
Abstract
Objective
In this study, we aimed at correlating the thickness of epicardial adipose tissue and levels of Vitamin D with cardiac risk in patients with familial Mediterranean fever.
Methods
Sixty-five patients with familial Mediterranean fever and 38 healthy controls with matching age and sex were included in the study. The patients with a history of familial Mediterranean fever attacks within the previous two weeks or with any history of inflammatory or cardiovascular disease were excluded. Data regarding age, gender, weight, height, waist circumference, body mass index (calculated as weight/height2), pulse wave velocity, serum Vitamin D levels from fasting blood samples, and Homeostatic Model Assessment for insulin resistance were obtained for the patients and controls. The epicardial adipose tissue was visualized as an echo-free space between the outer surface of myocardium and visceral pericardium using two-dimensional echocardiography, and the thickness of epicardial adipose tissue was measured in parasternal long-axis view at the end of diastole.
Results
The patients with familial Mediterranean fever had significantly higher levels of C-reactive protein, epicardial adipose tissue, and pulse wave velocity (p < 0.001, <0.05, <0.005, respectively) as compared with the control group. However, the serum Vitamin D levels in the two groups were observed to be similar (p = 0.486). Weak but significant positive correlations were observed between epicardial adipose tissue thickness and C-reactive protein (r = 0.302, p < 0.005), epicardial adipose tissue thickness and pulse wave velocity (r = 0.263, p < 0.01), and C-reactive protein and pulse wave velocity (r = 0.235, p < 0.05).
Conclusion
Thickness of epicardial adipose tissue and pulse wave velocity were observed to increase in patients with familial Mediterranean fever.
Introduction
Cardiovascular diseases are a major cause of morbidity and mortality in most autoimmune diseases. familial Mediterranean fever (FMF) is an autosomal recessive, autoinflammatory disease, wherein inflammation at subclinical level continues during periods between the attacks. Continuous subclinical inflammation results in endothelial dysfunction, negatively affecting the cardiovascular system. Chronic subclinical inflammation has been reported to be associated with the development of coronary artery disease. 1 Impairment of both right and left ventricle functions can be observed in patients with FMF. Additionally, pericarditis, rhythm disorders, and atherosclerosis may occur, and aortic elasticity may change in patients with FMF. 2 As a result of inflammation, the increased inflammatory mediators in circulation decrease the aortic elasticity and increase the arterial stiffness. 3
The studies in healthy individuals and hypertensive patients have revealed that arterial stiffness, assessed by pulse wave velocity (PWV), is closely associated with increased cardiovascular risk and mortality. 4 Arterial stiffness index has also been reported to increase in FMF patients. 3 Epicardial adipose, which secretes many pro-atherogenic and pro-inflammatory adipokines, is a special form of visceral fat stored around the heart and is an important indicator of cardiovascular risk. Epicardial adipose tissue (EAT) thickness and volume are associated with obesity, impaired glucose tolerance, metabolic syndrome, hypertension, diabetes, and atherosclerosis. 5 Although EAT thickness has less adipocyte density than other visceral fat stores, it is more efficient in the intake and secretion of fatty acids. 6
25(OH) Vitamin D inhibits the vascular calcification of blood vessels, improves endothelial functions, and has an antiatherosclerotic effect. 7 Vitamin D acts against atherosclerosis by inhibiting the conversion of macrophages to foam cells, down-regulating the proliferation and migration of vascular smooth muscles, and suppressing the inflammation which triggers the expression of endothelial adhesion molecules. 8 Clinical trials in individuals with chronic kidney disease have reported that deficiency of Vitamin D can independently cause cardiovascular diseases such as coronary vascular calcification and cardiac failure, and mortality. 9 A study also reported that low levels of 25(OH) Vitamin D were associated with sudden cardiac death in diabetic patients on hemodialysis. 10
The early prognosis of atherosclerosis could be essential in FMF patients presenting with subclinical chronic inflammation. This could be done by assessing levels of Vitamin D, aortic stiffness index, and EAT thickness, all of which are associated with cardiovascular risk. To this end, EAT thickness, arterial stiffness index, and Vitamin D levels of FMF patients were compared with healthy individuals.
Methods
Study protocol
This was a single-center, prospective, cross-sectional study. Sixty-five patients diagnosed with FMF on the basis of Tel-Hashomer criteria, 11 using colchicine, and 38 healthy individuals between the ages of 18 to 70, who had been admitted to the internal medicine outpatient clinics between 1 November 2015 and 31 May 2016, were randomly selected. Ethical Committee Approval for the study is obtained accordingly (Approval number: 26.06.2016/44). Those who had read and signed the consent form were inducted into the study in patient and control groups, based on their health status.
The following were exclusion criteria:
Patients who had an FMF attack within two weeks before admission Patients with chronic renal failure (glomerular filtration rate of <60 ml/min) Patients with known coronary artery disease, congestive cardiac failure, moderate to severe valvular heart disease, pericardial disease, congenital valvular heart disease (bicuspid aortic valve, atrial septal defect), and who had undergone cardiac surgery for any reason Patients with chronic pulmonary disease Patients being monitored for malignancy Patients with active infection or undergoing treatment for FMF attack and infection within the last two weeks Patients with hemoglobin value of <9.0 g/dl Patients with white blood cell count of >16 × 103 and <4 × 103/µl Patients with rheumatological disease other than FMF Patients with amyloidosis Presence of hyperlipidemia Presence of primary hyperparathyroidism Patients with bone metabolic disorder (rickets, osteoporosis, or osteopenia) and using medication for its treatment Thyroid gland dysfunction
General evaluation and assessments
Age, sex, and smoking status of each participant included in the study were recorded. Body mass index (BMI) was calculated as the weight in kilograms divided by the square of the height in meters. A waist circumference (WC) of 102 cm or more in males and 88 cm or more in females was considered as increased WC.
Echocardiographic evaluation was performed in the ECG room using the Philips Echocardiographic device (Epiq 7, Holland) with a 2.5 MHz transducer. Epicardial fat tissue was visualized as the relatively anechoic space between the visceral pericardium and right ventricle. Maximum EAT thickness was obtained by measuring the thickness of the space between the right ventricle and visceral pericardium, on the line vertically drawn from end-systole right ventricle to the midventricular free wall at the parasternal long axis, on a two-dimensional image. The differentiation of systole and diastole was determined on the basis of ECG readings. The assessments were performed by a cardiologist who did not have access to patient data. In order to determine interobserver variability, the echocardiograms of 20 study subjects were evaluated and their EAT thickness assessments were repeated after a week. Reproducibility of the assessments was statistically highly significant (intraclass correlation coefficient 0.921, p < 0.001).
PWV assessments were performed using the SphygmoCorR Pulse Wave Velocity System (Atcor Medical, Australia). Right carotid and femoral arteries were used as pressure recording points for the participants, and wave transmission time was automatically calculated by the device. PWV assessments were done using a three-lead electrocardiogram connected to the device and were calculated by software in the device.
Blood samples from the antecubital vein were taken from all participants after fasting for 12 h, and parameters such as complete blood count, fasting blood glucose, creatinine, albumin, total protein, sodium, potassium, blood urea nitrogen, aspartate transaminase, alanine transaminase, uric acid, calcium, C-reactive protein (CRP), thyroid stimulating hormone, total cholesterol, low-density lipoprotein, high-density lipoprotein, triglyceride, parathyroid hormone (PTH), phosphorus, and 25(OH) Vitamin D were measured. A Vitamin D level of 0–20 ng/ml was considered as very deficient, 21–29 ng/ml as mildly deficient, and 30–100 ng/ml as optimal.
Statistical analysis
For analysis of the data, the software package SPSS version 18.0 (Statistical Package for Social Sciences Inc., Chicago, Illinois, USA) was used. Categorical variables were expressed as percentages, and numerical variables were presented as the arithmetic mean ±standard deviation. The normality of distribution of the numerical variables was evaluated by one-sample Kolmogorov–Smirnov test. The presence of a linear relationship between the normally distributed parameters was checked using Pearson’s correlation test, while Spearman’s correlation test was used for nonnormally distributed parameters. The differences between various groups were analyzed using Student’s t-test for the parameters with normal distribution and the Mann–Whitney U test for those without normal distribution. The results were considered statistically significant if p-value was <0.05. Sample size of the study was estimated according to the study by Yildiz et al. 12 to obtain 80% power. It was calculated on a Power Analysis and Sample Size (PASS 6.0, USA) that a minimum of 36 participants in each group would be needed to provide sufficient power.
Results
Sixty-five FMF patients and 38 healthy individuals fulfilling the study criteria were included. Sixty-five of the study subjects were females and 38 were males. The mean WC was 96 ± 8 cm and mean BMI was 29.0 ± 4.4 kg/m2. Mean systolic blood pressure of study participants was 120 ± 10 mmHg, and mean diastolic blood pressure was 74 ± 7 mmHg. Comparison of clinical, laboratory, and echocardiographic data of the groups is presented in Table 1.
The clinical and laboratory parameters of FMF cases and the control group.
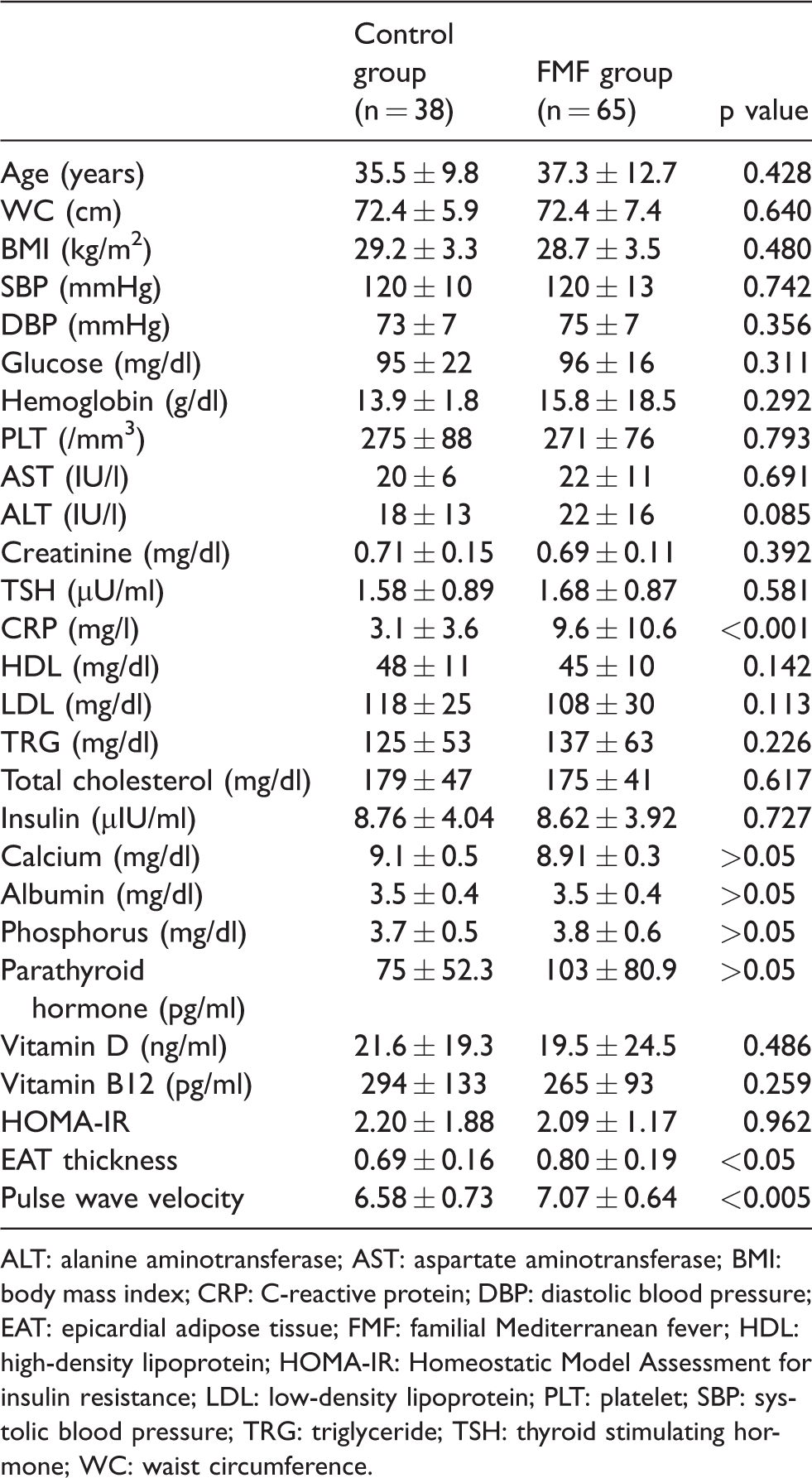
ALT: alanine aminotransferase; AST: aspartate aminotransferase; BMI: body mass index; CRP: C-reactive protein; DBP: diastolic blood pressure; EAT: epicardial adipose tissue; FMF: familial Mediterranean fever; HDL: high-density lipoprotein; HOMA-IR: Homeostatic Model Assessment for insulin resistance; LDL: low-density lipoprotein; PLT: platelet; SBP: systolic blood pressure; TRG: triglyceride; TSH: thyroid stimulating hormone; WC: waist circumference.
The levels of CRP and Vitamin D significantly differed between the two groups (p < 0.001 and p < 0.01, respectively). Both EAT thickness and PWV were observed to be statistically significantly higher (p < 0.05) in the FMF group, compared to the control group.
Threshold value for 25(OH) Vitamin D was set at 30 ng/ml, and EAT thickness values were compared between individuals with low and optimal 25(OH) Vitamin D levels. EAT thickness values of subjects with optimal Vitamin D level (0.79 ± 0.16 mm) and those with low Vitamin D level (0.74 ± 0.19 mm were statistically similar (p > 0.05).
Discussion
FMF is an autosomal recessive, autoimmune rheumatic disease characterized by fever and inflammation of the serosal membrane. Endothelial dysfunction and increased intima-media thickness have been reported in studies on FMF patients. 13 The studies have also reported the cardiac risk to possibly increase in amyloidosis-related FMF, due to reasons such as increased levels of asymmetric dimethylarginine and inflammation markers.14,15 A study evaluating the elastic properties of the aorta, ventricle function, and the presence of pericardial effusion in FMF patients reported the presence of a subclinical myocardial involvement in younger FMF patients without conventional cardiovascular risk factor. 16
The assessment of epicardial fat tissue is one of the best methods to quantitatively assess the relationship between autoimmune rheumatic diseases and the cardiovascular system. 17 Since the epicardial fat tissue has a similar embryological origin as other visceral fat tissues, the assessment of total visceral fat is an easy, inexpensive, and quantitative method for echocardiographic EAT thickness assessment. The epicardial fat tissue is a metabolically active organ and synthesizes many bioactive molecules influencing the cardiac function. The increased amount of epicardial fat tissue was observed in several patients undergoing coronary bypass procedure. 18 Although EAT thickness can also be assessed by other techniques such as CT or MRI, echocardiographic assessment is recommended as it is inexpensive and convenient. 19 The present study also used the echocardiographic assessment method.
Several studies have reported that increased epicardial fat tissue thickness is associated with autoimmune diseases such as rheumatoid arthritis and ankylosing spondylitis. 20 A study on pregnant women with FMF observed that levels of EAT thickness were significantly higher in FMF patients than in healthy individuals and that this relationship was correlated with the disease duration. 21 We also observed the EAT thickness values in patients with FMF to be significantly higher than the healthy individuals (p < 0.05).
Increased arterial stiffness can independently increase the risk of cardiovascular diseases. 22 Inflammation caused by autoimmunity and other disease-related factors may lead to arterial damage, which may result in increased PWV by impairing vascular functions. Increased arterial stiffness has been reported in patients with systemic lupus erythematosus, rheumatoid arthritis, and Behcet’s disease. 20 It is possible to detect impairment in aortic elasticity if FMF patients with normal clinical and echocardiography results are evaluated further.
If arterial stiffness is increased, the amount of blood pumped during systole increases, resulting in decreased coronary perfusion and increased PWV. 23 Furthermore, an increase in pulse pressure interval causes increased remodeling of arteries, the formation of plaques on arteries, and rupture of the plaques. 24 Increase in PWV, which is correlated with an increase in arterial stiffness, was reported in FMF patients. 25 As PWV is an indicator of arterial stiffness and is also associated with FMF, measurements of PWV may be used as a precursor of atherosclerotic process. We also observed increased PWV in FMF patients, which could also indicate the presence of subclinical effects in FMF patients.
Vitamin D is known to be beneficial to the cardiovascular system. The positive effects can be attributed to the antihypertensive, antidiabetic, PTH suppressive, anti-inflammatory, antioxidative, and renoprotective properties of Vitamin D. 7 In the studies on animal models, it was observed that active Vitamin D accelerated the relaxation of myocytes and improved the diastolic cardiac functions. 26 Likewise, active Vitamin D supplements reduce the PTH levels, which have been associated with increased blood pressure, cardiovascular disease, and mortality. The supplementation with natural Vitamin D has been shown to decrease the systolic blood pressure by 2–6 mmHg. 7 The Framingham Offspring Study revealed that the chances of cardiovascular events were 53–80% higher in individuals with low 25(OH) Vitamin D, without any history of cardiovascular disease. 27 Another study wherein 3258 patients who had undergone coronary angiography were followed up after a mean period of 7.7 years reported that cardiovascular and overall mortality was higher in individuals with low 25(OH) Vitamin D levels. 28
The researchers observed low bone mineral density in lumbar vertebrae, femoral neck, and entire femur in FMF patients with deficiency of Vitamin D and suggested that FMF was an independent risk factor for osteoporosis. 29 Kisacik et al. 30 reported that Vitamin D deficiency in FMF patients could also trigger the attacks. The abovementioned beneficial cardiovascular effects of Vitamin D could be attributed to its ability to downregulate pro-inflammatory cytokines and its anti-inflammatory properties. 30 Deficiency of Vitamin D could lead to insufficient immunosuppressor effect, thus contributing to inflammation in FMF patients. In an asymptomatic community-based study, Vitamin D deficiency was observed to be correlated with an increase in arterial stiffness and endothelial dysfunction. 31 Although we also observed low Vitamin D levels in FMF patients, we could not find a significant relationship between Vitamin D levels and EAT thickness. This may be due to the relatively small sample size.
Limitations of the study
There were some limitations to the present study. The first and the most important limitation was the number of patients included in the study. The second limitation is lack of information about duration, severity, and frequency of the attacks although relatively middle-age subjects were enrolled.
Conclusion
FMF patients are at risk of cardiovascular system complications even in the absence of known cardiovascular risk factors. Echocardiography is a highly valuable method in the early visualization of the effect of FMF on cardiac function. Hence, transthoracic echocardiographic evaluation of FMF patients and calculation of EAT thickness and PWV is essential for the early diagnosis and treatment of cardiovascular diseases. Similarly, the deficiency of Vitamin D which is directly correlated with cardiac risk is one of the parameters to be considered during monitoring of FMF patients.
Footnotes
Acknowledgments
This article was derived from the thesis of Dr Mustafa Kozan which was accepted and approved by Bozok University Faculty of Medicine in 2016. Additionally, the abstract of the manuscript was accepted as an oral poster in International Congress of 13. Update in Cardiology and Cardiovascular Surgery held in Antalya at 23–26 March 2017.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Bozok University Faculty of Medicine Ethics Committee for Clinical Researches; Approval number: 26.06.2016/44.
Informed consent
Written informed consent was obtained from all subjects before the study.
Guarantor
None
Contributorship
None