
Abstract
Introduction and objectives
Atrial fibrillation is a common arrhythmia following coronary artery bypass graft surgery. Its incidence can range from 10 to 60% of patients undergoing coronary artery bypass graft. This rhythm can result in shorter or longer intervals between beats.
Methods
Medical records of 143 patients from the Queen’s Medical Center, Kuakini Medical Center, Saint Francis Medical Center, and Straub Hospital and Clinic, all of which are located in Honolulu, Hawaii were reviewed. An additional 39 records of patients who did not develop these complications were also reviewed as a control group. Patients were selected according to the ICD codes for atrial fibrillation/flutter and coronary artery bypass graft. Both anomalies can lead to increased health care costs, morbidity, and mortality. In this study, possible predisposing factors to these complications were investigated. The time of onset, weight gain, elapsed time, fluid status (in/out), hematocrit, and drug regimens were compared between the two groups.
Results
The differences in weight gain, fluid status, and hematocrit between the groups were not significant. There were a total of 17 different drugs prescribed to the group as a whole but not every patient received the same regimen.
Conclusions
Atrial fibrillation and flutter were found to be more common in males, particularly between the ages of 60 and 69 years. There were no other significant findings.
Keywords
Introduction
Atrial fibrillation (AF) is a relatively common arrhythmia that may be observed in otherwise normal subjects, and also in those with rheumatic and ischemic heart disease, thyrotoxicosis, and hypertension.1–3 A frequent post-operative complication of most types of cardiac surgery, AF occurs in a wide range of incidence between 10 and 60% in those undergoing coronary artery bypass graft surgery (CABG). 4 Development of AF prolongs hospital stays and is associated with poor long-term prognosis. In a 20-year study between 1971 and 1992, a consecutive series of 9600 patients who underwent CABG surgery were followed up with 99.9% success. The 1-, 10-, and 20-year risk-unadjusted survival was 97, 81, and 50%, respectively. 5 Meanwhile, the Cleveland Clinic Foundation has reported the lowest prevalence of pre-operative electrocardiogram documented AF at 0.96% (451 of 46,984 patients). 6 Now, more advanced technology allows surgeons to ablate AF during CABG surgery versus cut-and sew lesions. 7 During AF, multiple foci can serve as pacemakers with rapid, irregular firing, resulting in randomly irregular atrial depolarization at a rate of 350–450 beats per minute. The electrocardiogram is notable for an uneven, irregular baseline without any recognizable P waves due to the chaotic atrial depolarization and normal QRS complexes. 8 Atrial flutter is defined by a rapid, regular atrial rate of 250–350 beats per minute, a narrow QRS complex and a ventricular rate of 125–175 per minute. The pacemaker is atrial and an A-V block is almost always present and only one ventricular depolarization occurs per 2 or 4 atrial depolarizations (2:1, 4:1), because the A-V node is refractory to all other rapid atrial impulses.
The increasing prevalence of AF in patients often leads to increased health care costs from associated conditions and increased morbidity. Typical conditions associated with AF include hypotension caused by rapid ventricular response, myocardial infarction, and death.9–19 Additionally, patients with AF are older adults with co-existing conditions such as compromised ventricular function, hypertension, diabetes mellitus, renal insufficiencies, peripheral vascular disease, a history of congestive heart failure or myocardial infarction, dyspnea, and cerebrovascular problems. 15 During the peri-operative period, management of patients experiencing AF is often times difficult as occurrences vary in degrees of intensity (seriousness) and frequency. 20 As technology advances, new techniques for the ablation of AF have become viable preferred strategies for treating patients experiencing arrhythmias, especially those undergoing CABG. 21 Means of prevention of AF following CABG procedures, however, even in those where preoperative atrial pressures and volumes were normal are still debatable. There has only been scant progress in finding correlations between predisposing factors and precipitating causes leading up to the occurrence of AF and thus, ideal treatments have yet to be determined. 22
This study evaluated perioperative parameters of 143 patients in Honolulu, Hawaii who experienced AF/flutter following a CABG surgery. These parameters included perioperative weight gain, fluid intake and outtake (I/O) values, hematocrit, drug usage, and blood chemistry values. Other factors considered were age and sex of the patients. The results were compared in an attempt to correlate the previously mentioned parameters with the prevalence of AF in these patients. New developments in the management of AF were reviewed.
Patients and methods
The institutional review boards of the participating hospitals approved this retrospective study. Medical records were reviewed from the Queen’s Medical Center, Kuakini Medical Center, Saint Francis Medical Center, and Straub Hospital and Clinic, all of which are located in Honolulu, Hawaii. Patients were selected according to the ICD code for AF/flutter and CABG. Both anomalies can lead to increased costs, morbidity and mortality. In this study, possible predisposing factors to these complications were investigated. The time of onset, weight gain, elapsed time, fluid status (in/out), hematocrit, and drug regimens were compared between the control and the experimental groups. There was not a significant difference in weight gain, fluid status, or hematocrit between the groups. Some patients were administered different drugs than others. There were a total of 17 different drugs prescribed. AF and flutter were found to be more common in males compared with females, particularly in the 60–69 age group.
Results
Parameters measured
Elapsed time
This was defined as the time period between admission of the patient into the intensive care unit (ICU) and the onset of atrial arrhythmia. “Day One” is the day of the surgery. Patients were observed over a 7-day period following the operation.
Weight gain
This was defined as the difference in pounds between the patients’ weight preoperatively and his/her weight at the onset of atrial arrhythmia. Fractional weights were rounded to the next nearest whole number. Each patient was carefully monitored. There was a significant increase in weight in four patients.
Fluids in and out (I/O)
The total fluid status (in/out) for the patients during the time span between the day of surgery and the first day of the atrial arrhythmia was recorded. The total “Fluids Out” during that period was subtracted from the total “Fluids In”. Negative values indicated that the patient lost more fluids than he/she took in.
Hematocrit (% recovered)
Patients’ hematocrit values were measured to determine the extent of recovery of his/her erythrocyte count. The value for the “atrial arrhythmia day” was divided by the “preoperative value” to arrive at a number. The former was defined as the third post-operative day as this was when most patients went into AF and/or flutter.
Drug therapy
Drugs given to the patients were recorded. Any electocardioversions and spontaneous cardioversions performed were noted. Patients were administered drugs as needed. Drug regiments varied from patient to patient based on each situation. Table 1 shows the different medications received by patients as well as the numbers who received, electrocardioversions and thoracocentesis and those who underwent spontaneous cardioversion.
Comparison of the elapsed time and the number of patients experiencing AF during the 7-day period. Display of the exact weight gain (or loss) on the first day of atrial arrhythmia. The amount of fluids administered between the day of coronary artery bypass grafting surgery and the first day of atrial arrhythmia. Hematocrit (erythrocyte levels) values for the 143 patients in the study. Based on the fluid control, 1000+ ml displayed the most significant amount of fluid change. The control group showed a statistically insignificant difference in fluid control. The weight gain in the control group displayed variation compared to the patients who had arrhythmia. Of the 39, no single patient lost any significant weight. Hematocrit percentage recovery rates. Majority of the patients sustained in the 80th–90th percentiles. Drugs and procedures used on patients in the study.



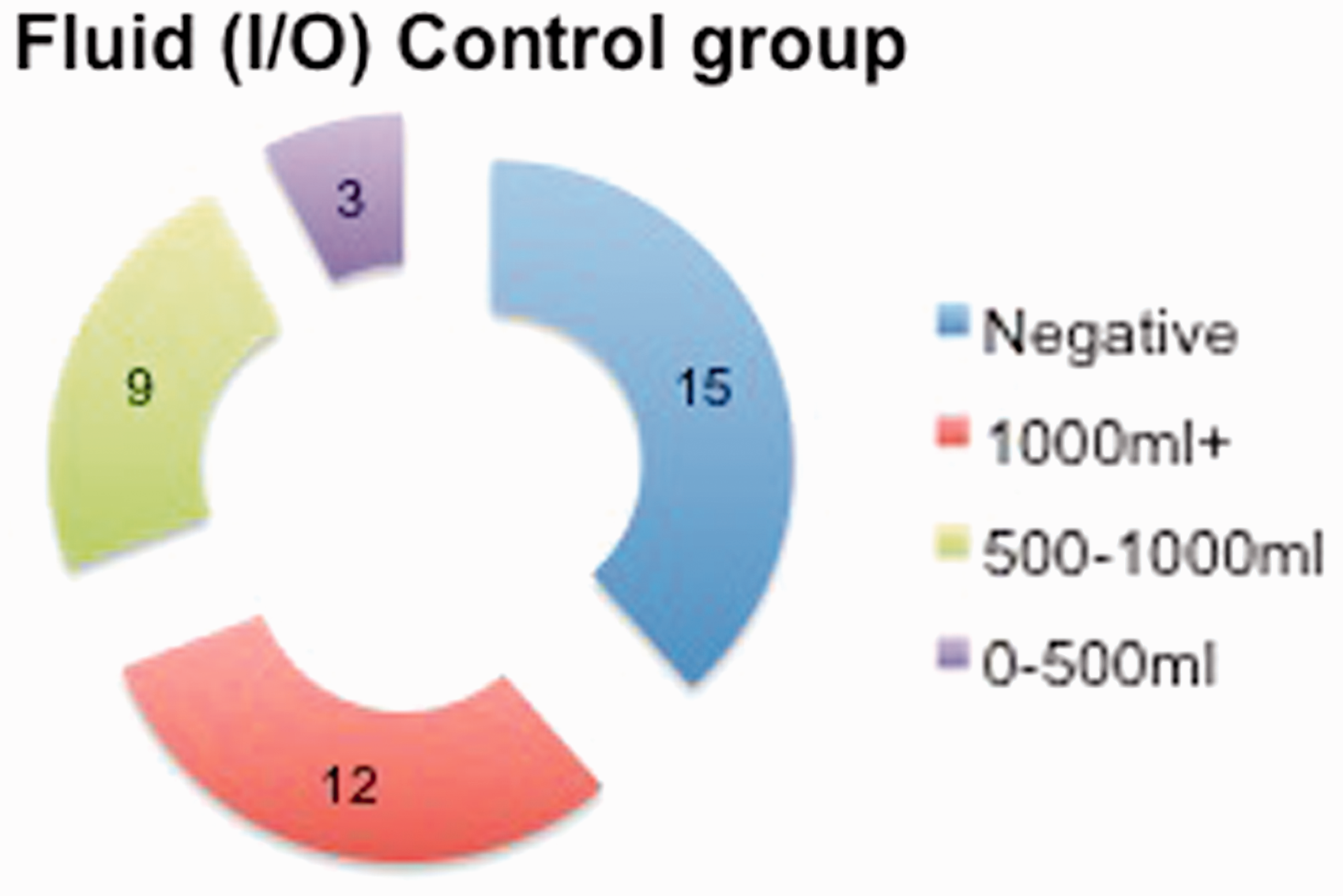



Control group
This group consisted of 39 males between the ages of 60 and 69 years who underwent a CABG surgery without going into AF/flutter post operatively. They were examined at 3 days following surgery, as that was the day that most of the AF patients went into their arrhythmia.
Discussion
AF and flutter can occur early in the postoperative period or as a late complication of cardiac surgery. Postoperative AF is likely related to a combination of factors. These include pre-existing degenerative changes in the atrial myocardium and perioperative conditions that result in abnormalities of several electrophysiologic parameters that promote the development of AF, such as dispersion of atrial refractoriness, increase in phase 3 depolarization, enhanced automaticity, increased interatrial conduction time, and decreased conduction velocity and atrial transmembrane potentials.23–27 Perioperative factors that have been implicated in the creation of atrial susceptibility to AF or atrial flutter include pericarditis, atrial injury from surgical handling, or cannulation, atrial suture lines, acute atrial enlargement from pressure or volume overload, inadequate myocardial protection during cardiopulmonary bypass, atrial ischemia, long bypass and aortic cross-clamp times, hyperadrenergic states (such as the use of postoperative inotropic medications), pulmonary complications, hypoxemia, inflammation,28,29 hypokalemia, and hypomagnesemia.30–33 While mechanisms specific to late AF have not been identified, atrial flutter in these patients is re-entrant and may involve atypical isthmuses between natural barriers, atrial incisions, and scar as well as the cavotricuspid isthmus.34–36
Some patients develop AF after cardiac surgery without any apparent predisposing factors. However, most patients have at least one clinical predictor. Preoperative risk factors include Increasing age,37–43 previous history of AF, mitral valvular disease, particularly mitral stenosis, increased left atrial size or cardiomegaly, previous cardiac surgery, chronic obstructive pulmonary disease (COPD), elevated preoperative hemoglobin A1c, 48 low-intensity physical activity in the year prior to surgery, 49 Caucasian race, 31 obesity,47,50 absence of beta blocker or angiotensin converting enzyme inhibitor (ACE inhibitor) treatment or withdrawal of previous treatment, preoperative digoxin use in some38,44 but not all studies, 45 higher preoperative plasma concentration of brain natriuretic peptide (BNP), 41 low-dose dopamine, 51 severe right coronary artery stenosis, 43 preoperative increase in P wave duration on surface (>116 msec) 46 or on signal averaged (>140 msec) ECG.40,52
Though rarely fatal, 10–60% of patients undergoing CABG surgery may develop AF and flutter. 57 Although several studies have described the occurrence of AF and flutter following CABG, there is no clear agreement of its pathogenesis. 3 Advancing age has been reported as a consistent risk factor, and is in agreement with our findings. An examination of the information from the 143 patients in our study allows several observations. Regarding elapsed times, most patients went into AF/flutter on either the third or fourth postoperative day. Approximately 70% of all those who lapsed into atrial arrhythmias did so during this time. On the subject of weight gain, 64% of patients gained between 2 and 8 pounds. Looking only at those patients who gained weight and ignoring those who remained the same and those who lost weight, the earlier percentage rises to 72%. In terms of fluid distribution, 66% of those studied had a positive fluid balance. It is worth noting that 55% of those with a positive fluid balance at the time of atrial arrhythmia had a 1000+ ml surplus. With regard to the hematocrit, 76% of patients with AF/flutter had recovered between 70 and 100% of their original erythrocyte count.
The prescription of drugs was made noteworthy both by the wide variety of drugs prescribed, and by the preponderance of Digoxin. About 66% of the patients were treated with the latter, either alone or in combination. In all, there were 17 different drugs prescribed. About 19% of the patients who slipped into atrial arrhythmia resumed a sinus rhythm spontaneously and did not require medical intervention. Comparing the controls to the test group failed to yield any differences in value or patterns. The weight gain was well scattered, without any one focal point. The fluid I/O situations were similar in the two groups. This was also the case regarding the hematocrit. Both groups of patients gained weight peri-operatively and followed a similar pattern of gradual weight loss postoperatively. Finally, recent reports have suggested that diseases of the arteries supplying the sino atrial (SA) and the atrio ventricular (AV) nodes may contribute to the incidence of AF following CABG. If this is the case, it may be possible to predict the incidence of AF in patients by studying the anatomical distribution of these arteries. Such studies can pave the way for the prophylactic treatment of AF in these patients prior to CABG surgery.53–55
Conclusions
Patients who experience atrial arrhythmias gained weight peri-operatively and followed a similar pattern of gradual weight loss postoperatively, as well as those who did not experience atrial arrhythmias. The fluid distribution between the two groups was also similar as were the hematocrit values. Despite the fact that the hypothesis was not supported by the results, several interesting pieces of information came to light. It was seen that of those patients who lapsed into atrial arrhythmias, 90% were male. Looking at the overall picture, this transposes into the following figures. Among all coronary artery bypass operations, 27.1% of the males who underwent surgery will go into atrial arrhythmia, while the figure for women is much lower at 9.6%. It was also observed that the predominant sex/age category of those who went into atrial arrhythmia were males in the 60–69 year group. A final interesting point concerns the heavy use of Digoxin for the prophylaxis of arrhythmias. Some researchers have found that several factors associated with open-heart surgery tend to increase the sensitivity to Digoxin and lessen the threshold for toxicity following surgery. These included hypocalcemia, hypomagnesmia, and a reduced creatinine clearance. In addition, Digoxin is not effective against ventricular arrhythmias. Some researchers have proposed beta-blockers such as Propranol as a prophylaxis for arrhythmias.56,57
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
None.
Guarantor
Shyamal Premaratne.
Contributorship
Data collection -- Shyamal Premaratne, Nahidh W. Hasaniya Data Analysis -- Shyamal Premaratne, Ishani D. Premaratne, Naomi D. Fernando, Lashira Williams Figures -- Shyamal Premaratne, Ishani D. Premaratne Draft -- Shyamal Premaratne, Ishani D. Premaratne, NDF FINAL PAPER -- Shyamal Premaratne, Ishani D. Premaratne, Nahidh W. Hasaniya