
Abstract
Aims
The Multiple Stent Delivery System (VascuFlex® Multi-LOC) is a novel stent delivery system with six short stents (13 mm long each) mounted on one wire-guided catheter, designed for the treatment of femoropopliteal arteries. The aim of the present study is to evaluate the safety and the feasibility of the VascuFlex® “Multi-LOC” stent delivery system, which enables spot stenting without changing the delivery system.
Methods and results
After proof of concept in a porcine model and after European Conformity marking, first clinical experiences were gathered in 20 patients with severe intermittent claudication or critical limb ischemia. First-in-human data are presented. The study included 20 limbs that underwent femoropopliteal revascularization for claudication (n = 14) or critical limb ischemia (n = 6). “Multi-LOC” provisional spot stenting resulted in acute technical success in all lesions with resolution of flow-limiting dissection and elastic recoil after balloon dilatation of the femoropopliteal artery. There were no device-related complications. Follow-up examinations after 30 to 40 days revealed no major adverse events, and six months’ results were encouraging.
Conclusions
First clinical use of the novel Multiple Stent Delivery System (Multi-LOC) after balloon dilatation of the femoropopliteal artery was safe and feasible in this early study.
Introduction
The Multiple Stent Delivery System (MSDS; VascuFlex® Multi-LOC; Medicut Stent Technology GmbH, Pforzheim, Germany) is a novel 6-French multiple stent delivery system with six self-expanding nitinol stents mounted on one central wire-guiding (0.035 inch) catheter (Figure 1). Designed for the treatment of femoropopliteal arteries, the VascuFlex® Multi-LOC device enables spot stenting without changing the delivery system. Each stent has a closed cell design with a radial force and crush resistance comparable to other commercially available nitinol stents. A radiopaque tantalum marker at the proximal end of each stent prevents stent jumping and facilitates exact stent positioning.

Illustration of the Multi-LOC stent delivery system. The Multiple Stent Delivery System with six self-expanding nitinol stents mounted on one central wire-guiding (0.035 inch) catheter is available in different versions with different stent diameters (from 5 to 8 mm) and two different working lengths (80 cm and 130 cm). The device represents a new generation of stent delivery technology, developed for provisional stenting of the femoropopliteal artery in case of insufficient results after balloon dilatation.
Preclinical experience in a porcine model demonstrated excellent feasibility of the MSDS with very favorable results concerning stent fracture, restenosis, and patency of spot-stented femoropopliteal arteries compared to standard long nitinol stenting (mc-peripheral; Medicut, Germany) at 27 days postimplantation. Consistent with these angiographic data, neointimal growth as assessed by representative histomorphology was less in the short stent types. 1
These promising preliminary results have led to the use of this device in humans during the present VascuFlex® Multi-LOC clinical First-in-Man (FIM) study, with the aim of assessing the safety, feasibility, and performance of the MSDS for the treatment of de novo femoropopliteal lesions.
Materials and methods
Patients
The clinical study was a prospective, nonrandomized, first-in-human safety and feasibility study. Patients were treated at the Department of Angiology, Diakonissenkrankenhaus, Mannheim, Germany. Twenty patients were enrolled with 20 lower extremities treated. The protocol was approved by the Human Subjects and Ethics Committee at the Mannheim University Hospital. The subjects’ written informed consent was obtained and baseline clinical data were collected.
Prior to the endovascular procedure, all patients had been screened with duplex ultrasonography due to symptomatic peripheral artery disease of the lower extremities (severe intermittent claudication or critical limb ischemia) and diagnosed with significant femoropopliteal stenosis (>70%) or total occlusion. Patients had no significant stenosis of the iliac arteries of the index limb as assessed by duplex ultrasonography. This feasibility pilot study enrolled only patients with severely calcified femoropopliteal lesions, in which bailout stenting was indispensible due to inacceptable results from balloon dilation (residual diameter stenosis > 30%, or flow-limiting dissection).
Endovascular procedure and medication regimens
After puncture in an antegrade approach of the ipsilateral common femoral artery, transfemoral 6-French access sheath placement was performed and Heparin was administered. The lesion was crossed intraluminally using a standard guidewire (0.035-inch Terumo Glidewire; Boston Scientific) technique in all patients. Each patient underwent percutaneous transluminal angioplasty (PTA) with the balloon inflated to nominal pressure to match the reference vessel diameter. Post-PTA angiograms were obtained in multiple views, and residual stenosis (≥30%) was treated with repeat PTA. This pilot study only included patients, for whom multifocal provisional stent implantation was indispensable after balloon dilatation due to acute flow-limiting dissection or elastic recoil, defined as persistent stenosis ≥30% after repeat dilation. Procedural success was defined as <30% residual stenosis in the final angiogram (Figure 2).
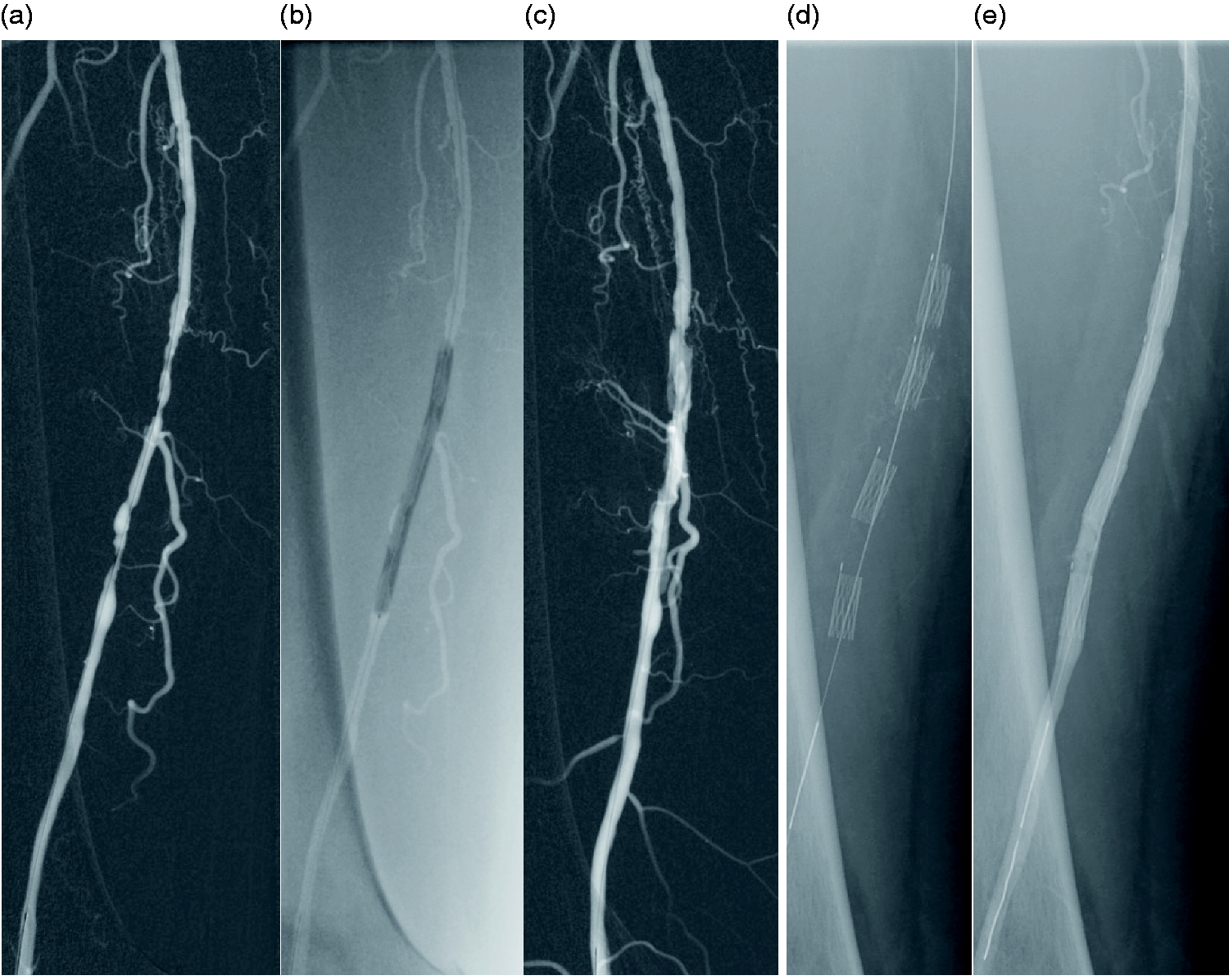
Patient with right calf claudication, who underwent PTA of the distal superficial femoral artery. Angiogram of the right superficial femoral artery revealed an 80-mm-long stenotic lesion (a). Treatment with a 5.0/80-mm uncoated balloon (b) resulted in a flow-limiting dissection (c). Four “Multi-LOC” stents were placed (d) with successful resolution of the dissected areas (e).
This was a pilot safety and feasibility study with short follow-up of 20 patients with symptomatic peripheral artery disease. The primary safety endpoint was freedom from death, target vessel occlusion, clinically or ultrasound-driven index-limb reintervention, and occurrence of surgery related to the procedure within 30 days following the procedure.
The feasibility endpoint was the ability to improve an insufficient primary result after balloon angioplasty (ability to secure dissection flaps and eliminate elastic recoil) at the time of implantation. The technical success endpoint was defined as angiographically documented acute luminal femoropopliteal patency at the conclusion of the revascularization procedure with a tibial run-off unaltered to preinterventional situation.
Required medications were consistent with the standard of care, including long-term medication with acetylsalicylic acid at a dose of 100 mg/day. A loading dose of 300 mg clopidogrel was administered immediately after the procedure for patients, who underwent provisional stent implantation, and a dose of 75 mg/day of clopidogrel was required for at least one month after the procedure.
Follow-up
The patients were treated according to the standard of care and were reassessed with vascular history and physical examination, ankle-brachial indexes (ABIs), and duplex arterial ultrasound examinations at one and six months.
While not powered to evaluate efficacy, effectiveness evaluation included assessment of Fontaine category, clinical examination, calculation of ABI, and treadmill exercise testing (3.2 km/h at a 12-degree slope) for claudication patients with pre- and postexercise ABI measurement. Duplex ultrasonography was performed for morphologic and functional evaluation of the femoropopliteal axis with significant restenosis defined as peak velocity ratios ≥2.4 at the target lesion site.
Data analysis
Categorical variables were expressed as counts and percentages; continuous data were expressed as means with standard deviations. There was no statistical analysis performed.
Results
Patient characteristics are listed in Table 1. A total of 79 stents were successfully placed in 20 femoropopliteal lesions. Stent delivery by retraction of the protecting sheath and exact stent positioning was performed without difficulties. Lesion characteristics and procedural data are illustrated in Table 2. The mean femoropopliteal lesion length was 94 mm. With a mean number of 4.0 “Multi-LOC” stents implanted per leg, the mean length of the stented segment was 51 mm, thus approximately 54% of the total lesion length.
Patient characteristics.

SD: standard deviation; GFR: glomerular filtration rate.
Lesion characteristics and procedural data.

SFA: superficial femoral artery; PA: popliteal artery; SD: standard deviation.
The primary endpoint of freedom from major adverse events 30-day postprocedure was achieved at 100% (Table 3). No stent thrombosis and no clinically or ultrasound-driven index-limb reintervention occurred. Furthermore, no surgery related to the procedure and no major amputation was necessary.
30-Day and 6-month clinical (major adverse) events.

Interventional procedures could restore the 14 patients with moderate or severe claudication (Fontaine stage IIb) to a claudication-free stage in 12 cases (Fontaine stage I) or clinical significant improvement in 2 cases (Fontaine stage IIa with an increase of maximal walking distance on treadmill testing from under 150 m prior to the endovascular procedure to over 300 m on follow-up visits). ABI measurement indicated improvement of lower leg perfusion in 15 patients, while 5 patients showed incompressible arteries due to severe mediasclerosis (1 patient with end-stage renal disease and 4 patients with long-standing diabetes mellitus type 2). Duplex ultrasonography confirmed full patency of all implanted stents, thus a 100% patency rate at one- and six-month follow-up visits (Table 4).
Baseline, 30-day, and 6-month clinical and measurement data.

All 15 patients with claudication performed treadmill testing at a treadmill velocity of 3.5 km/h and on an incline of 12%. On follow-up, a maximal walking distance of >300 m was achieved in all patients.
Five patients with incompressible arteries due to severe mediasclerosis are not included.
In two of the five patients who suffered from chronic ischemic lesions, complete wound healing could be achieved between the follow-up visits at one and six months and in two other patients, wounds were improving. Unfortunately, one patient had to be major amputated five months after the intervention due to uncontrolled local infection of the preexisting foot gangrene. At the time of amputation, duplex ultrasound showed an open target vessel without in-stent stenosis.
Discussion
First clinical use of the novel MSDS (“Multi-LOC”) after balloon dilatation of the femoropopliteal artery was safe and feasible.
In this early study, an optimal technical success rate (100%) with an excellent ability to secure dissection flaps and eliminate elastic recoil after primary balloon dilatation was observed. Even though the single-arm design of the present investigation does not allow a direct comparison with other stent delivery systems, these data suggest a good deliverability/handling/feasibility of “Multi-LOC” stents. Patients reached the prespecified primary endpoint of freedom from major adverse events at 30-day postprocedure in 100% of the cases. This observation, in addition to the encouraging procedural data, demonstrates the safety and feasibility of the MSDS (Vascuflex® “Multi-LOC”).
An additional novel feature of the MSDS methodology is that not only one but six self-expanding nitinol stents are mounted on one central wire-guiding catheter, enabling multiple stent implantation without changing the delivery system. The closed cell design of each self-expanding nitinol stent provides radial force and crush resistance comparable to other commercially available nitinol stents for provisional stenting, when scaffolding properties are needed after balloon-dilatation of femoropopliteal lesions. With a single stent having a considerably short length of only 13 mm, application of this technology helps to reduce the mass of foreign body implants and its possibly negative influence on vessel integrity (chronic outward force) and on biomechanical properties of arterial segments. Our case series comprises solely lesions, for which provisional stenting was indispensible after balloon dilatation; nevertheless, a mean lesion length of 94 mm is accompanied by only 51 mm length of stented segment. This realizes the concept of “spot stenting” together with the demand “to leave nothing or as little as possible behind,” which might be a seminal treatment modality for long segment femoropopliteal disease. 2 To enable exact stent positioning at desired location, a radiopaque tantalum marker at the proximal end of each stent prevents stent jumping and facilitates a precise anatomically controlled stent release. Furthermore, the delivering of up to six stents without changing the delivery system might allow reduction in procedural time, fluoroscopy time, and contrast usage that are clinically relevant issues for selected high-risk patients.3,4
The FIM implantation followed a preclinical evaluation of the “Multi-LOC” stent delivery system in porcine femoropopliteal arteries. In the healthy animal model, control angiography after 23 days revealed very favorable results concerning stent fracture, restenosis, and patency of spot-stented femoropopliteal arteries in comparison with a standard nitinol stent which was similar in total length. In the present investigation, color duplex ultrasonography did not show any restenosis at target lesions. This effect could be partially explained by the fact that, in the present study, only stents with a diameter of 5.0 or 6.0 mm were used and deployed in large vessels, thus reducing the clinical impact of the neointimal growth after a follow-up period of six months.
In conclusion, data observed in the present study suggest the safety and feasibility of the implantation of the novel MSDS. Promising clinical results could be shown by the follow-up examination and color duplex ultrasonography did not show any restenosis at target lesions.
These data, due to the small number of patients included in this first-in-human study, need to be confirmed by larger investigations. With permission from the ethical committee at the faculty for clinical medicine Mannheim, part of the University of Heidelberg, the LOCOMOTIVE all comers registry was established (ClinicalTrials.gov identifier: NCT02531230).
Limitations
There are some limitations to this case series. This was a pilot safety and feasibility study with a short follow-up of a small and heterogeneous group of symptomatic patients with peripheral artery disease. The lesions were distributed in the femoropopliteal artery with 90% involvement of the distal superficial femoral and/or popliteal arteries which have traditionally been considered no stent zones. No core facility was employed to either adjudicate duplex ultrasound or angiographic results in this study. The present study should be considered exploratory and no direct comparison with other nitinol stents was performed. Finally, no conclusions about efficacy can be drawn from the pilot trial design.
Conclusions
We, for the first time, demonstrate the safety and feasibility of the MSDS (“Multi-LOC”) for bailout stenting after balloon dilatation of femoropopliteal lesions in humans with symptomatic peripheral vascular disease. Further studies with a larger number of patients and a longer follow-up are needed to fully evaluate the performance and efficacy of this novel device.
Impact on daily practice
Despite the many endovascular treatment options for femoropopliteal lesions, the main limitation of endovascular treatment modalities is the high rate of recurrent lesions necessitating repeat interventions and reduction in restenosis rates as femoropopliteal angioplasty remains to be of high interest among the peripheral intervention community. It appears that this can be accomplished with the “leave nothing or little behind” strategy. While “bailout” stenting is widely accepted in case of suboptimal or failed result from balloon dilation (e.g. residual diameter stenosis >30%, or flow-limiting dissection), no or little disturbance of the overall biomechanical properties in the stented segment seem to be of paramount importance. Our experience demonstrates that the novel MSDS (“Multi-LOC”) is a safe and efficacious device for femoropopliteal spot stenting with the advantage of releasing up to six short stents without changing the delivery system.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Klaus Amendt received lecture fees and travel support from B. Braun Melsungen AG and Biotronik SE & Co. KG. Johannes Jung was the managing director for the manufacture of the “Multi-LOC” device used. Heinz Kölble was the managing director of Endoscout GmbH, distribution partner for the manufacturer. Dr. Klaus Amendt, Johannes Jung, and Heinz Kölble are co-inventors of a patent application for the “Multi-LOC” device used in this study. Dr. Martin Sigl has no conflicts of interest to declare.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval for this study was obtained from the responsible local ethics committee (Medizinische Ethik-Kommission II of the Ruprecht-Karls-Universität Heidelberg, ID 2015-411M-MA-§23b MPG).
Guarantor
Klaus Amendt guarantees the work.
Contributorship
MS analysed and interpreted data and wrote the manuscript; JJ interpreted data and revised the manuscript; HK interpreted data and revised the manuscript; KA analysed and interpreted data, created figures, and revised the manuscript; All authors approved the version to be published.
Informed consent
Written informed consent was obtained from all subjects before the study.
Trial registration
This pilot study was not registered. Based on this data, the LOCOMOTIVE—all comers registry was established (ClinicalTrials.gov identifier: NCT02531230).