
Abstract
Aim
Conversion to open repair becomes the last option in case of endovascular repair of abdominal aneurysm failure, when radiological interventional procedures are unfeasible. While early conversion to open repair generally derives from technical errors, aetiopathogenesis and results of late conversion to open repair often remain unclear.
Methods
We report data from our Institute’s experience on late conversion to open repair. Twenty-two late conversion to open repairs out of 435 consecutive patients treated during a 18 years period, plus two endovascular repair of abdominal aneurysms performed in other centres, are analysed. The indication for conversion to open repair was aneurysm enlargement because of type I, type III, type II endoleak and endotension. Even if seven cases (23%) had shown an initial aneurysmal shrinkage, in a later phase, the sac began to enlarge again. In 12 patients, conversion to open repair was the last chance after unsuccessful secondary endovascular procedures.
Results
Three cases (12.5%) were treated in emergency. Aortic cross-clamping was only infrarenal in 10 cases, only or temporarily suprarenal in 14 and temporarily supraceliac in 9 cases, for 19 total and 5 partial endograft excisions. Two patients died for Multiple Organ Failure (MOF), on 42nd (endovascular repair of abdominal aneurysm infection) and 66th postoperative day. No other conversion to open repair-related deaths or major complications were revealed by follow-up post-conversion to open repair (mean: 68 months ranging from 24 to 180 months).
Conclusion
Late conversion to open repair is often an unpredictable event. It represents a technical challenge: specifically, the most critical point is the proximal aortic clamping that often temporarily excludes the renal circulation. In our series, conversion to open repair can be performed with a low rate of complications. In response to an endovascular repair of abdominal aneurysm failure, before applying complex procedures of endovascular treatment, conversion to open repair should be taken into account.
Introduction
Since its birth, endovascular repair of abdominal aneurysm (EVAR) is associated with a high rate of secondary interventions up to 15%.1,2 The majority of these treatments are still endovascular. Conversion to open repair (COR), considered at higher risk than an aneurysm open primary repair, 3 becomes the last option for those patients where more radiological procedures are unsafe or unfeasible. In a recent review, Kouvleos et al. have found the cumulative single centre rate of late COR nearly to 4% (ranging from 0.9 to 22.8%). 4 Even though early COR (performed <30 days after EVAR) generally derives from technical errors in planning or during EVAR, aetiopathogenesis of late COR often remains unclear as well as its results. The aim of this study is to analyse 22 late conversions (in terms of indication operative details and outcomes) in our series of 435 consecutive patients treated with EVAR during a 18 years period, plus two cases of EVAR performed in other vascular centres.
Methods
Data of all our 435 EVARs were prospectively collected in a database during the period from 1997 to 2015. In this database, we recorded the main demographic data, comorbidities of each patient, measures for planning, type of endograft used and duration of implant. We also collected postoperative follow-up: timing and reasons for any other procedures, possible COR with relative operative details, mortality and major morbidity. Follow-up schedule consisted of a physical examination and an AngioCT scan performed after 1 month in the early period; then of a colour duplex scan every 6 months. If type II endoleak is still present at the operating room discharge or a new onset occurs during the follow-up, we prefer to individualize subsequent checks by using AngioCT or contrast-enhanced US.
The complications predictive of EVAR failure were investigated with AngioCT scan. Endovascular procedures were always considered as the first therapeutic approach: we chose between selective embolization and/or proximal/distal neck relining, whilst we never used FEVAR, BEVAR or chimney/snorkel or other already proposed techniques. In some cases, laparoscopic ligation of inferior mesenteric artery was performed. COR was performed if no secondary endovascular procedures were feasible or after their prior failure. Indications for COR resulted the following: onset of type I or III endoleak, sac enlargement >5–7 mm with or without endoleak evidence, radiological evidence of ruptured aneurysm or graft infection. COR was defined urgent if performed less than 24 h after revealing the problem, while it was defined elective COR if performed after that time. Out of that database, we retrospectively analysed 22 patients treated with COR (5% out of our 435 EVAR). Additionally, we studied the available history of two patients undergoing EVAR in other centres. All 24 cases underwent late COR with graft removal >30 days after EVAR: two other patients were excluded from the study because they were early CORs. Every patient’s physical status was assessed according to American Society of Anaesthesiologist score (ASA).
Within operative details, we evaluated the kind of surgical approach performed, position and duration of the proximal aortic cross-clamping, total or partial graft explanation (conversion vs. semi-conversion). Post-operative variables included major perioperative (30 days) morbidity and mortality. Major complications were recorded and defined per SVS/VQI reporting guidelines 5 . Acute kidney injury (AKI) and acute renal failure (ARF) were based on the RIFLE (Risk, Injury, Failure, Loss and End staged kidney disease) criteria. 6
Results
Population
Mean age of the 24 patients undergoing conversion to OR was 75 (ranging from 48 to 79) (Table 1). Graft explanation was performed after an average of 49 months (IQR 27–70). The time course between EVAR and COR proved to be totally unpredictable. Clinical history of each patient is clearly explained in the three graphics presented (Figures 1 to 3). Demographic data and risk factor are shown in Table 1. The majority of patients had an ASA score ≥III due primarily to their cardiovascular comorbidity. Four patients were affected by chronic renal insufficiency.
Demographic characteristics and risk factors of the population analysed.

IQR: interquartile range; ASA: American Society of Anaesthesiologist.
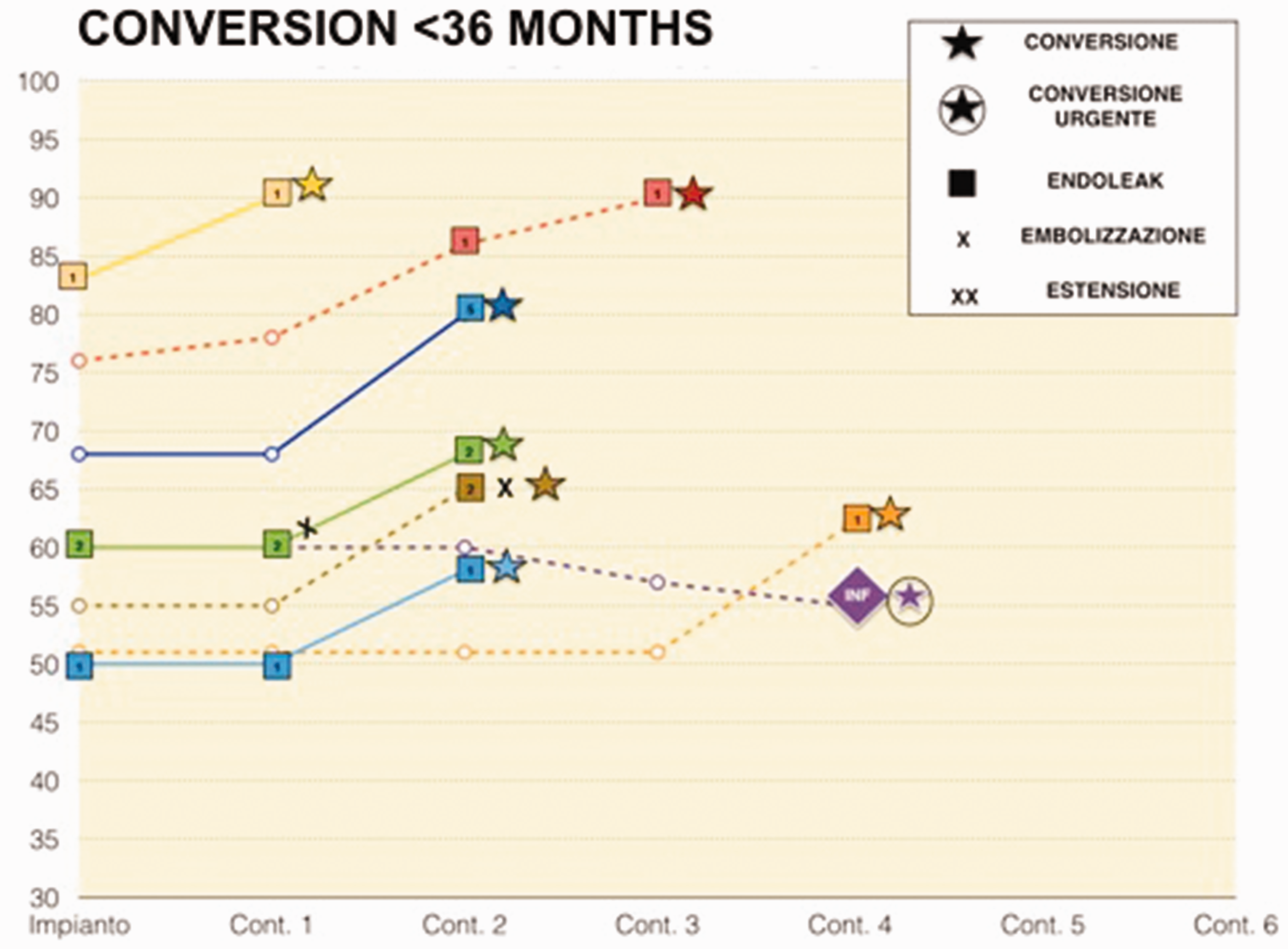
Clinical history: relation between time and diameter of sac patients underwent ROC Conversion to Open Repair < 36 months.
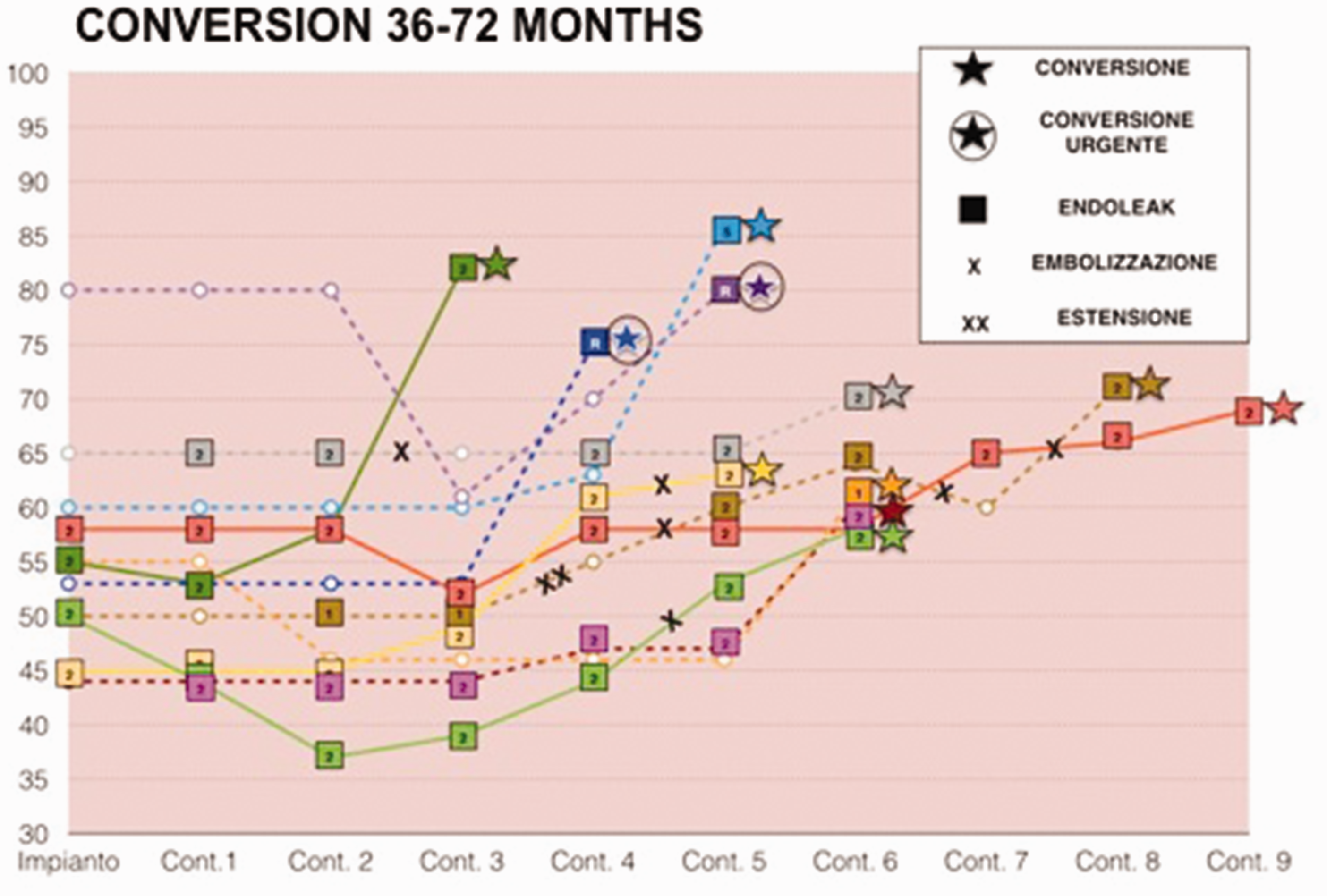
Clinical history: relation between time and diameter of sac patients underwent ROC 36–72 months.

Clinical history: relation between time and diameter of sac patients underwent ROC > 72 months.
Graft, previous treatment and follow-up
The types of the converted stent grafts were Talent (Medtronic, Minneapolis, MN) in 54% patients, followed by Excluder (W.L. Gore & Ass. Flagstaff, AZ) and Endurant (Medtronic, Minneapolis, MN) with 17% both, Aneurx (Medtronic, Santa Rosa, CA) were explanted in 12% of cases. So fixation was suprarenal in 71% and infrarenal in 29% of patients. In our overall series, we used mainly suprarenal fixing (270/435, 62%). The 22 patients treated in our Institute were scheduled on average for 5 ± 3 controls before OR. Before COR, seven cases (23%) had shown an initial shrinkage of the aneurysmal sac, while 12 patients had undergone at least one secondary procedure to treat the endoleak (Table 2): two had undergone laparoscopic inferior mesenteric artery ligature, one an iliac extension and six successful lumbar embolization, while three other endovascular procedures of lumbar closure failed. There were no follow-up details for the two patients who underwent the EVAR procedure in other centres.
Details of ROC causes and surgical details of 24 ROC.

Indications
The most frequent indication for COR was type I endoleak with (n = 10). Other indications included type III (three cases) and persistent type II, with an aneurysmal sac enlargement of at least 5 mm (seven cases). We also found two cases of endotension. Therefore, the overall indication for endoleak was about 96%. The last case was one infection with aorto-enteric fistula (Table 2). Overall, three cases (12.5%) were treated in emergency settings: the infected EVAR and two aortic ruptures for type I B endoleak and type III, respectively. Notable, both aortic ruptures occurred after regular follow-up checks, with no signs of major complications until that event.
Operative details
We chose a midline abdominal incision in 23/24 patients and one bilateral sub-costal incision in a great obese patient. Aortic cross clamping was suprarenal in 14 patients and infrarenal in 10 patients (58% and 42%, respectively); in nine cases, a temporary (7–15 min) supraceliac clamping was necessary. The EVAR infection associated to an aorto-duodenal fistula was urgently treated with total endoprothesis explanation, aorto-bisiliac substitution using silver coated Dacron and a duodenal resection. Partial explanation of stent graft was performed in five cases with supra renal fixing (21%), while total excision was preferred in 19 cases (Table 2).
Patients’ outcome
Two patients died for multiple organ failure: one died 42 days after having undergone urgent procedure for graft infection and aorto-duodenal fistula, and one died 66 days after elective treatment. We also observed one non-lethal myocardial infarction, one mild stroke and five cases of mild renal impairment (with one case of renal artery thrombosis), with no cases of permanent haemodialysis. After a mean follow-up of 68 months, we have an overall survival of 79%; however, the subsequent deaths were not COR related.
Discussion
Although EVAR is a less invasive technique with good short-term results compared to traditional open repair, long-term follow-up data have confirmed the need for continued surveillance and secondary interventions to achieve a complete exclusion. The rate of secondary interventions varies depending on several factors (such as correct planning, centre’s experience, type of device used) and it can reach up to 15%.3,4,7–9 The majority of these procedures are endovascular, but very often they involve complex endovascular techniques without clear results and late follow-up.10–13 However, open conversion after EVAR represents the ‘last chance’ in case of failure of less invasive techniques, although it is considered to be more demanding compared to primary open surgical repair. A recent review 4 shows a COR after EVAR rate ranging from 1% to 22% with an average of 3.7%. Our institute has an OR rate of 5% and the time of explants occurs, on average, more than 4 years after the EVAR procedure. As reported in the literature, in our series, the main cause of conversion is represented by endoleaks, in particular of type I. Although the management of this complication contemplates increasing endovascular salvage technique, elective COR can be technically challenging but associated with good results. Recently, in particular, Scali et al. showed that COR for type I endoleak is not associated with increased morbidity or mortality when compared to pararenal aneurism open repair. 14 We think that this kind of defect must be aggressively treated despite of some reported experience of spontaneous delayed sealing. 15 The second cause of conversion and the first complication after EVAR is type II endoleak, which is the most frequent complication after EVAR. 16 It represents a very disturbing problem because these patients, during their clinical history, must be repeatedly subject to several procedures such as embolization of inferior mesenteric artery or lumbar arteries, or laparoscopic ligation of mesenteric artery without definitive results. The nature and evolution of this endoleak remain obscure events that can be assumed as a generic marker of negative prognosis after EVAR.17–19 In our Institute, we perform(ed?) a definitive elective treatment when type II endoleak persisted over a 12 months period or pulsatile sac enlargement > 5 mm was detected during a 6 months period. Several studies in literature consider sac shrinkage as a marker of successful EVAR. In particular, it could be expected that patients who have significant reduction in sac diameter during early post-operative period would experience less complications.20–23 Despite these considerations, in our study, we experienced several cases of ‘anarchic’ follow-up, in particular we are eager to highlight two phenomena: the occurrence of one unexpected type III endoleak that required an emergent treatment after a regular follow-up and seven COR for sac enlargement despite an initial good shrinkage.
Literature shows that endoprothesis with infrarenal fixing are more likely to be explanted? 4 This is in discordance with our experience, because we removed 71% of stent graft with suprarenal fixing; however, this could be the result of the large use of these devices in our experience (overall, 62% of 435 patient treated).
Late conversion after EVAR can be accomplished with complete explantation or partial preservation of the endoprothesis. In our series, in 79% of cases, the stent graft could be completely removed. Control of the aorta above the proximal fixation site is of utmost importance for a safe endoprothesis removal. In most cases, suprarenal aortic clamping was safe enough, when the fixation of the endograft was infrarenal, but also when a graft with a suprarenal fixation had migrated caudally. When endograft is still suprarenal, temporary supraceliac aortic cross clamping is the best option in order to achieve a good aortic control and to avoid injuries to the native aorta and the renal arteries during semiconversion,24,25 which has to be considered the first technical choice in case of ‘active’ suprarenal fixations. The same advice is recommended during the removal of suprarenal bare stent without barbs or hooks. Eventually, it could be useful to perform the external Teflon stripes reinforcement of the anastomosis between native vessels and open graft.
In conclusion, late open conversion after EVAR remains challenging; however, it can be performed with good results compared. Nowadays, consolidated in high volume centres for the open repair of juxtarenal aneurysm. In case of EVAR failure, these results should be taken into account before performing complex endovascular treatments.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
None.
Guarantor
None.
Contributorship
None.