
Abstract
Cardiovascular disease remains a substantial concern in terms of global mortality and morbidity, while prevalence of cardiovascular disease is increasing as treatment modalities improve survival. With an ageing population and increasing costs of chronic medical care, primary prevention of cardiovascular disease is an important target for healthcare providers. Since the previous iteration of this paper, new international guidelines have been produced regarding hypertension and lipid lowering therapies, whilst there is a growing body of evidence and new therapies emerging in other areas of lifestyle and pharmacotherapeutic intervention. This review outlines emerging evidence in the field and compares and contrasts contemporary recommendations from European and American guidelines.
Introduction
Cardiovascular disease (CVD) describes coronary heart disease, cerebrovascular disease, peripheral arterial disease, rheumatic and congenital heart disease and venous thromboembolism. Collectively, CVD is responsible for 17.9 million deaths per year globally – 31% of all deaths, within which Ischaemic Heart disease (IHD) accounts for the majority of mortality. 1
Despite a fall in the proportion of CVD related deaths over the last 40 years, the rate of decline is slowing while morbidity from CVD is rising. 2 The financial implication of this on healthcare providers is substantial – it is estimated that CVD now costs NHS in the UK £9 billion a year 3 and €210 billion across the European Union in combined direct and indirect costs. 4
The ability to identify those at risk of CVD allows for risk factor modification through primary prevention. There are a number of factors that affect a person’s risk of developing CVD including increasing age, gender, family history and ethnicity which are non-modifiable. There are also a number of factors in terms of lifestyle and pharmacological interventions that have been demonstrated to affect CVD risk and are modifiable including hypertension, obesity, tobacco smoking, diet, exercise, cholesterol levels, alcohol intake and diabetes mellitus control. 5
Methods
Contemporary guidelines targeting primary prevention of cardiovascular disease (CVD) were reviewed from the European Society of Cardiology (ESC), European Society of Hypertension (ESH) and American Heart Association (AHA)/American College of Cardiologists (ACC).
In keeping with the previous review, common areas within these guidelines were noted and then a literature search was performed using the search terms Exercise, Diet, Weight, Weight loss, obesity, Smoking, tobacco, e-cigarette, electronic cigarette, alcohol, ethanol, lipids, cholesterol, HDL, LDL, triglycerides, hypertension, blood pressure, glucose, diabetes, polypill, anti-platelets.
Evidence regarding their effect on CVD was assessed then compared and contrasted, as were guidelines and evidence used by the above advisory bodies.
Discussion
Risk assessment
Modification of cardiovascular risk is predicated upon the understanding of underlying individual risk burden. Many of the interventions discussed below use risk stratification methods to guide their timing and intensity; as such, the use of validated risk assessment tools in primary prevention of CVD is vital and recognized in both European and American guidelines.
The ESC guidelines recommend the use of the SCORE risk assessment tool,6,7 whilst the ACC guidelines recommend the use of the updated atherosclerotic cardiovascular disease (ASCVD) risk assessment tool,8,9 both of which are available online as simple risk calculators for ease of use.
The reason for the discrepancy in terms of risk calculators is due to the validation of these tools in their intended cohorts; the ASCVD risk assessment tool was developed and validated using American patient datasets, whilst the SCORE risk chart was developed using European data and can be calibrated within Europe depending upon individual country’s mortality statistics.
Both guidelines advise consideration of alternate risk calculators in specific populations with altered CVD risks; the ASCVD calculator is intended and validated only for use in patients aged between 40–79, whilst the SCORE risk chart was similarly derived from patients aged <80, and the online version and is intended for use in patients aged 40–65.
There are now a variety of alternate risk assessment tools designed and validated for use in more narrowly defined population groups, including diabetic patients 10 and the elderly, 11 and it is important to remember to use the appropriate tool for the correct cohort.
These tools all deliver a quantitated measure of risk for the physician, commonly in the form of 10-year CVD risk, or 10-year CVD mortality. It is according to these quantitative risk estimates that we attempt to modify risk factors, and reduce the burden of CVD.
Lifestyle modification
Exercise
Exercise remains universally recommended for risk reduction of CVD, consistent with its positive effects for a wide variety of health conditions. 12
The most substantial reductions in major cardiovascular events are seen at commencement of exercise, with subsequent increases in level of exercise providing further benefit though diminishing returns are noted at upper extremes of exercise intensity. 13 There is limited evidence currently to support the hypothesis that extreme levels of exercise increase the risk of ASCVD however there is some evidence suggesting an increased risk of other cardiac conditions, in particular atrial fibrillation. 14 The evidence indicates that regular exercise is overwhelmingly beneficial for the general population where benefits substantially outweigh the risks. 15
Recommendations regarding exercise have largely remained unchanged since the first iteration of this review in 2017. The ESC recommend a combination of aerobic and strength exercise advised at least 150 minutes moderate-intensity or at least at 75 minutes of vigorous intensity aerobic exercise plus at least 2 muscle strengthening sessions a week.6,16 AHA/ACC advise physical activity to reduce blood pressure (BP) and non-HDL cholesterol - in particular they advise 3–4 40 minute sessions of moderate to vigorous exercise based on meta-analysis from 2001 onward. 17
The nature of the dose-response effect of exercise on cardiovascular risk reduction remains unclear which may account for the lack of contemporaneous guideline updates. 18 Current recommendations are predicated largely on reasonable expectations of exercise in the general population rather than specific ideal dosing. Further investigation is required to generate clear evidence-based goals for exercise. What is clear from the evidence is that exercise is one of the most powerful tools in primary prevention of CVD.
Diet
There is a large body of observational and epidemiological evidence that demonstrates changes in diet can reduce morbidity and mortality from CVD. However, the multifaceted nature of dietary modification means there is limited evidence in the form of RCTs. 2
The ESC recommends a diet low in saturated fats with a focus on wholegrain products, vegetables, fruit and fish as the dietary mainstay of CVD prevention. They advise abstinence from alcohol and sugar-sweetened drinks and adherence to a Mediterranean type diet. All such adjustments have been shown to significantly reduce CVD risk. 6
Clear evidence causally linking industrially produced transfats and CHD is reflected in the ESC guidance on avoidance of such foods – “the less the better”. 19
AHA guidance has been updated since this previous review and is now more in line with the ESC. The previously recommended DASH (Dietary Approaches to Stop Hypertension) diet is now not recommended as dairy intake was found to be associated with an increase in CV mortality rates when compared with vegetable protein, 20 it is no longer included in their recommendations. 8 AHA now recommend Mediterranean diets, coupled with increased nut, vegetable, legume, fruit, and lean vegetable or animal protein (preferably fish). This is based on consistent association of such diets with lower risk of all-cause mortality than control or standard diets found in observational studies. 8
As can be seen there is a general consensus between the recommendations but definitive answers are hindered by the logistical difficulty of conducting comprehensive RCTs in this field. As such these consensus statements are largely based upon old observational data and epidemiological evidence.
Weight
Obesity (Body mass index (BMI) ≥30) and being overweight (BMI ≥25) are associated with increased risk of CVD, whilst BMI 20–24.9 is associated with the lowest all-cause mortality. A BMI of ≥25 is directly related to increased risk of hypertension and type 2 diabetes mellitus which are themselves known risk factors for CVD. The corollary of this is that weight loss to maintain a BMI of 20–24.9 has been shown to reduce BP, improve glycaemic control and thus reduce other modifiable risk factors for ASCVD.21,22 It must be recognised thar BMI is an easy to use but imperfect tool. BMI is often used as a surrogate for waist circumference or other more direct measures of adiposity which is known to correlate negatively with CVD risk. 23 Particularly in athletic and muscle-bound individuals, an elevated BMI is unlikely to correlate well with underlying risk and this should be taken into account in patient risk assessment where appropriate. 24
Both AHA and ESC guidelines recommend maintenance of weight within the healthy range as described above, using a combination of balancing caloric intake in association with structured exercise programmes with activity based upon the guidance described above.
Smoking and E-cigarettes
Smoking remains one of the leading contributors to CVD worldwide. An estimated 1 billion people smoke worldwide 25 and 12% of deaths related to CVD are attributable to tobacco use. 26 There is no safe level of smoking and even passive smoking is known to increase CVD risk. 27 Stopping smoking is the most cost-effective intervention that one can make in primary prevention to reduce CVD risk. 6 As such, all guidelines recommend smoking cessation.
Pharmacotherapies such as nicotine replacement therapy (NRT) and Buproprion (a noradrenaline dopamine reuptake inhibitor) have been shown to help around 80% more people quit compared to placebo. Varenicline (a partial nicotine agonist) doubles the chance of abstinence 6 and earlier concerns regarding a possible link between varenicline and serious neuropsychiatric events appear to have been disproven. 28
A recent Cochrane review found increasing behavioural support as an adjunct to pharmacotherapy for smoking cessation was likely to increase the chance of success by 10–20% as compared to little or no behavioural support. 29
Electronic cigarettes (ECs) are battery powered devices which simulate smoking by heating nicotine amongst other chemicals in a vapour which is then inhaled. Long-term safety data remains sparse and inconclusive regarding ECs. The data available suggest that they are less cardiovasculopathic than traditional cigarettes, but there is still potential for increased CVD risk with their use. These effects are mediated by increases in inflammation, 30 platelet aggregation31,32 and arrhythmogenesis 33 amongst other pathways.
As such there is obviously concern about the risk to non-smokers but for current cigarette smokers switching from cigarettes to ECs appears a useful harm reduction strategy with a recent RCT demonstrating that this strategy outperforms NRT in achieving long-term smoking cessation. 34
The weight of evidence demonstrating causality between smoking and CVD leads both AHA and ESC guidelines to recommend firm support of smoking cessation. Further evidence on the utility or harms of ECs are still awaited and will influencing future guidelines.
Alcohol
There has been controversy regarding the purported benefit of light-moderate alcohol intake on CVD risk despite the plentiful evidence linking alcohol intake above current UK guideline limits and increased CVD risk. 35 There are epidemiological studies linking light-moderate drinking with reduced CVD risk 36 however Holmes et al. challenge this assumption in their 2017 meta-analysis. They found CVD risk profile to be significantly lower in those studied with a single nucleotide polymorphism in the alcohol dehydrogenase enzyme which predisposes the individual to consume less alcohol. They suggest the cardioprotective effects of alcohol found in previous observational studies may be due to selection or confounding biases. 37 The ESC specifically cite Holmes et al. in their justification for limiting alcohol intake with no safe recommended limit. 6 The AHA recommend a daily limit of 1 or 1–2 drinks/day for women and men respectively though the evidence appear to demonstrate that if there is any putative cardioprotective effect it is likely to occur at levels lower than this. 38
In summary there is a clear consensus regarding the negative effects of excessive alcohol intake but due to lack of clear evidence the guidelines are not concordant in regards to healthy levels of alcohol consumption.
Pharmacological therapies
Lipid-lowering therapy
Lipids are vital molecules for a variety of physiological processes including energy utilization, steroid hormone production and bile acid formation. Apolipoprotein-B containing lipoproteins <70 nm in diameter can cross endothelial walls where they can interact with extracellular matrix structures, ultimately leading to lipid deposition and atheromagenesis, the precursor to ASCVD. 39
A variety of data support the fact that levels of serum cholesterol and its lipoprotein carriers are linked causally to ASCVD. Epidemiological studies demonstrate that populations with lower total and non-High Density Lipoprotein cholesterol (non-HDLC) have lower levels of ASCVD, and that longer-term exposure to lower levels of non-HDLC in comparison to short-term exposure lead to reductions in the rate of ASCVD.40–42 In addition, RCTs of medications which lower cholesterol demonstrate marked reductions in ASCVD with no evidence of a J-shaped curve. 42
Elevated plasma levels of triglycerides are associated with higher rate of ASCVD. This effect can be ameliorated by pharmacologically reducing TG levels, though this appears to be mediated by linked changes in the concentration of TG-rich lipoproteins as estimated by non-HDLC. 39 Recommendations are made for other lipid groups, but it is noted that clinical trials have not clearly determined target levels for HDL-C or TG, however the evidence in favour of more aggressive reduction in LDL-C is increasing.
HDL-C levels are inversely associated with ASCVD and this is consistently seen through epidemiological studies, however RCTs have demonstrated no beneficial effect to raising HDL-C levels,43–45 neither in changing the progression of atherosclerosis nor rates of ASCVD. As such, neither the AHA/ACC nor ESC guidelines recommend target levels nor interventions for these molecules. Instead they suggest their use to help risk-stratify individual patients, particularly in those with iatrogenically lowered LDL-C as elevated Triglyceride, ApoB and lowered HDL-C levels can indicate persisting CVD risk.39,46
Since the previous review, guidelines have been updated from the AHA/ACC 46 as well as the ESC 47 regarding cholesterol management, and both advise lower serum cholesterol targets and new practices in the face of updated evidence and new therapeutic options – see Table 1 for a comparison between the two. Both ESC and AHA/ACC recommendations for intervention and ideal target serum cholesterol levels in primary prevention are predicated on risk assessment of the individual patient. This can be performed using a variety of available risk-stratification tools including the ESC recommended SCORE system 6 or QRISK3. 48

The differences between the two target groups are acknowledged explicitly in the ESC guidelines as not having been borne out by RCT evidence, and they note that they infer target levels from meta-analyses and mendelian analyses demonstrating the persistent reduction in ASCVD risk with lower LDL-C levels. 39 That said, these guideline targets remain consensus agreements rather than clearly defined and evidenced targets.
In order to achieve these targets, and subsequent to appropriate lifestyle interventions as described above, there are a variety of pharmacological tools recommended to achieve these targets. The long-term mainstay and first line therapy in both European and American guidelines for primary prevention remains statins which, since 2005, have been shown to be effective in reducing serum cholesterol with clear correlation between absolute reduction in LDL and reduction in risk of ACSVD; headline values include 20–25% reduction in Major Adverse Cardiovascular Events (MACE) and a 10% reduction in all-cause mortality over 5 years per 1 mmol/L reduction in LDL-C. 49
For those intolerant of statins, cholesterol absorption inhibitors such as Ezetimibe remain second line in ESC guidelines and are recommended for use in addition to statins when target values cannot be achieved due to good evidence for an additive effect on top of maximally tolerated statins. ESC guidelines also recommend their use as monotherapy where statins cannot be tolerated due to inferences made from their use as additional therapy on top of statin use,50,51 but there is little good RCT evidence backing this statement 52 and their use is omitted from the ACC/AHA guidelines entirely.
Discussed as a novel therapy in the previous iteration, 53 Proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors have been shown to significantly and substantially reduce LDL-C levels and cardiovascular risk as part of secondary prevention in high risk individuals,54,55 and have, in part, driven some of the narrative regarding even lower target serum LDL-C levels. Their use has, however, as yet only been recommended for primary prevention in patients with significantly elevated risk such as due to familial hypercholesterolaemia due to the lack of good quality and longer-term outcome data for their use in primary prevention groups. The effect of cholesterol reduction is typically seen over longer time periods so with further longitudinal data, and perhaps changes in drug price, their inclusion in primary prevention recommendations is something that could change between the current and subsequent guidelines.
In a similar vein, Inclisiran is a novel medication designed to interfere with translation of PCSK9. Phase three trials are still to be reported for its use in familial hypercholesterolaemia but initial results demonstrate a substantial and significant LDL-C reduction in these patients. 56 Currently there is no data for their use in primary prevention but this is a treatment modality which may expand in subsequent years with greater data from the primary prevention group and longitudinal data within the secondary prevention and extremely high-risk populations.
Whilst LDL-C reduction remains of clear benefit in elderly patients with known ASCVD, there remains real argument about the purpose and benefit of cholesterol reduction in primary prevention. In those above 75 years it appears that in otherwise low-risk individuals there is little evidence to support clear individual benefit, and in even high-risk groups at older ages this evidence appears to disappear entirely as seen in both retrospective cohort studies and prospective RCTs.57–60 The recent Cholesterol Treatment Trialists meta-analysis does little to dispel this, noting that in the primary prevention group ‘…there is less direct evidence of benefit among patients older than 75 years’. 61 The ongoing STAREE study was designed specifically to address this question; it looks at the effect of Atorvastatin use in those >70 years who are otherwise well, particularly with no evidence of CVD, diabetes, kidney or liver disease and is due to report in 2023. 62 Until then, in this age group it appears even more pertinent to discuss with the individual patient the risk-benefit profiles and their wishes when considering LDL-C lowering therapies.
Hypertension
Hypertension remains recognised as one of the foremost contributors to cardiovascular risk with recent studies naming it as the leading contributor to global premature death 63 and accounting for more CVD death than any other modifiable risk factor in the United States. 64 Meta analyses have demonstrated significant and substantial CVD risk reduction with reductions in systolic blood pressure (SBP); Lewington et al. demonstrated a doubling of CVD risk with each SBP increase of 20 mmHg and DBP increase of 10 mmHg in patients with BP from <115 to ≥180mmHg 65 and this continuous linear reaction has been demonstrated in all ages 66 and ethnic groups.67,68
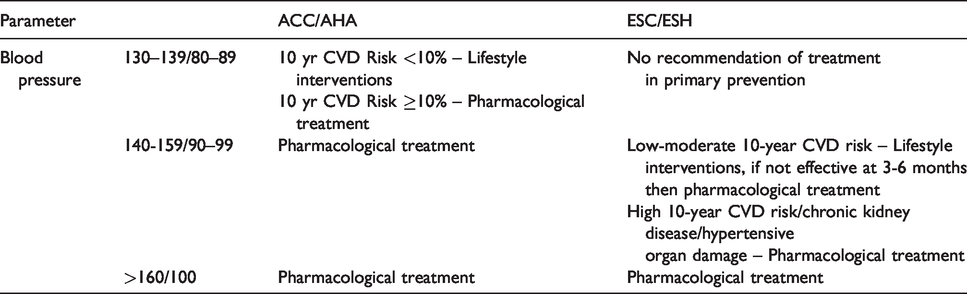
There now exists notable agreement between European and American guidelines in terms of how to diagnose and management of hypertension, while there are some discrepancies in terms of treatment cut-off values and target BPs69,70 – please see Table 2 for a comparison between the two.
Diagnosis and monitoring of BP are recommended via repeated automated office BP measurement, ambulatory or home BP monitoring. Home and ambulatory blood pressure monitoring has been shown to be better correlated with hypertensive end organ damage and can aid in the reduction of overtreatment of ‘white-coat’ hypertension.71,72 Using the results of these BP measurements, both guidelines recommend the use of CVD risk calculators as described above to assess the need for, and intensity of antihypertensive therapy.
In terms of when to treat, European and American guidelines are in agreement in the upper ranges of BPs; with BPs of >160/100 both guidelines recommend treatment with pharmacological intervention. Both guidelines cite the proven benefits of anti-hypertensive therapies in moderate to high risk patients with SBP >130mmHg and DBP >80mmHg73,74 and in any patient with severe hypertension (SBP ≥180/DBP ≥110), the latter in whom intervention has been demonstrated to be clearly beneficial irrespective of assessed CVD risk. 75
The main discrepancy between the two occurs at lower levels of BP. At BPs of 130–139/80–89 the ESC/ESH guidelines recommend lifestyle interventions (as discussed above), and consideration of pharmacological management only in high risk patients with pre-existing CVD, particularly coronary artery disease.
In contrast, the ACC/AHA recommend stratifying these patients using a risk calculator, and pharmacologically intervening in those with a risk of ≥10% over 10 years, whilst encouraging lifestyle interventions if <10%.
Anti-hypertensive therapy is not considered for all patients at these lower targets due to the absence of evidence supporting its use76,77; taking CVD risk into account allows for targeting of those patients in whom there is likely to be a clear clinical benefit and good relative risk reduction.
Moving to BPs of 140–159/90–99 the ESC guidelines recommend initial attempts at lifestyle management in patients with low-moderate CVD risk before a move to pharmacological therapy if these are not adequate at 3–6 months. For those at high risk, or with pre-existing chronic kidney disease or hypertension mediated organ damage they recommend immediate pharmacological therapy, while the ACC/AHA recommend pharmacological intervention for all patients with BP >140/90.
The discrepancies at lower levels of BP are not insignificant in terms of their impact on the target population. In America this change of definition suddenly medicalizes a significant proportion of the population with a potential impact on the cost of healthcare as a result of increased insurance premiums.
The discrepancy between the recommended timing of pharmacological treatment stems from assessment of the relative benefit of intervening at lower levels. Changes to the recent ACC/AHA guidelines cite meta analyses, and particularly data from the Systolic Blood Pressure Intervention Trial (SPRINT) which demonstrate CVD risk reduction when treating lower levels of BP, whilst the ESC/ESH group consider the gains in CVD risk reduction made by intervening at these lower levels to be marginal with a corollary increase in adverse events as evidenced by the same trial. 78 In addition, while the American guidelines cite the evidence of increased relative risk between SBP of <120 to 130–139, the European guidelines point to the lack of evidence of risk reduction when treating those with BP <140. In addition, a noteworthy criticism of the SPRINT trial is that it includes patients with a baseline BP of 130–139 in its data analysis despite these patients already being on antihypertensive treatment. As such, the medical conservative can argue that the results of the trial cannot be extrapolated to untreated patients with similar BPs.
Both groups agree that the use of CVD risk calculators should aid targeting of treatment to those with highest risk, but the discrepancy in treatment thresholds appears largely a question of consensus opinion on risk/benefit of therapy at lower levels and the perceived merits or disadvantages of medical conservatism.
In terms of target BPs there has been a suggestion of a J-shaped curve in CVD events from observational trials65,79,80 but there are significant concerns over confounding variables and no clear data supporting this from RCTs. 81 Physiologically there must be a suboptimal arterial pressure at which systemic perfusion becomes compromised but this level remains unsatisfactorily delineated. Meta-analysis suggests that more aggressive SBP and DBP lowering leads to further reduction in CVD events, 82 whilst current target levels are largely based upon evidence from the SPRINT trial which demonstrated an increased rate of hypotensive side-effects when intensive SBP targets of <120 were set in comparison to <140. 78 The ESC-CHL-SHOT trial was designed in part to further clarify this issue but is yet to complete and its data are eagerly awaited. 83
The difference of risk/benefit priorities is again seen in the approach to BP targeting in the elderly patient; the ESC suggest higher target BPs of <140/90 to offset an increased rate of adverse effects seen when pursuing lower BP targets in the elderly, whilst the AHA recommend lower targets of <130/90 due to the perceived cardiovascular benefit accrued in this population. Again, it appears pertinent here to consider the concerns and wishes of the individual patient when applying these recommendations.
Both guidelines agree on the use of combination therapy in patients with BP ≥20/10 mmHg above their SBP target due to the strong and uncontroversial evidence of the synergistic effect of anti-hypertensive therapies as demonstrated by Wald et al. 84
The continued recommendation of beta-blockade as an anti-hypertensive agent in European guidelines remains a point of contention, with the American guidelines contending that a 2017 Cochrane review demonstrates that there is no evidence of risk reduction secondary to their use. 85 They do note their potential utility in certain patients, specifically those with comorbid conditions that may benefit from its use, such as heart failure with reduced ejection fraction or ischaemic heart disease. Otherwise there remains broad agreement regarding the use of specific antihypertensives, with angiotensin converting enzyme inhibitors, angiotensin receptor blockers, calcium channel blockers and thiazide diuretics all preferred as first line options in isolation or in combination.
Whilst not covered in the scope of this review, it Is relevant to comment on the 2019 NICE hypertension guidelines. 62 NICE guidelines are produced with a slightly different emphasis compared to European and American guidelines, still using best available clinical evidence but with a greater focus on cost-effectivity, and with a narrower focus on the UK population and standard UK medical practice.
The targets for treatment of BP in the NICE guidelines are markedly higher than both European and American guidelines in both younger and older adult groups. NICE consider the SPRINT trial evidence to be inapplicable to the UK population due to the automated BP measurement performed as standard in the trial. As this is not common in the UK it was not included as part of their guidance, but they do acknowledge the potential benefits of maintaining BPs at a lower range. 62
In addition, the NICE guidelines are more prescriptively focussed on CVD risk estimation using a tool such as QRISK2 for initiation of anti-hypertensive therapy in patients with BP < 140/90. This stems from a cost-effectiveness analysis performed by NICE themselves demonstrating an incremental cost-effectiveness ratio at QRISK2 > 10% in males over the age of 60 of £10,000 62 and concerns re increased harms when instituting therapies at lower BPs. 86
Blood glucose
Diabetes Mellitus (DM) is a recognised risk-factor for CVD and is commonly grouped together with hypertension and dyslipidaemia under the umbrella of the metabolic syndrome. While some studies have struggled to show significance, meta-analyses have demonstrated that intensively treating DM and maintaining appropriate glycaemic control reduces the risk of CVD, with discrepancies in statistical significance likely due to inappropriately short follow-up times. There is clear evidence of increased CVD risk with longstanding DM and event rate increases with glycaemic burden as evidenced by the UKPDS. 87
As with almost all medical conditions, sustained lifestyle alterations discussed above can produce marked changes in disease burden and have been causally linked with a reduction in ACSVD. As such they should be recommended to all individuals with DM as a first line option, with metformin as the first-line pharmacological option. Metformin use leads to clear reductions in both glycated haemoglobin (HbA1C) levels and CVD rates but is inferior to anti-hypertensive and lipid-lowering therapies in terms of relative and absolute risk reduction. 87 Intensive control of HbA1C has been shown to be of benefit in reducing CVD, 88 though recent data suggests this is more effective in younger populations with recent diagnoses compared to older patients in whom this risk has been present for some time. 89
Whilst clearly required in type 1 DM, the cardiovascular rationale for insulin usage in type 2 DM is not without controversy. Whilst it is known to improve HbA1C and thus theoretically improve macrovascular risk as described above, it may contribute to atheromagenesis, it causes weight gain, increases risk of hypoglycaemia and due to increased retention of sodium can worsen systemic congestion and heart failure. 90 There have been no significant RCTs which conclusively describe its CVD safety profile, 91 while all concern over its potential for harm has stemmed from meta-analysis of observational studies with consequent inherent flaws and confounders. 90 Its use is currently predicated on its well-established ability to reduce systemic glucose exposure, with evidence from the UKPDS demonstrating that tighter glycaemic control leads to significant CVD risk amelioration. 87 Since this there has been little attempt to acquire good RCT evidence to support or refute its use, likely in part due to the ethical difficulties of conducting such a study.
Both ESC and AHA/guidelines recommend metformin as first line, while the ESC guidelines suggest subsequent consideration of the SGLT2 inhibitors due to recent evidence of their beneficial profile in this cohort. The emergence of the sodium-glucose-transporter 2 inhibitors (SGLT2) for the treatment of diabetes has been revelatory for CVD risk reduction. Cardiovascular outcome trials (CVOTs) for SGLT2s demonstrated not only safety but improved cardiac outcomes above and beyond the changes in glycaemic control.92,93 As such research is ongoing into their use specifically as a cardioprotective medicine, but notably much of their cardioprotection was due to reduction in heart failure deaths and hospitalisations as opposed to CVD. 94 Indeed, contemporary evidence suggests that they may have a use in both primary and secondary prevention of CVD, though their use in patients without DM is as yet unclear. 95 As yet their use is not specifically recommended by either American or ESC guidelines, but with further data they may be considered in forthcoming guideline updates.
Similarly to SGLT2s, CVOTs in the Glucagon-like peptide-1 (GLP-1) class demonstrated a cardioprotective effect for some members of the class, namely liraglutide, semaglutide, albiglutide and dulaglitide. 96
Unlike SGLT-2 inhibitors, the reduction in negative cardiovascular outcomes is seen due to a reduction in macrovascular complications. Whilst this has not been demonstrated as a class effect, contemporary European guidelines have been updated to recommend that in T2DM with high risk of CVD SGLT-2 antagonists and GLP-1 agonists with proven cardiovascular benefits should be considered first line, even before metformin. 97
The benefit of their use in primary prevention of CVD is as yet unclear – whilst a recent meta-analysis did demonstrate a CVD benefit in patients without established CVD, the authors noted the small number of MACEs in the primary prevention arm, with the resultant risk of the data not being sufficiently robust upon which to base guideline recommendations for use. 98
Polypill
Polypills that have been assessed for their use in primary prevention of CVD typically contain a combination of an anti-hypertensive and a cholesterol lowering agent. Since the previous iteration of this review, data has been presented suggesting that, whilst inferior to uptitrating optimal medical therapy, there appears to be an application in difficult to reach patient populations as well as patients in whom adherence is a known concern. In these groups, combination tablets have been shown to significantly and substantially reduce CVD risk in otherwise difficult to reach populations, specifically in low to middle income countries and groups less likely to seek primary healthcare.99,100 Optimal medical therapy is clearly superior but perfect should not become the enemy of good in this scenario and prescribing with appreciation of patient-specific factors remains important. Currently neither ESC nor AHA/ACC recommend its use, particularly in place of optimal guideline recommended therapies,6,39 though it appears to offer benefit in difficult-to-reach patient populations.
Anti-platelets
Since publication of the previous article, the case against the use of anti-platelets for primary prevention has strengthened. Further evidence from recent RCTS including ARRIVE, ASPREE and ASCEND have demonstrated the largely deleterious effects of taking aspirin for primary prevention, with no substantial reduction in CVD but a significant increase in major bleeding. 101 As a result, it appears we are now largely in a post-aspirin era for primary prevention and its blanket prescription for primary prevention of CVD is to be avoided. 102 ASCEND did suggest that aspirin may reduce CVD events in patients with well controlled diabetes but with a corollary increase in major bleeding events of a similar margin. 103
Amongst patients with high CVD risk and low bleeding risk this may remain a discussion to be had with the patient regarding risks vs benefits but in the majority of patients, contemporary evidence suggests that this strategy be avoided; this is reflected in contemporary guideline advice both in Europe and America.
Conclusion
While the evidence behind lifestyle modification for primary prevention of cardiovascular disease is moving slowly, we see that there are evolving therapies for the pharmacological reduction of risk. Guidelines remain divergent in terms of aggressive vs conservative approaches to hypertension management. New data are likely to emerge regarding the long-term risk of electronic cigarettes, the use of which currently seem a preferable to smoking, but still likely harmful. Doubtless there are further therapies and interventions that will help to reduce risk of CVD, but adherence to guideline recommendations regarding lifestyle modification has a powerful effect on risk reduction and is recommended as a first line intervention.
Footnotes
Acknowledgements
The authors would like to thank Drs Nicola Raeside and Maredudd Harris for their assistance in proof-reading.
Contributorship
The Lifestyle modification section was primarily written by Katherine Addy and Sarah Campbell and reviewed and edited by Jack Stewart while the Pharmacological therapy section was primarily written by Jack Stewart and reviewed and edited by Katherine Addy. The review was supervised and guided by Peter Wilkinson.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Not applicable.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
Jack Stewart.