
Abstract
Background
In this study, we aimed to review the consequences of coronary endarterectomy with coronary artery bypass grafting, and assess outcomes of this combined surgical technique for patients with diffuse coronary artery disease in a single surgeon’s practice.
Methods
We retrospectively reviewed outcome of 1198 endarterectomized coronary artery in 1000 patients with diffuse coronary artery disease, who have had experienced coronary endarterectomy with off pump coronary artery bypass grafting in between 2009 and 2016.
Results
The mean age was 61.5 ± 5.5 years. Coronary endarterectomy was performed on 74.7% in the left coronary territory (43.2% left anterior descending, 26.6% diagonal, 4.9% Obtuse Marginal), and 25.3% in the right coronary territory. Post-operative intensive care unit mortality rate was 1.9%, and there were 11 (1.1%) late deaths. Mean intensive care unit stay was 36.6 ± 6.7 hours. Patients were extubated following a mean of 9.8 ± 1.25 hours. The mean duration of hospital stay was 10 ± 1 days. One-year survival rate was 97.8% and 89.5% survival rate was at 5 years follow up. However, 91.8% of patients were angina free at median follow-up of 2.5 years.
Conclusion
Coronary endarterectomy with off pump coronary artery bypass grafting is attainable and accomplishes surgical revascularization in coronary artery disease patients when there is no other alternative for sufficient revascularization.
Introduction
Ischemic heart disease (IHD) patients, who are referred for coronary artery bypass graft (CABG), are increasingly getting more complex with multiple comorbidities, such as hypertension, diabetes, renal impairment and peripheral artery disease. A large proportion of these patients also have presented with history of previously undergone coronary intervention and angioplasty. Subsequently, atherosclerotic process has progressed in this group of patients and developed diffuse coronary artery disease (CAD), making complete surgical revascularization highly challenging.
In 1957, coronary endarterectomy (CE) was first reported by Bailey et al. 1 as a surgical option for myocardial revascularization. This procedure involves the expulsion of the atheromatous plaque, dismembering and isolating the outer media and adventitia layers. CE is frequently performed during CABG in order to achieve total myocardial revascularization or used to facilitate anastomosis of severely calcified and diffusely diseased coronary arteries. In the case of diffuse CAD, conventional CABG does not provide a satisfactory blood supply through the distal parts of coronary vessels. 1 The consequence of inadequate myocardial revascularization does not influence the early mortality rates, but influences the rate of native vessel restenosis that ultimately leads to long-term cardiac dysfunction. These patients have been shown to have greater risk of recurrent angina attacks, poorer stress test performance, repeat interventions following CABG and higher rate of absence from work.2–5
This study aimed to assess the outcome of CE with off pump CABG (OPCABG) in a single surgeon’s practice and to provide details regarding our treatment strategies for patients experiencing diffuse CAD.
Methods
In between 2009 and 2016, 1000 patients were submitted to CE with CABG in a single surgeon’s practice (Figure 1). During this study, every patient was approached during outpatient department visit or by telephone and data were gathered by questionnaire. Outcomes variables of study population were survival rate, post-operative cardiovascular and neurological events, post-operative myocardial infarct (MI), re-intervention, hemodynamic instability, NYHA class and Canadian class for angina.

Bar diagram illustrate number of patients undergone coronary endarterectomy in each year from 2009 to 2016.
Coronary endarterectomy technique
Standard intra-operative monitoring strategies were utilized and a cardiopulmonary bypass (CPB) circuit was kept on standby for all cases. All procedures were performed through a standard median sternotomy. Heparin was used to maintain an activated clotting time more than 400 seconds during harvesting of conduits (internal mammary artery, the saphenous vein and sometimes radial artery). Almost all the operations were performed using OPCABG procedure except in a few cases where the assistance of CPB was required. We utilized mechanical stabilizers such as suction type and the compression type to immobilize the target coronary artery during grafting. A conclusive decision to endarterectomize a vessel was made per-operatively and CE was considered when localized lesion blocked a sufficient distal stream (i.e. complete occlusion), distal diffuse lesion or multi-segmental lesion, as well as when a calcified or extremely thick plaque burst, making anastomosis troublesome or hindering the stream.
Coronary endarterectomies were performed manually by slow sustain and continuous traction of atheromatous plaque with the aid of delicate Ring Forceps, utilizing the closed methods trailed by reproduction with anastomosis with pre-planned graft. The arteriotomy incision was approximately 8–10 mm long, but could be stretched out for another 5 mm in some cases, if complete removal of the plaque was not feasible. Exceptionally sensitive ring forceps (Figure 3) were utilized to build up a plane between the media and the atherosclerotic plaque. With slow sustain and continuous traction, the plaque removal was attempted, with the assistance of another ring forceps (counter traction), facilitating the expulsion of the biggest portion of plaque. Close consideration was paid to the entire expulsion of the distal segment; proximal traction of the plaque was avoided usually in the interventricular artery because of the danger of proximal dissection and the impediment of a wide septal branch, oblique branches or even of the circumflex artery. Subsequently, to finish distal anastomosis incision in the conduits was extended to coordinate the arteriotomy, with the exception of few situations where venous patch was utilized. In this study, complete proximal endarterectomy was avoided due to the possibility of competitive flow loss between the graft and native artery. To ensure complete expulsion, the atheromatous plaque was carefully inspected for a smooth distal tapper end. In addition, back flow of blood from the distal vessel following extraction of the atheroma is a consoling indication of adequate removal of atheromatous plaque and that is a special feature in OPCABG endarterectomy. In our study, longest atheroma (14 cm) was removed from right coronary artery (RCA) and also another 10-cm atheromatous plaque extracted from left anterior descending (LAD) coronary artery during OPCABG (Figure 4).
Every patient was monitored in intensive care unit (ICU) for close observation and management. In early post-operative period, patient was treated with heparin (usually 2–3 hours following surgery) bridging to warfarin from the first post-operative day to the next 3–6 months. A combination of Clopidogrel with Aspirin was given orally at the dose of 75 mg o.d. for both drugs to prevent acute thrombosis within the graft as well as the endarterectomized artery. Warfarin was typically started at 10 mg daily for first three post-operative days followed by 2.5–5 mg for next 3 to 6 months with the dose adjusted according to INR level (our local targeted INR was 1.5–2.5).
Results
About twelve hundred CE were performed in one thousands patients; that is 9.9% of our study population required multiple coronary endarterectomy. The mean age was 61.5 ± 5.5 years and 78.2% were male patients. Most common risk factors associated with CAD were HTN (82.1%), dyslipidemia (76.5%) and smoking (71.9%). About two-third of study population has past medical history of myocardial ischemia and approximately 15% patients have been treated with coronary angioplasty previously. Significant number of study population has LV dysfunction; 29.7% patients has EF between 30% and 50% and 11.8% patients has EF below 30%. Majority of the patients has poor functional class; 66.1% has NYHA class 3–4 and 67.2% has CCS class 3–4. Pre-operative variables of study population are shown in Table 1.
Pre-operative characteristics of study population.

MI: myocardial infarct.
More than two-thirds of CE were performed in the left coronary territory and in 43.2% cases LAD required endarterectomy followed by diagonal artery (26.6%), Obtuse Marginal (OM) (4.9%) and 25.3% in the right coronary territory (Figure 2). Conduit for LAD graft used LIMA in 100% cases in our study. The mean number of grafts was 3.3 and 88.8% patient required CABG for three or more vessels CAD. Only 1.3% patients had undergone CE with CABG surgery as an emergency procedure in this review and there were only 12.8% conversions to on-pump CABG using CPB. The quantities of graft and endarterectomies are shown in Table 2.
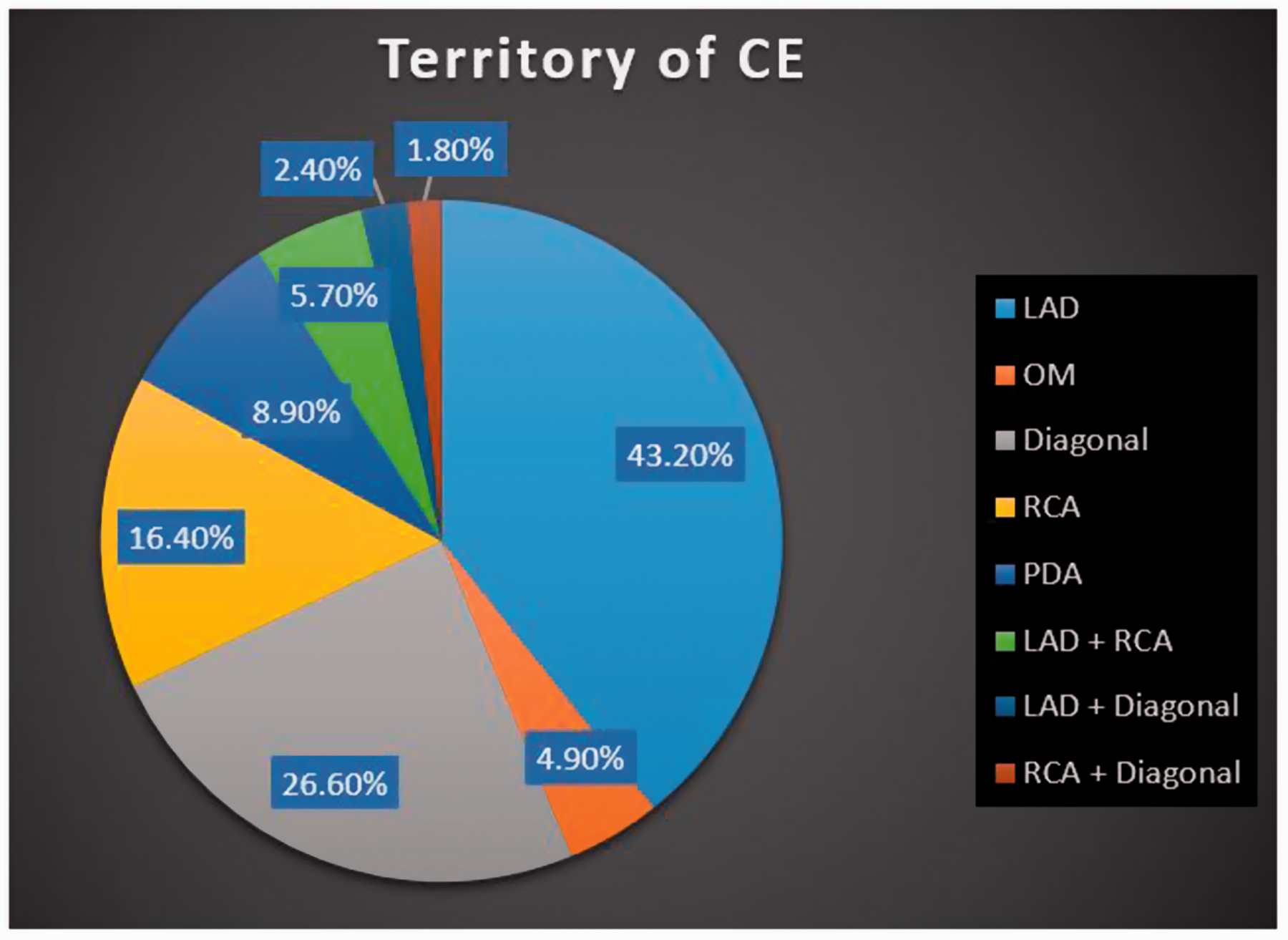
Pie Chart represents the territory of coronary endarterectomy in a patient with diffuse CAD.

Instruments used for the removal of the atheromatous plaque during off pump coronary artery bypass grafting (OPCABG).

Long segment atheroma removed by Professor Asit Baran Adhikary (a and b) and atheromatous plaque with stent in situ (c): 14 cm longest atheromatous plaque extracted from RCA (a); 10-cm long segment atheroma from LAD (b).RCA: right coronary artery; LAD: left anterior descending.
Operative data of study population.

CPB: cardiopulmonary bypass; RCA: right coronary artery; LAD: left anterior descending; PDA: Posterior Descending Artery; OM: Obtuse Marginal.
Post-operative ICU mortality rate was 1.9% and there were no intra-operative mortalities in our study. No patient required ventilation for more than 12 hours. Patients were extubated following a mean of 9.8 ± 1.25 hours and mean ICU stay was 36.6 ± 6.7 hours following surgery. A mean of 1.5 ± 0.5 units of blood was transfused post-operatively. The mean duration of hospital stay was 10 ± 1 days. Only 15.7% patients developed new onset AF following CE with CABG procedure and others post-operative complications was also insignificant (3.1% post-operative MI, 2.3% renal failure, 1.1% respiratory failure and 1.4% neurological complication). Use of intra-aortic balloon pump (IABP) was very minimum in our study (only 0.8%). The mean follow-up period was 10.5 ± 2.5 months. In our review, 92.7% patients were in regular follow-up, and significantly 91.8% of our patients were angina free at median follow-up of 2.5 years. However, 88.7% of study population were free from angina at long-term follow-up over a period of 5 years. Amid this follow-up period, 85.8% of the Endarterectomy of Coronary Artery (ECA) patients were in Canadian Class l and 14.2% in Canadian Class II. The rest of the post-operative characteristics including mortality and morbidity are listed in Table 3.
Post-operative variables of study population.

MI: myocardial infarct
Discussion
Despite the 60-years history of CE as a treatment option for diffuse CAD, till date its application remains controversial as it conveys a higher peri-operative hazard and poor long-term survival.
1
In a review, Djalilian et al.
13
described CE procedure being as yet a matter of controversy, which was also supported by other authors. Usually, we utilize the “traction technique – slow, sustain and continuous traction” to perform CE. This procedure is more straightforward, easy to perform through a little incision and simpler to reconstruct. But the potential dangers incorporate inadequate expulsion of the plaque and the “snowplow effect,” to be specific, shearing-off of the plaque in the side branches. The “open procedure” is better visualized, which may help with the entire expulsion of the atheroma from the coronary vessel and its side branches.
14
In our study, we used the LIMA to anastomose with LAD in 100% of our cases. Previously, the internal mammary artery (IMA) has been utilized cautiously as a conduit to an endarterectomized vessel, but many authors have shown satisfactory early and late clinical results with luminal patency of IMA to an endarterectomized vessel compared to great saphenous vein conduit.
13
In our review of high-risk group patients, the early mortality rate in ICU was of 1.8%, which was largely attributed to LAD endarterectomy and endarterectomy multiple coronary arteries, which is consistent with findings form previous studies.
6
Following CE, routine heparin infusion was prescribed to prevent thrombosis in graft or native tissue in the early post-operative period bridging to oral Warfarin for next 3 to 6 months, which is commonly practiced by other specialists also.
2
Conclusion
CE accomplishes total myocardial revascularization in patients with diffuse CAD and should not be considered a contraindication to OPCABG. However, surgical skill and the patient’s selection criteria are main stream for better outcome in CE with CABG.
Footnotes
Acknowledgements
Dr. TS Han (Deputy Editor of JRSM Cardiovascular Disease) helped with proofreading of the draft. Dr. Han played no other roles in the content of the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
None.
Guarantor
Asit Baran Adhikary.
Contributorship
Ranjan R – Conception, planning, data collection, carrying out, analyzing and writing up of the work.
Adhikary D – Analyzing and writing up of the work.
Mandal S – Expert guidance to analysis and writing up the work.
Seedher A – Analysis and writing up the work.
Adhikary AB – Provide active help, guidance and valuable suggestions regarding analysis and writing up the work.