
Abstract
Objectives
The present study uses the Atlanta Heart Failure Questionnaire as a tool to evaluate and design a tailored education material for ambulatory heart failure patients with preserved ejection fraction, highlighting the strengths and weakness toward the planning of education programs.
Methods
A total of 450 patients were screened; 112 patients were recruited, and 27-item was used to evaluate the usefulness of this questionnaire. All patients received education by a dedicated medical education about the nature of the disease, risk factors and management including prevention of complications. Descriptive statistics were used for assessing the sample characteristics.
Results
In the assessment of patient disease knowledge, in a 7-item questionnaire, the most well-understood item was correctly identified in 95% patients, whereas the least-understood item was identified in 1.8% of patients. In the assessment of patient management knowledge, in a 6-item questionnaire, the most well-understood item was correctly identified in 50% of patients and the least-understood item was identified in 10% of patients. In the assessment of patient medication intake knowledge, in a 3-item questionnaire, the most well-understood item was correctly identified in 97.3% of patients and the least-understood item was identified in 26.6% of patients.
Conclusion
For a disease not fully understood, the study has concluded the usefulness of Atlanta Heart Failure Questionnaire for filling the gaps, setting a base line and follow-up in the process of educating ambulatory heart failure patients with preserved ejection fraction HFPF.
Introduction
Heart failure (HF) is a disease that mostly develops due to chronic risk factors such as diabetes mellitus, hypertension, and ischemic heart disease. Controlling such risks factors delay and may even prevent the development of heart failure. Unfortunately, all risk factors are asymptomatic in its early stages and require knowledge, medical follow-up, and commitment to deal with such condition not only to control the disease but also to prevent the development of the adverse complications. 1 Heart failure has emerged as a major health problem, which shows significant impact on economic situation, mortality, and quality of life of individuals. Lack of patient knowledge regarding heart failure results in social isolation, lack of self-care, co-morbidities, and worsening of quality of life. 1
There is a reduction in the severity of disease and heart failure-related symptoms by adhering to current heart failure guidelines for improving the prognosis related to mortality and re-hospitalizations.
2
Three types of heart failure are listed in the European Society of Cardiology guidelines:
2
Heart failure with reduced ejection fraction of less than 40%. Heart failure with medium range ejection fraction of 40%–49%. Heart failure with preserved ejection fraction of 50% or more.
Improved outcomes for hypertensive and diabetic patients can be attained with education concerning their disease and lifestyle modifications. 3 The very first heart failure knowledge instrument was a 3-part tool that was administered by home health nurses assessing learning style, family and environment, and current knowledge. 4 This mainly focused on the level of awareness among heart failure patients regarding the process, activity, medications, and diet. 4 Expert review is likely to be used for the establishment of content and face validity. This tool is to be used positively for determining comprehensive and focused teaching to the patients with heart failure.
Another study conducted by Artinian et al. 5 was successful in developing a 13-item multiple choice test questionnaire that also included additional items requiring short answers. The items included in this questionnaire were based on clinical experience and validity analysis because this type of questionnaire was performed by a nurse practitioner. Similarly, another study was based on a 15-item multiple choice test, known as the Dutch Heart Failure Knowledge Scale that assessed heart failure patients that had to be hospitalized. 6
The two most common causes for hospital readmissions of patients with HF are the failure to keep to a medications regimen and low adherence to a low-sodium diet. Thereby, it is essential to accurately evaluate the diet of a patient, which is important for the control of HF. In addition, sociocultural values of patients should be evaluated that helps to make adequate food selection when making a diet plan. In general, the education and knowledge of HF in patients and their families are an important factor in disease management. Thus, medical personnel play a vital role in educating patients about their disease process autonomously.
The successful management of HF patients relies on controlling signs and symptoms, which include drug regimens, exercise plans, daily weights, and diet control of salt intake. The achievement of treatment plans is important for improving outcome and quality of life. The present study aims to use the Atlanta Heart Failure Questionnaire as a tool to evaluate and design a tailored education material for patients with heart failure and preserved ejection. This is the first time that such a questionnaire is tested in such a cohort of patients that showed usefulness in setting a base line for the level of knowledge that patients at risk for heart failure possessed. It may be an important tool in designing patient educational programs and utilizing the questions as a key performance indicator KPI for follow-up in the collaborating effort and preventing heart disease. The results are likely to depict the usefulness of the Atlanta Heart Failure Questionnaire for setting a base line and follow-up in the process of educating ambulatory heart failure patients with preserved ejection fraction. Moreover, it is also of importance in developing patient education material in heart failure programs for treatment and prevention.
Theoretical background
The prevalence of heart failure increases with age, and requires management, especially in ischaemic cardiomyopathies. The patient’s adherence to treatment can be improved through non-pharmacological management that include, self-care management, self-care behaviour, and patient education. 7 The higher cost of heart failure is associated with higher rates of hospitalization. 8 Severe physical symptoms are experienced by the majority of heart failure patients which visit emergency departments and are admitted. 9 Therefore, it is obvious that the negative impact on the health of these patients can be prevented first, and once the diagnosis of heart failure is established, then the prognosis can be improved by assessing the physical symptoms through a reliable and valid instrument.
Studies have used various instruments to assess the physical symptoms among patients suffering from heart failure, such as the Heart Failure Somatic Perception Scale (HFSPS), 10 MSAS-Short Form, 11 Memorial Symptom Assessment Scale (MSAS), 12 and Kansas City Cardiomyopathy Questionnaire (KCCQ). 13 In the former and latter instruments, it is difficult to differentiate the physical symptoms from functional impairment. Therefore, an efficient scale is needed to measure the frequency, stability, and burden of the physical symptoms experienced by patients. The depressive and physical symptoms can be improved through different types of interventions that include: tele-health communication devices, comprehensive discharge programs, educational programs, and appropriate diet charts and exercises. 14
Heart failure not only creates psychological and physiological burdens, it can also impose a severe economic burden on health insurance systems. A study conducted by Kato et al. 15 showed significant reduction in hospitalization rates as a result of disease management programs that enhanced self-care among the patients. This is linked to an increase of knowledge regarding their own condition, although the improvement in hospitals was not specified. A few studies have shown better adherence is associated with greater knowledge, although knowledge regarding heart failure does not always result in adherence to therapeutic regimens.6,16,17
In this regard, a study by Sedlar et al. 18 has identified personal and environmental factors that should be taken into consideration with self-care behaviours among HF patients, which include health-related qualify of life, gender, education, and age. Another study has found that poor self-management capacity of HF patients is associated with gender, disease severity, number of comorbidities, age, ethnicity, low income, literacy, education, and baseline self-management capacity. Thereby, there is a need to put forth efforts for enduring unravelling success of self-management interventions and for validating the shifting influence of patient characteristics. 19
Methods
Instruments
At the initial phase, Atlanta Heart Failure Knowledge Assessment Test was used for evaluating the knowledge of patients and their families regarding heart failure and its treatment (including self-care). For this purpose, a 27-item instrument was used that would help in measuring change in knowledge after being exposed to education and self-management intervention. The items of the questionnaire measure different factors of patient education that relate to the process of heart failure. These items are based on the concepts that are associated with clinical recommendations, mainly emphasizing on self-care. The items included in the study were arranged in the following way: pathophysiology (2 items), symptom management (4 items), behaviour (5 items), medication (5 items), and nutrition (11 items).
The test scoring attributed to 1 point for a correct answer; however, with this there was no additional weighting of the items. This is likely to be followed by gathering the correct responses. Against each item, there were more than two choices as this instrument was developed for discrete knowledge measurement. The questionnaire was revised based on the comments provided by the researchers. An official translation body translated the data collected from Arabic into English.
Study population
A total of 480 patients were screened from which the study has collected data from 112 heart failure ambulatory heart failure patients with preserved ejection fraction (HFpEF). The study has been approved by Institutional Review Board of King Abdulaziz University, Saudi Arabia. Written consent was obtained from recruited patients.
Inclusion criteria
The eligibility criteria for this study were:
Ability to read, write, and speak English. Telephone access. Diagnosis of heart failure with preserved ejection fraction. Symptoms of heart failure. Shortness of breath. Lower limb oedema. History of hospitalization for heart failure. Echo EF more than 50% with diastolic dysfunction.
Data collection
The patient medical records were used to gather patient demographic and clinical data at Internal Medicine Clinic, King Abdulaziz University Hospital, Saudi Arabia. The patients were told to complete the Atlanta Heart Failure Knowledge Assessment Test. Before completing the questionnaire, patients were asked to sign a consent form to ensure their participation in the study. The patients were requested to answer each question to the best of their abilities, but if they did not know an answer they were permitted to make an educated guess. The patient demographic and clinical data obtained from their history showed that the ratio of males to females was equal (Table 1). Regarding the risk factors, the majority of the patients stated that they were suffering from diabetes (65.2%), hypertension (69.9%), obesity (32.1%), and were not habitually smoking (95.5%); 52.7% of patients stated that they knew that any previous risk factor is responsible for causing HF, whereas 47.3% of the patients disagreed on this (Table 1). The last item “previous risk factor is responsible for causing HF” was assessed as the one that can be used to develop educational interventions and to improve patients’ knowledge.
Demographic characteristics of the respondents.

Data analysis
Descriptive statistics were used for assessing the sample characteristics. Item statistics were also generated to describe discriminations and difficulties faced by patients. The data were analysed using Statistical Package of Social Sciences (SPSS) version 20.0. Means and standard deviations were used for descriptive statistics and Pearson correlation coefficient was used for inferential statistics, showing the association between patient education and questionnaire items.
Results
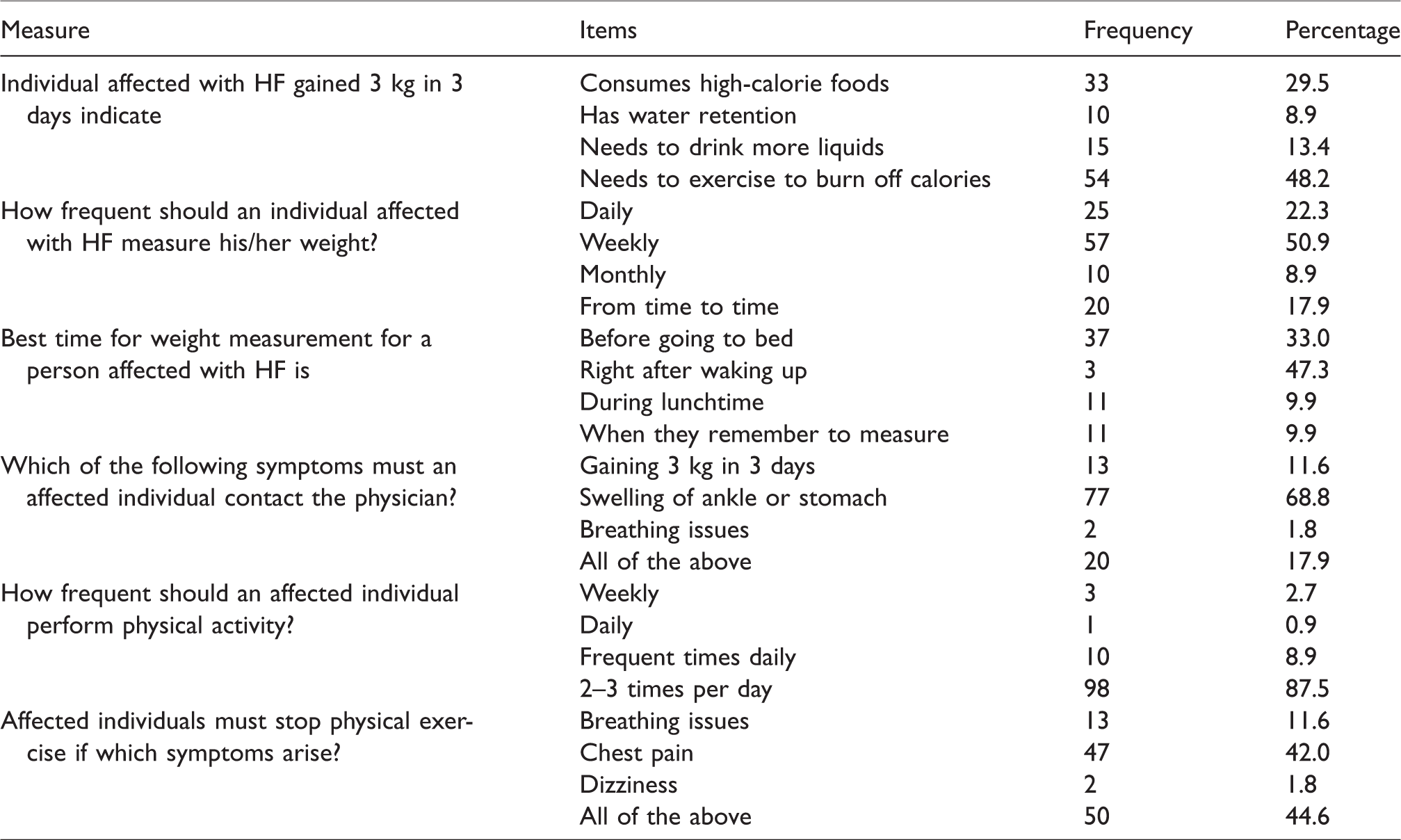
In Table 2, the first group of questions is about assessing patient education regarding management of HFpEF; six questions were used. The first indication question, “In the individual affected with HFpEF gained 3 kilograms in 3 days”, 8.9% of the participants said “has water retention” which is the correct answer, whereas 48.2% chose “needs to exercise to burn off calories”. In the question on how frequently an individual affected with HFpEF should measure his or her weight, 50.9% of the respondents said “weekly” as an answer for the second question, yet the correct answer is “daily”, which was chosen by 22.3% of patients. In the question regarding the best time for weight measurement for a person affected with HF, only 64 (48%) answered correctly (“right after waking up”), while 33% answered “before going to bed”. In a similar manner, the question, “Which of the following symptoms must an affected individual contact the physician?”, 68.8% answered wrongly, with “swelling of ankle or stomach”, whereas only 17.9% chose the correct answer “all of the above”. When patients were asked about the frequency of the physical activity, the majority of the respondents (87.5%) chose the wrong answer “2–3 times per day”. Only 0.9% answered correctly, with “daily”. While 44.6% got the right answer with regard to the symptoms that prevent the physical activity, 42% chose “chest pain”.
Assessing patient education regarding HF.

Table 3, on assessing patient education regarding heart failure with preserved ejection fraction reports on seven questions. The maximum score of all items was 95.5% and the minimum score was 1.8%. In the issues related to HFpEF question, the majority (95.5%) chose “increases the blood volume in the body”. Only 3.6% chose the correct answer, which was “medications can be used to treat HFpEF”, as compared to 57.1% patients that wrongly chose “individuals affected with HFpEF cannot have a normal life”. Only 27.7% of patents in the questionnaire said that HF patients should avoid foods with high level of salts. Also, 16.1% said “no” to HFpEF patients drinking large amount of fluids, which is the correct answer. But 67.9% patients correctly said “yes” to HFpEF patients quitting smoking. Among study participants, only 1.8% said “no” to stopping the medications when HFpEF patients feel better. Only 22.3% thought that it is important to know the signs that require them to contact the physician.
Assessing patient education regarding medication intake for HF.

Table 4, the last group of questions assessed patients’ education regarding medication intake for HFpEF. For the first question (“How do common medications used for HFpEF increase the heart capabilities to pump blood?”), most patients (97.3%) answered correctly by electing that they “remove excess fluids and sodium from the body”, while only 26.6% correctly knew that diuretic medication helps the kidneys to generate urine in heart failure patients with preserved ejection fraction patient. Finally, only 44.6% chose the correct answer, which is to “know if they have to take potassium supplements”, in response to the question, what an HFpEF patient on diuretic medication must do.
Assessing patient education regarding management of HF.
In the assessment of patient education regarding nutrition intake in the management of HF. Patients were asked about 11 items, the majority of patients scored true answers in seven items and wrong in four items as shown in Table 5. Three of the fault’s answers are discussing salt intake and one discussing fluids intake for HFPEF patients.
Assessing patient education regarding nutrition.

Discussion and conclusions
Discussion
The findings have added to knowledge in this field, showing the nature of gap in education, awareness, and knowledge of patients with respect to ambulatory heart failure with preserved ejection fraction HFPF. The patients reported that alarming symptoms like swelling of ankle and stomach, or breathing issues, they should immediately contact their physician. Low level of knowledge regarding heart failure and its management leads to social isolation, lack of self-care, worsening of the quality of life, and increased comorbidities. 1 Inheritance of these factors increases healthcare costs as the knowledge of patients characterizes their adherence to treatment and its success.20,21 The impact of teaching and learning can be measured through assessment tools in health educational programs, which may include possible modifications to the attitudes of patients towards heart failure. 1
There is much variation in the publication of complete instruments, comprehensive psychometric properties, and scoring; educational interventions and knowledge of individuals about heart failure have been reported extensively. The present study has assessed the education level of patients, which revealed that they were aware that patients with HF should avoid salty food, stop smoking, and immediately contact doctor if any alarming symptom is observed. The knowledge of patients regarding their own disease is the initial step towards the development of educational action. A similar study conducted by Bonin et al. 1 assessed the level of knowledge of HF patients in comparison with their socio-economic characteristics. The results showed that higher score was achieved by the patients with greater family income and educational level.
The study findings have shown that majority of the participants had critical gaps in their knowledge of HF and its management. It has been shown that patient-related factors contribute towards adequate or proper knowledge in HF patients. A study conducted by Irene 22 determined the self-care behaviour practices and knowledge in HF patients, through cross-sectional analysis. The study found an association between HF knowledge scale scores and self-care behaviour scale scores in demographic variables. The results showed that the level of knowledge in the majority of patients was poor regarding the management of HF, symptom recognition, and management of symptoms.23
The study is limited in a small number of respects, such as the sample size being comparatively small and using participants from a limited demographic. Therefore, these findings require further confirmatory evidence, which may be met with a larger sample.
Conclusion
The present study has assessed the use of the Atlanta Heart Failure Questionnaire as a tool to evaluate and design tailored education materials for ambulatory heart failure patients with preserved ejection fraction. This tool met the psychometric properties from its development to its validation. Despite the small sample size, with an average score of 37.9%, the results have depicted the usefulness of Atlanta Heart Failure Questionnaire for filling the gaps, setting a base line and follow-up in the process of educating ambulatory heart failure patients with preserved ejection fraction. For future research, the study has highlighted the need to establish more standardized HF education programs for the patients to minimize gaps in patients’ knowledge regarding heart failure with preserved ejection fraction. Moreover, the study recommends assessment of HF knowledge and self-care to be a continuous process, applying the Atlanta Heart Failure Questionnaire to identify and address the deficits, aiming for a better patient care.
Footnotes
Acknowledgements
■.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
■.
Guarantor
■.
Contributorship
■.