMI on the risk of cardiovascular outcomes, health policymakers and practitioners should pay more attention to the significant role of BMI in health problems and physicians might better check the variability of BMI visits to visit.
Introduction
High body mass index (BMI) and weight gain are acknowledged as primary global epidemic health problems and are associated with an increasing prevalence of hypertension, diabetes, and cardiovascular and cerebrovascular diseases. 1 The health complications of obesity are the results of two factors: the heightened mass of adipose tissue and the raised secretion of pathogenetic products from enlarged fat cells. Moreover, high BMI is associated with an increasing prevalence of hypertension which is the chief cause of cardiovascular mortality and disability in Western countries.1,2 In 2017, the number of patients with cardiovascular diseases (CVDs) reached a record 485 million worldwide, resulting in 17.8 million deaths, therefore placing a heavy burden on the global medical system. 1 Weight loss is commonly recommended in obese patients as one of the primary measures for preventing and treating hypertension, diabetes, improvement of blood lipids, reduction in blood glucose, and CVD. However, weight loss is very often followed by weight gain, which is commonly called “weight cycling,” which results in BMI variability and fluctuations.3,4 Whether such fluctuations and variabilities in BMI are associated with a good or a worse prognosis in cardiovascular outcomes remains controversial. 5 The Framingham study was one of the first studies to show that subjects with higher body weight variability compared with those with low body weight variability had a significantly higher risk of developing CVDs. 6 Other studies also showed that variability in BMI and body weight is associated with a higher risk of mortality and cardiovascular events in coronary disease and diabetes mellitus patients.6,7
Although there are systematic reviews that study the association of BMI with cardiovascular outcomes and mortality, to our knowledge no studies have explored the associations of variability in BMI with cardiovascular outcomes as a systematic review. In this study, we conducted a systematic review to estimate the association of variability in BMI with cardiovascular outcomes in the general population.
Research design and methods
Registration of review protocol
The protocol for this systematic review was registered and is visible in the Open Science Framework.
Data sources and searches
Included and excluded studies were collected following the Preferred Reporting Items for Systematic Reviews (PRISMA) flow diagram (Figure 1).
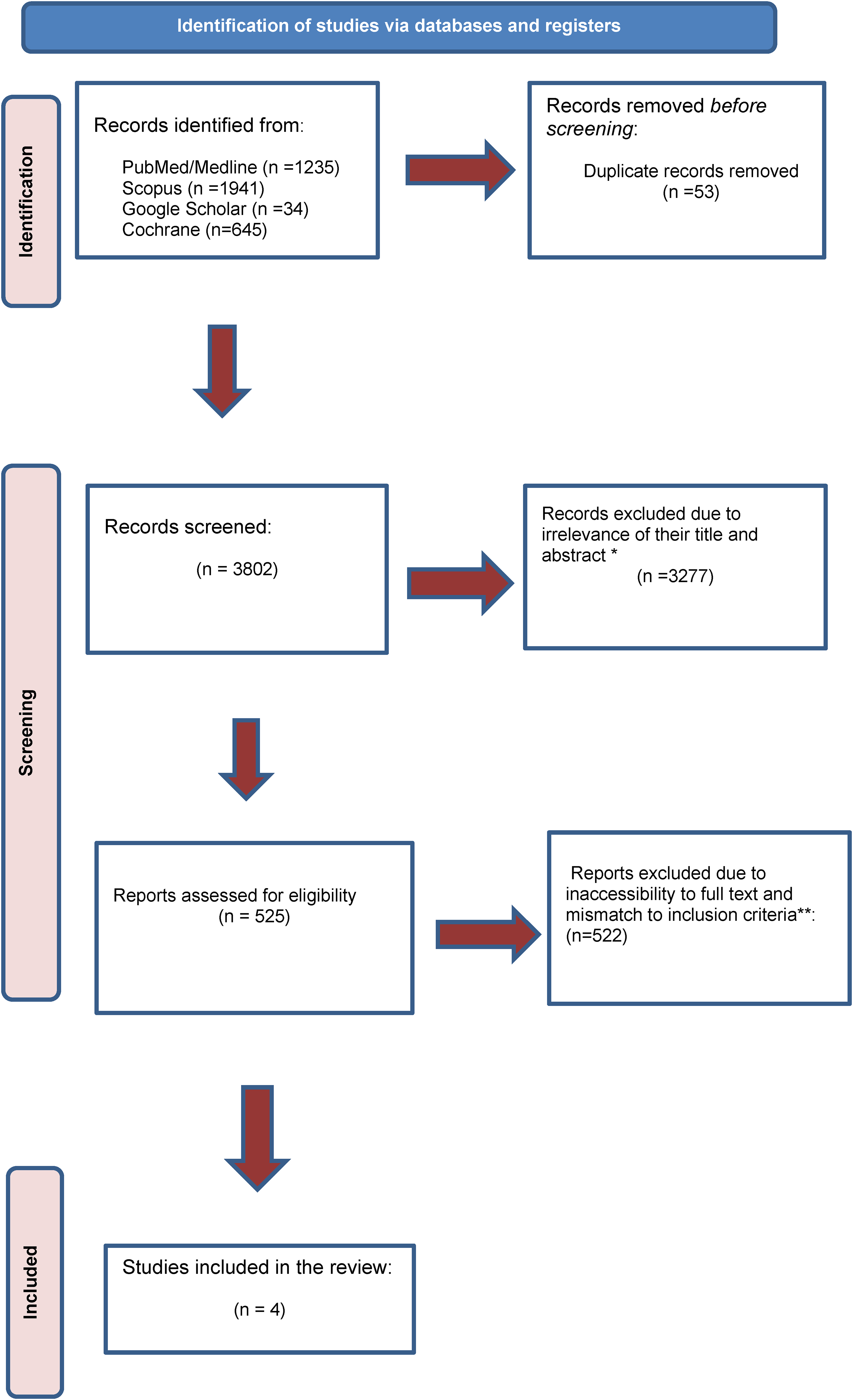
Preferred Reporting Items for Systematic Reviews (PRISMA) flow diagram of the study. *They are (1) review article; (2) editorial; (3) not observational. ***Irrelevant outcome.
Search strategies are provided in Table 1. A complete search in the references of retrieved articles was performed by one of the authors to find all related articles. Reference lists of relevant articles and previous review articles were hand-searched for other relevant studies.
Search strategies for PubMed, Scopus, and CENTRAL databases.

EndNote 8X software was used to manage retrieved references. Duplicate articles were removed. The screening was initially conducted by titles and then abstracted by two of the authors separately. Afterward, the full text of the articles was evaluated by two independent reviewers. The articles were studied and determined whether they met inclusion criteria. Discrepancies were resolved at first by consensus, and then were referred back to the original article, in consultation with a third author.
Eligibility criteria
The cohort studies that reported the association of variability in BMI with subsequent cardiovascular outcomes in the general population with a minimum follow-up duration of 4 years were included in this systematic review. Study participants included both sexes with no limitations in terms of comorbidities and ethnicity. Language restrictions were not applied either. Any definition of weight variability (i.e. variability independent of the mean (VIM), average successive variability, average real variability (ARV), coefficients of variation (CV)) was considered. The exclusion criteria of this systematic review were as follows: (1) any studies except for cohort study (i.e. reviews, editorials, abstracts, case reports, practice guidelines, in vivo, in vitro, and randomized control trial studies); (2) studies conducted on other population than the general population or patients with diabetes; (3) studies that demonstrated variability in BMI was a result of surgery or medications.
Data extraction and quality assessment
For all studies, we extracted information on study characteristics, type of study, follow-up duration, population characteristics, type of exposure, exposure definition, assessment methods, outcome of interest, adjusted variables, and quality assessment score. Any disagreements or disputes between the two evaluators were settled by agreement, then by the third evaluator. This review has been registered on The Open Science Framework.
Two authors assessed the risk of bias independently. The JBI Critical appraisal tools (https://jbi.global/critical-appraisal-tools) were used to judge study quality for each type of study. We judged studies that received a score of one-half of the total score to be at low risk of bias, and studies that scored less than one-half of the total score to be at high risk and we eliminated them.
Results
After removing the duplicates, 3802 articles were screened and 525 of them were eligible based on the title and abstract. Finally, after checking the full text, four articles were eligible for entering the current study (Figure 1).
A total of four cohort studies involving 7,038,873 participants, in the USA 8 and, South-Korea9,10 were surveyed to measure BMI variables ARV, VIM, and CV. The follow-up duration is at least 5.3 years and at most 32 years. Outcomes included coronary heart disease, atrial fibrillation (AF), and hospitalization due to CVD (more than four outpatient visits per year, death within 30 days of the first diagnosis). Two of the studies examined AF, and both showed a generally negative impact of BMI variability on the risk of AF. In general, an increased risk was observed in the others although in, one of the studies in Q1, Q2, and Q3 BMI variability for AF, the significant risk was not observed (Table 2).
Summary of the included studies in the current systematic review.

ARV: average real variability; VIM: variability independent of the mean; CV: coefficients of variation; AF: atrial fibrillation; BMI: body mass index; OR: odds ratio; HR: hazard ratio; CI: confidence interval; RR: risk ratio; CHD: coronary heart disease.
Discussion
This systematic review was planned to determine the impact of BMI variability on related CVDs, and 7,038,873 participants from four cohort studies with a minimum of 5.3 years to a maximum of 32 years were selected. These studies showed that the risk of AF, especially in men compared to women, morbidity due to coronary heart diseases, and hospitalization due to CVD is significantly strong in patients with a history of BMI variability.
Obesity is a well-known significant risk factor for coronary heart disease, AF, and heart failure. The epidemiology of CVD risk factors is changing rapidly with the obesity pandemic. 11 Also, based on recent research on the fluctuation of BMI and CVDs, there is a peculiar relationship between them that affects the prognosis of patients with cardiac problems. Cho et al. revealed an association between BMI variability and cardiovascular outcomes. Their study showed BMI fluctuation found to be a significant risk factor among cardiovascular patients with all-cause. Furthermore, in contrast to the BMI loss, it showed mild weight gain, which is reflected by an increase in BMI, reducing all-cause mortality among cardiovascular and non-cardiovascular middle-aged adults. 12
Several reasons have been suggested to justify the association of BMI fluctuations with CVD. First, these studies claimed that weight changes were the cause of CVD, but the opposite may be true, meaning that CVDs could have caused weight fluctuations. However, these diseases did not cause overt symptoms when the weight changes were examined. 6 Weight fluctuations may be an indicator of the preclinical stages of some diseases, such as CVDs. 9 Second, systemic disease or general weakness can cause cardiovascular complications, and weight fluctuations may be due to these cases. 9 Third, overweight and obese people are prone to CVDs. These people go on weight loss diets, but due to the failure of these diets, they gain weight again, and the chance of cardiovascular complications is still high in them. 9 Therefore, weight fluctuations are mistakenly considered to cause these cardiovascular complications. At last, the various physiological mechanisms that discriminate between intentional and unintentional weight reduction may explain this somewhat perplexing observation. Unintentional weight reduction (caused by diseases linked to sarcopenia or another underlying disease) has been linked to greater mortality, while intentional weight loss is typically associated with good cardiovascular outcomes.13,14 These data indicate that the cause of unintentional weight fluctuations can lead to cardiovascular complications.
Among the included studies, AF was reported in two studies. AF is the most clinical arrhythmia; thus, appropriate management and detection are crucial due to its high morbidity and mortality. The study by Lee et al. 9 used the VIM to express the variability of BMI. Their study showed patients with the highest VIM quartile of BMI had an increased chance of AF compared to the lowest. Another study by Zhao et al. supports the mentioned findings, which linearly increased the risk of AF found to be in patients with higher BMI and waist circumference significantly. However, these factors’ variability was not associated with the risk of AF. 15 Although BMI is not a perfect predictive factor due to the inability to distinguish between muscle mass and body fat, there are several hypothetic mechanisms related to the variability of BMI and AF. First, adiposity, which BMI measures, is related to obstructive sleep apnea, 16 risk of hypertension, 17 diabetes, 18 heart failure, 19 left ventricular hypertrophy, 20 and coronary heart disease, 20 which are confirmed risk factors for AF. Also, Dewland et al. demonstrated the impact of low-grade inflammation due to adiposity, strongly related to AF, which could be another mechanism of BMI's impact on cardiovascular events. 21 In another included study, Huxley et al. found that weight change and its association with AF were related. 8 Their study revealed that men were substantially more affected by weight change than women; those who gained >10% body weight compared to 5% weight gain had a 61% larger risk of AF than women, who had a 19% greater risk. The significant rise in incident AF among people who lost more than 5% of their original body weight during follow-up is intriguing.
Diabetes, similar to the up and down of BMI, is a well-known risk factor for cardiovascular events. The combination of these major risk factors was discussed in the Youk et al. study, which is based on the concept of the Framingham study in 1960. 10 Their study showed the OR in the group of diabetic individuals with high BMI variability was 1.51 (95% CI 1.04 to 2.20), which markedly elevated the risk of CVD compared to the group with low variability. Also, the incidence of cardiovascular illnesses was unaffected by BMI variations in non-diabetic patients. Similar to this result, another study reported a similar effect that patients with type 2 diabetes who experience weight gain or reduction over 18 months, particularly if the change is <5%, may be at risk for developing negative cardiovascular consequences. 20 The controversy over the impact of weight or BMI change was discussed in another study too. The study by Doehner et al. showed that those who were overweight or obese and had Type 2 Diabetes Mellitus and cardiovascular co-morbidity died less frequently than patients who were of normal weight. In addition, increased mortality and morbidity were associated with weight loss but not weight gain.22,23
According to reports from Lim et al. in particular populations, metabolic variability parameters—such as glucose-CV, triglyceride CV, systolic blood pressure variability CV, and total cholesterol CV—are significant risk factors for cardiovascular events in diabetic patients, regardless of their corresponding mean values. Future research must clarify the precise mechanisms by which the variability of several parameters influences one another. 24
The large prospective cohort of patients with stable congestive heart failure studied by Held et al. did not support the overweight paradox for cardiovascular clinical outcomes. Following multivariable corrections, a U-shaped curve represented the relationship between BMI and the risk of cardiovascular and overall death, as well as hospitalization for heart failure. Notably, people with a BMI of about 27 kg/m2 had the lowest risk, which is a little higher than what is presently advised in preventive guidelines. Both patients with very high BMI and those with very low BMI showed the highest risk, suggesting that there is a particular high-risk category of people. It is advised to pay close attention to these extreme groups in order to identify the underlying pathology and improve treatment. The explanations for these variations could vary. 25
These controversial findings are still unclear due to the lack of specific studies on these crucial topics. To achieve higher certainty, a number of shortcomings in the study must be fixed in subsequent evaluations. There were not many publications that fulfilled the eligibility requirements overall, based on our review of the body of current literature. Because we limited our research to open-access journals, the overall amount of publicly available evidence was also reduced, which may have had an impact on this investigation. More large cohort designs with greater quality and longer length are needed in order to investigate this topic more confidently and precisely. Furthermore, extensive studies with the lowest bias and long-time follow-up are needed because of limited available data.
Conclusion
Altogether, the impact of BMI fluctuation on cardiovascular outcomes was discussed in this study. This systematic review of current evidence showed a negative impact of BMI variability on cardiovascular outcomes such as AF, morbidity due to coronary heart diseases, and hospitalization due to CVD among the general population and diabetic patients, so a clear awareness of weight change in a protocol of diet therapy could prevent future major adverse effects. Healthcare providers should recommend a stable weight to their patients and other people in society and pay more attention to the changes in patients’ weight.
Footnotes
Acknowledgement
The authors would like to thank the researchers whose work was included in this study.
Authors’ contribution
Study concept and design: Niloofar Deravi. Acquisition of data: Kimia Kazemzadeh, Mohammadreza Saleh, Alireza Niazi, and Mahnaz Bakhshi Mohebbi. Drafting of the manuscript: Mohammad Ali Esfandiari, Akram Ansari, Goharsharieh Alishiri, Amir Abdi, Rozhina Tamannaeifar, Shaghayegh Afshari, Sepand Daliri, Sahar Balanian, Fatemeh Vosoughian, and Elaheh Foroughi. Critical revision of the manuscript: Niloofar Deravi. Study supervision: Niloofar Deravi
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Guarantor of the study
Niloofar Deravi.