
Abstract
Background
The paucity of data regarding the association between atherogenic index of plasma and risk of cardiovascular disease in HIV-infected populations living in sub-Saharan Africa prompted us to conduct this study which aimed to assess the relationship between atherogenic index of plasma and risk of cardiovascular disease among a Cameroonian HIV-infected population.
Methods
This was a cross-sectional study conducted among 452 HIV-infected adults in Yaoundé, Cameroon. Risk of cardiovascular disease was calculated using the Framingham risk score; atherogenic index of plasma was derived as log (triglycerides/high-density lipoproteins cholesterol).
Results
Participants’ mean age (80% females) was 44.4 ± 9.8 years. Atherogenic index of plasma values ranged from –0.63 to 1.36 with a median of 0.11 (25th–75th percentiles: –0.08-0.31). Most participants (88.5%) were on antiretroviral treatment. There was a significant correlation between atherogenic index of plasma and fasting plasma glucose (r = 0.116; p = 0.014), atherogenic index of plasma and total cholesterol (r = –0.164; p < 0.001). Atherogenic index of plasma was significantly associated with the risk of cardiovascular disease either in univariable (β = 5.05, 95% CI: 3.31–6.79; p < 0.001, R2 = 0.067) or in multivariable linear regression model after adjusting for socio-demographic, clinical and biological confounders (adjusted β = 3.79, 95% CI: 1.65 – 4.88; p < 0.001, R2 = 0.187).
Conclusion
Atherogenic index of plasma may be an independent factor impacting the risk of cardiovascular disease among Cameroonian HIV-infected people. More studies are needed to better elucidate the association between atherogenic index of plasma and risk of cardiovascular disease in our setting.
Introduction
The human immunodeficiency virus (HIV) infection remains a critical cause of illness and death worldwide. 1 During the year 2015 for instance, 2.1 million people became newly infected, completing to 38.7 million the number of people living with the HIV globally. 1 There is no doubt nonetheless that the introduction and widespread use of continuous antiretroviral therapy (ART) has drastically changed the HIV-related paradigm, as HIV-infected people live longer and better; 1 however, this is not without any drawback effect. Evidence has indeed accumulated an increased incidence of cardiovascular disease (CVD) and its main risk factors, especially hypertension, diabetes and lipid disorders among HIV-infected persons.2–4 This HIV-induced burden of CVD adds to the current epidemic proportions of CVD in the global general population. 5
In comparison to the conventional lipid profile, serum lipid ratios such as total cholesterol/high-density lipoprotein-cholesterol (TC/HDL-C), low-density lipoprotein-cholesterol (LDL-C)/HDL-C and triglycerides (TG)/HDL-C have been shown to be better predictors of CVD. 6 Further, atherogenic index of plasma (AIP), defined as the logarithmically transformed ratio of TG to HDL-C, 7 has been presented as a superior predictor of CVD than the previous lipid parameters.6,8–10 This could be truer in the HIV-infected population, considering very high rates of lipid disorders in this vulnerable group.8,11,12 Additionally, HDL-C and triglycerides correlate strongly with insulin resistance; which itself is known to be related to ART, advocating for the high relevance of AIP for CVD risk prediction in HIV-infected people.13,14 However, how AIP influences the risk of CVD has poorly been studied in this particular population.
Given that the best way of tackling the epidemic of CVD is primary prevention of risk factors alongside the understanding of how they interact with each other, and considering a dire lack of data, we conducted the present study to assess the association between AIP and other CVD risk factors and how AIP impacts the global risk of CVD among a group of black African HIV-infected patients.
Methods
Study design and setting
This was a cross-sectional study carried out from December 2015 to May 2016 at the HIV day-care unit of the Yaoundé Central Hospital in the Capital City of Cameroon. This is one of the most important HIV clinics in the country. Blood samples were analyzed at the biochemistry laboratory of the Yaoundé University Teaching Hospital, Cameroon. The study was approved by the Cameroon National Ethics Committee for Human Health Research (Ethical approval N° 2015/12/710/CE/CNERSH/SP). Administrative approvals were obtained from authorities of the Yaoundé Central Hospital and the Yaoundé University Teaching Hospital. Participants who provided a signed informed consent form after receiving all information on the study were included.
Participants
All HIV-infected patients reporting for follow-up visits at the HIV clinic of the Yaoundé Central Hospital were approached for their enrollment in the study. Consenting participants were included if they were aged 30 to 74 years, had no history of CVD, were not pregnant or breastfeeding women, were not on lipid-modifying therapy or hormone therapy and were clinically stable.
Data collection
A structured pretested interviewer questionnaire and medical files of participants were used for data collection on socio-demographic characteristics, history of HIV infection and cardiovascular risk factors (hypertension and diabetes). Family history of CVD was defined as CVD in a first-degree relative before the age of 55 years for men or 65 years for women. 15 Smoking status was classified as never, former or current (those who had stopped smoking within the past 12 months were considered current smokers), sedentary lifestyle was defined as absence of physical activity (walking, intense physical activity) at least once a week. 16 Alcohol consumption was access using the Alcohol Use Disorders Identification Test-Consumption (AUDIT-C) score and Hazardous alcohol drinking was defined by a value ≥4 for men and ≥3 for women. 17
Anthropometric parameters and blood pressure of all participants were measured during physical examination. Height was measured to the nearest 0.1 cm, using a stadiometer. Weight was measured to the nearest 0.1 kg, using an electronic scale (CAMRY, Hong Kong, China). Body mass index (BMI) was derived as weight (kg)/height∗height (m2), and participants grouped as underweight (<18.5), normal (18.5–24.9), overweight (25.0–29.9) or obese (≥30.0). 18 Waist circumference and hip circumference were measured to the nearest 0.1 cm using a measuring tape. Both parameters were used to calculate the waist-to-hip ratio (WHR). Abdominal obesity was defined in accordance with the International Diabetes Federation (IDF) criteria (waist circumference >90 cm for men and >80 cm for women). 19 Blood pressure was measured using an electronic device (Omron M5-1, Omron Healthcare, Kyoto, Japan). High blood pressure was defined as a systolic blood pressure (SBP) ≥140 mmHg and/or a diastolic blood pressure (DBP) ≥90 and/or self-reported history of antihypertensive medication. 20
Blood collection and biochemical assays
Blood sample of each participant was aseptically collected on the day of appointment, after a 12-h overnight fasting, by venipuncture of the brachial vein in a 5 mL sodium fluoride tube and a 5-mL dry tube. Samples were placed on ice (4°C) and immediately transported to the biochemistry laboratory where plasma and serum specimen were separated by centrifugation at 3.000 r/min for immediate analyses. We used standard colorimetric procedures to assay fasting plasma glucose (FPG), TC, TG and HDL-C. LDL-C was subsequently calculated when the TG level was equal or below 4 mmol/L using the Friedewald formula and assayed trough standard colorimetric procedures when TG levels were over 4 mmol/L. 21
Diabetes was defined by an FPG ≥7.0 mmol/L at two occasions within at least 48 h, or self-reported history of diabetes or used of antidiabetes medications. 22 The atherogenic index of plasma (AIP) was calculated as the common logarithm base ten (log) transformed ratio of molar concentrations of TG to HDL-C. 8 The risk was categorized into low (<0.1), intermediate (0.1–0.24) and high (>0.24). 23
Cardiovascular risk assessment
The 10-year CVD risk of each participant was calculated using the general Anderson-Framingham CVD risk equation. The Framingham equation estimates CVD risk through a combination of age, sex, SBP, antihypertensive therapy (yes or no), serum TC and HDL-cholesterol values, current smoking status (yes or no) and diabetes (yes or no)). 24 Participants were subsequently grouped into three classes, given they presented a low risk (score <10%), a moderate risk (score 10–20%) or a high risk of CVD (score >20%). 24
Statistical analysis
Data were coded, entered and analyzed using IBM Statistical Package for Social Sciences (SPSS) version 23.0. (IBM Corporation, United States of America). Results are presented as frequency (percentage) for categorical variables, and mean ± standard deviation (SD) or median (25th–75th percentiles) for continuous variables where appropriate. Non-parametric tests were used to compare continuous variables between groups and Chi-square test for categorical variables. The association between two continuous variables was assessed using Pearson correlation coefficient (r). Further, univariable and multivariable linear regression analyses were undertaken to investigate the interplay between the risk of CVD and other parameters including AIP. We introduced in the multivariable model all variables with a p value <0.25 in the univariable model, in addition to the AIP, regardless of its p value obtained in univariable analysis, followed by backward elimination to retain the final significant predictors in the model. A p value <0.05 was used to characterize statistically significant results.
Results
We recruited 452 participants (361 women, 80%); their ages varied between 30 and 74 years, with a mean age of 44.0 ± 10 years. Four hundred participants (88.5%) were on ART. Nine participants (2.0%) had diabetes and 60 (13.3%) had hypertension. Twenty-seven participants (6.0%) were active smokers; 251 (55.5%) did not report regular physical activity and 88 (19.5%) had obesity (Table 1).
Distribution of clinical and biochemical parameters.
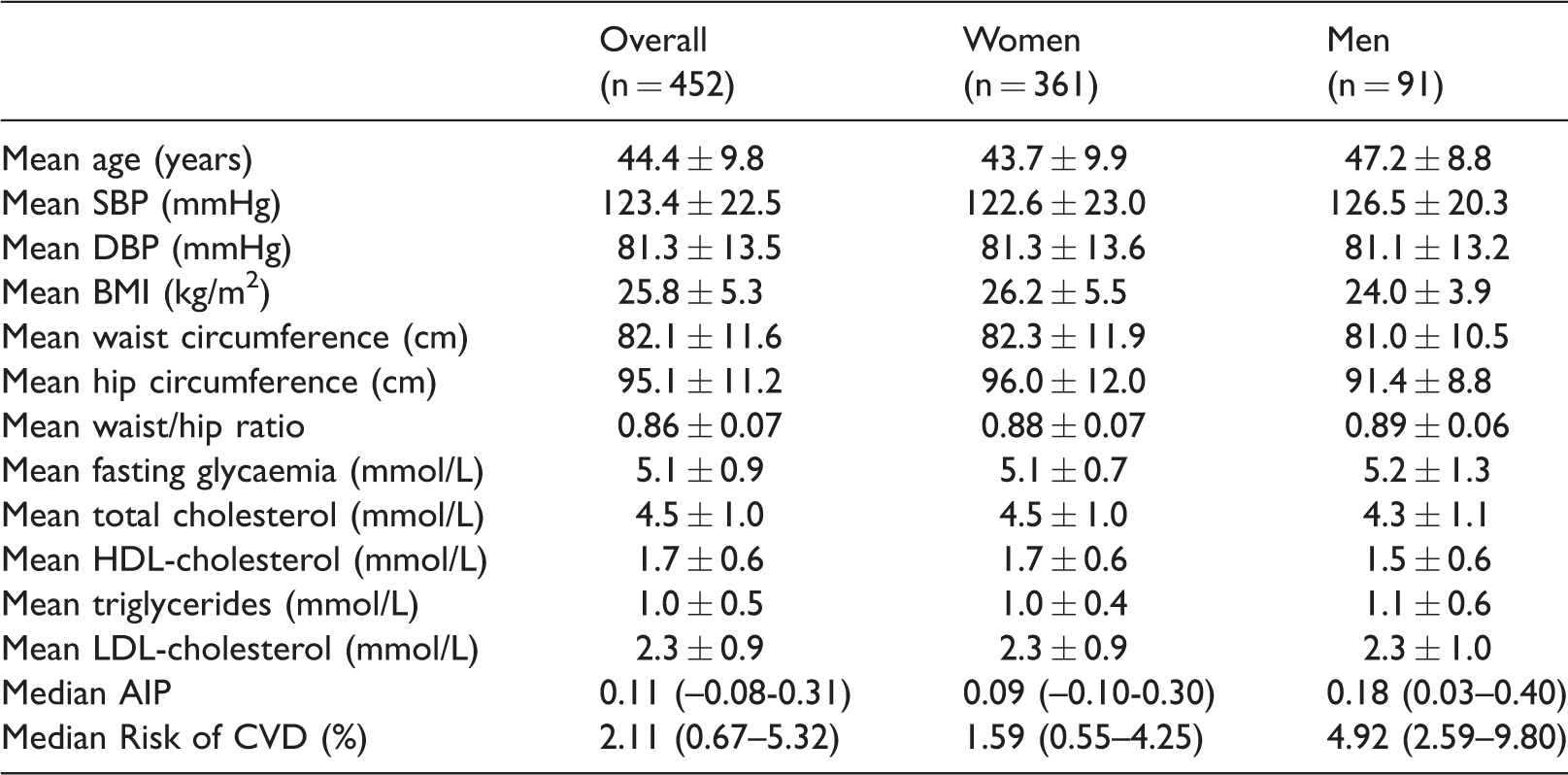
Data presentation: Mean ± standard deviation, Median (25th–75th percentiles).
BMI: body mass index; DBP: diastolic blood pressure; SBP: systolic blood pressure; FPG: fasting plasma glucose; TC: Total Cholesterol; LDL-C: low-density lipoproteins cholesterol; HDL-C: high-density lipoproteins cholesterol; VLDL-C: very low-density lipoproteins cholesterol; AIP: atherogenic index of plasma.
The distribution of various clinical and biological variables measured is depicted in Table 1. AIP values ranged from –0.63 to 1.36, with a median of 0.11 (-0.08 -0.31). Two hundred and fifteen participants (47.6%) had a low AIP, 90 (19.9%) had a moderate AIP and 147 (32.5%) had a high AIP. The median AIP was lower in participants on ART than in their counterparts (0.09 vs 0.25, p = 0.002). However, AIP values did not vary significantly with regard to known diabetes (p = 0.178), known hypertension (p = 0.488), active smoking (p = 0.998), regular physical activity (p = 0.158), obesity (p = 0.989) and hazardous alcohol consumption (0.904).
There was a significant correlation between AIP and FPG (r = 0.116; p = 0.014), AIP and AUDIT-C score (r = 0.115; p = 0.014), LDL-C (r = 0.108; p = 0.022) and between AIP and TC (r = –0.164; p < 0.001), though these correlations were weak (Table 2).
Correlation between the atherogenic index of plasma (AIP) and other variables.

BMI: body mass index; DBP: diastolic blood pressure; SBP: systolic blood pressure; FPG: fasting plasma glucose; TC: Total Cholesterol; LDL-C: low-density lipoproteins cholesterol.
The 10-year risk of cardiovascular events based on the FRS varied between 0.02% and 38.47%, with a median of 2.11 (0.67–5.32). Three hundred and ninety-four participants (87.2%) had a low risk of CVD, 42 (9.3%) had a moderate risk and 16 (3.5%) had a high risk of CVD.
There was a significant relation between the FRS (as the dependent variable) and the AIP in univariable linear regression (β = 5.05, 95% confidence interval (CI): 3.31–6.79; p < 0.001, R2 = 0.067); there was also a significant relationship between categorized risk of CVD and categorized AIP (p = 0.043; Table 3).
Categorized risk of cardiovascular disease (CVD) and AIP (p = 0.043).

Furthermore, in multivariable linear regression analysis after adjusting for socio-demographic factors (occupation, level of education), clinical factors (waist circumference, hip circumference, duration of HIV infection) and other biological factors (CD4 count, LDL-C), the relationship between AIP and the risk of CVD remained significant (adjusted β = 3.79, 95% CI: 1.65–4.88; p < 0.001, R2 = 0.187; Table 4). Occupation, waist circumference, hip circumference and LDL-C were other independent factors impacting our participants’ risk of CVD.
Relationship between risk of CVD, AIP and others factors.

AIP: atherogenic index of plasma; Β: regression coefficient; CVD: cardiovascular disease; ART: antiretroviral therapy; LDL: low density lipoproteins.
Discussion
In this study carried out in an HIV-infected black African population, we found that there is a significant association between AIP and the 10-year risk of CVD either in univariable analysis or in multivariable analysis after adjusting for confounders.
AIP was globally higher in our study population than in the general non-HIV-infected population (32.5% high AIP vs 25% high AIP) 25 ; these results can be explained by the fact that HIV infection and ART are well-known risks of metabolic complications and thus likely predispose HIV patients to an increased risk of dyslipidemia and its correlates. 26 However, the median values of AIP were lower in our study than values obtained by Onyedum et al. 27 in an HIV-infected population in Nigeria despite the fact that their study population was solely made of ART-naïve patients 0.11 (interquartile range: –0.23) vs 0.30 (interquartile range: 0.60). We do not have a clear explanation of this finding, as we would have expected AIP levels to be higher in our study population due to the fact that more than half of our study population was on ART. Moreover, in our study, the median AIP was lower in participants on ART than in their counterparts (0.09 vs 0.25, p = 0.002) despite a mean duration of ART of 72 months (25th–75th percentiles: 35–108). All these facts are suggestive of a possible relationship between ART and reduction in AIP, but we are in need of further investigations to better assess the interplay between AIP and ART.
The AIP was significantly correlated with FPG, AUDIT-score, LDL-C and TC but not with age, SBP and BMI. Except for LDL-C, which was also reported to be significantly correlated with AIP in other HIV-infected populations, 27 our findings differed from results reported by many other studies. Indeed, physical activity, waist circumference and BMI were reported as factors significantly correlated with AIP by Niroumand et al. 14 who worked in the general population, for the specific case of HIV-infected persons, CD4 count, BMI and LDL-C were reported associated with AIP.27,28 The correlation between AIP and TC was negative; further studies are warranted to clearly elucidate the relation between these two parameters among HIV-infected patients as we did not find any clear reason to justify what we observed.
The 10-year risk of cardiovascular events assessed using the Framingham risk equation was significantly associated with the AIP in univariable analysis and after adjusting for socio-demographic, clinical and biological confounders in multivariable analysis. Occupation, waist circumference, hip circumference and LDL-C were other independent factors impacting our participants’ risk of CVD. These findings were similar to results reported in the general population, suggesting the use of AIP to assess cardiovascular risk events because of its high correlation with many traditional cardiovascular risk factors and risk estimators of CVD.14,29 Nevertheless, they are different from results reported by Nansseu et al. 30 in a Cameroonian population of postmenopausal women. Indeed, they did not find a significant relationship between AIP and risk of CVD and explained their findings by limitations of their study. 30
Our study presents some limitations. First, the cross-sectional design of this study precludes us from concluding on the predictive nature of factors identified significantly associated with AIP or CVD risk. Second, our sampling method was not random and we recruited our patients from only one site, which could be a source of bias hampering perhaps the translatability of our findings to the entire Cameroonian HIV-infected population. Third, in the absence of locally-developed tools to assess the cardiovascular risk, we used the FRS which may lack to accurately assess the cardiovascular risk in African populations as they may present different patterns of CVD when compared with that of developed countries.14,29 Notwithstanding these limitations, our sample size was relatively high and we used rigorous methodological and statistical procedures to carefully assess our research questions.
Conclusion
This study conducted among 452 HIV-infected Cameroonian patients showed a significant correlation between the atherogenic index of plasma (AIP) and FPG, LDL-C, AUDIT-score and TC. AIP was an independent factor impacting the risk of CVD. However, more studies are needed to better elucidate the interplay between AIP and risk of CVD in our settings and could finally lead to the development of a CVD risk equation for HIV-infected population including AIP.
Footnotes
Acknowledgments
We thank all the physicians and professional nurses of the HIV out-patient clinic of the Yaoundé Central Hospital for their assistance during recruitment and the personnel of the biochemistry laboratory of the Yaoundé University Teaching Hospital for their assistance during biochemical measurements. We are also grateful to all those who have voluntarily accepted to take part in this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the Cameroon National Ethics Committee for Human Health Research (Ethical approval N° 2015/12/710/CE/CNERSH/SP). All participants singed a consent form.
Guarantor
SRN is the guarantor for this study.
Contributorship
Conception and design: SRN, JRN, JJB; Participant recruitment and data collection: SRN; Data analysis: SRN, JRN, JJB; Manuscript drafting: SRN, JRN JJB; Manuscript revision: ES, APK, MYD, JJB, JRN, VJAM, FKA; Approved the final version of the manuscript: All authors.
Original publication
This manuscript is not under consideration by any other journal, and it has not already been published in any journal.