
Abstract
Objectives
In Denmark, the local and regional health authorities share responsibility for cardiac rehabilitation (CR). The objective was to assess effectiveness of CR across sectors coordinated by a nurse case manager (NCM).
Design
A one-year follow-up study.
Setting
A CR programme (GoHeart) was evaluated in a cohort at Lillebaelt Hospital Vejle, DK from 2010 to 2011.
Participants
Consecutive patients admitted to CR were included. The inclusion criteria were the event of acute myocardial infarction or stable angina and invasive revascularization (left ventricular ejection fraction (LVEF) ≥45%).
Main outcome measures
Cardiac risk factors, stratified self-care and self-reported psychosocial factors (SF12 and Hospital Anxiety and Depression Scale (HADS)) were assessed at admission (phase IIa), at three months at discharge (phase IIb) and at one-year follow-up (phase III). Intention-to-treat and predefined subgroup analysis on sex was performed.
Results
Of 241 patients, 183 (75.9%) were included (mean age 63.8 years). At discharge improvements were found in total-cholesterol (p < 0.001), low density lipoprotein (LDL; p < 0.001), functional capacities (metabolic equivalent of tasks (METS), p < 0.01), self-care management (p < 0.001), Health status Short Form 12 version (SF12; physical; p < 0.001 and mental; p < 0.01) and in depression symptoms (p < 0.01). At one-year follow-up these outcomes were maintained; additionally there was improvement in body mass index (BMI; p < 0.05), and high density lipoprotein (HDL; p < 0.05). There were no sex differences.
Conclusion
CR shared between local and regional health authorities led by a NCM (GoHeart) improves risk factors, self-care and psychosocial factors. Further improvements in most variables were at one-year follow-up.
Keywords
Introduction
Since 2007, the local and regional health authorities in Denmark have shared responsibility for prevention, health promotion and physical rehabilitation for patients with chronic cardiovascular disease after hospitalisation. The outcome of cardiac rehabilitation (CR) in the transition between hospital and municipal is not well-documented. Studies suggest that several patients opt out from the recommended sequence due to lack of information and interruptions, when the health care delivery task is cooperated across sectors. This encourages the need for Shared Care between sectors.1,2 The use of proactive support across sectors, e.g. through a nurse case manager (NCM), has proved effective in chronic disease management.3,4
Another challenge for CR is sex differences in health outcomes. It is well-known from primary prevention that women do not perceive heart disease as a priority health concern, or they have less obvious symptoms. 5 Further, women have lower compliance rates and completeness of programme. 6 Therefore, the development of methods to enhance women’s compliance in healthcare settings should be included when developing programme.
We have previously shown that the implementation of a NCM compared to usual care reduces the number of patients who refuse to participate in CR from 25% to 5% and increase the number of patients who participate in the CR at the municipality from 46% to 58% with no sex differences. 7
The aim of this study was to assess effectiveness of CR across local and regional health authorities coordinated by a NCM at clinical, self-care and psychosocial outcomes at discharge from hospital after three months (phase IIb) and one-year follow-up (phase III).
Methods
Design, setting and study population
Figure 1 shows the Danish single-centre CR programme GoHeart. The programme was conducted between the Department of Cardiology, Lillebaelt Hospital Vejle and the Municipal Health Centre Vejle. The programme was in accordance with the European Society of Cardiology (ESC) guidelines.
8
The Shared Care between hospital and the municipality was standardised as were the components of the hospital-based NCM responsibility across the hospital and municipality sectors.
9
Key components of the NCM were administration, direct patient support and enhanced support for vulnerable patients with low self-management (Table 1). In agreement with the local general practitioners (GPs) and approval from the patient the NCM made telephone contact to the GP at discharge if the patient was stratified with high risk including low self-care management to ensure a follow-up in phase III (Figure 1). The NCM provided risk stratified care management using the Chronic Care Model risk stratification tool10,11 based on psychosocial risk factors, disease complexity and self-care management. As all patients included had chronic ischaemic heart disease (IHD) they were stratified to differentiated CR programme according to their self-care level (low or high).
Flow chart of the cardiac multidisciplinary rehabilitation programme for cohort (GoHeart). Key components of the nurse case management at the Department of Cardiology, Lillebaelt Hospital, Vejle, Denmark. aUsual cardiac rehabilitation.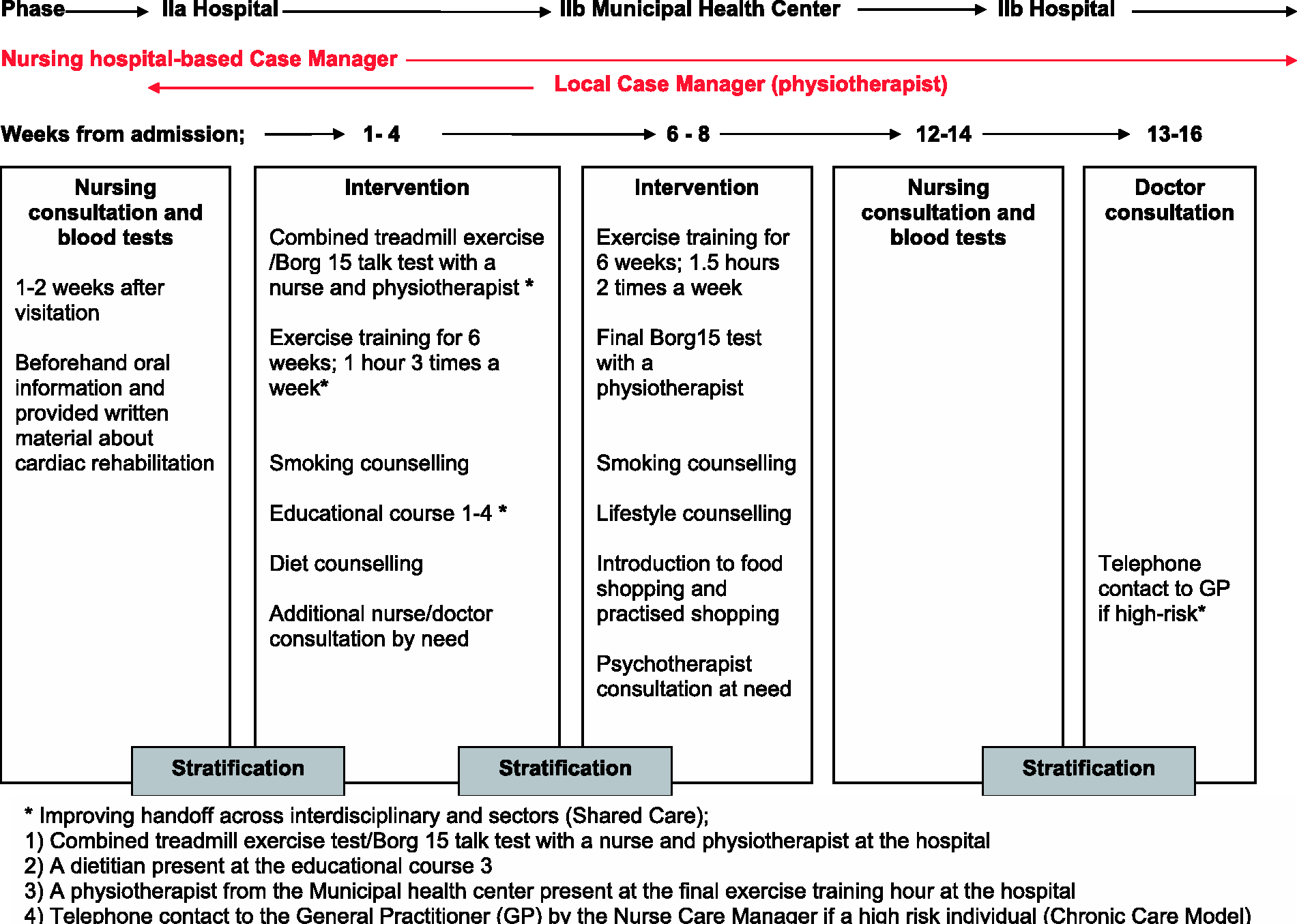

Patient enrolment and inclusion criteria
Consecutive patients admitted to CR in the period from September 2010 to November 2011 at the Department of Cardiology, Lillebaelt Hospital Vejle were asked to participate in the study at the nurse CR admission consultation (Figure 1 and Figure 2). The criteria for CR were the event of acute myocardial infarction (MI) or stabile angina and coronary angiography at the Department leading to assessment of revascularisation at the associated centres (percutaneous transluminal coronary intervention (PCI), coronary artery bypass grafting (CABG) with or without combination of valve replacement or recommendation of a conservative strategy). Exclusion criteria were heart failure (left ventricular ejection fraction (LVEF) <45%). These patients received CR through the heart failure clinic.
Flow chart for the GoHeart-study.
In total 315 patients fulfilled the criteria for CR in the period (Figure 2). Twenty-three (7.3%) patients refused participation mainly due to previous CR. Further reasons were alcohol abuse and severe psychiatric disease, found it unnecessary or because of workload. Overall 292 patients accepted admission to CR and were invited to participate in the study. The NCM contacted non-responders (to the questionnaires) or drop-outs (absent at the clinical follow-up measurements) by telephone after two weeks. If there was no response to this telephone call a postal reminder was sent. Participants were excluded from the analysis upon failure to respond to the follow-up (Figure 2).
Data collection and measurements
Clinical characteristics at baseline of the participants in the study cohort (GoHeart) compared to non-responders and non-participants.

NSTEMI: non-ST segment myocardial infarction; STEMI: ST segment myocardial infarction; PCI: percutaneous transluminal coronary intervention; CABG: coronary artery bypass graft; IHD: ischaemic heart disease; stratification; according to the Chronic Care Model; BMI: body mass index.
Values are numbers (%) unless stated mean (SD).
Outcome after cardiac rehabilitation for cohort at admission compared to three months at discharge and at one-year follow-up.a

mo: months; NS: non significant; BMI: body mass index; METS: 3,5 ml O2/kg/min; 6MWT: 6-min walk test; *HbA1c: only measured for diabetic.
aSelf-care management was determined after stratification according to the Chronic Care Model. Health status (SF-12v2) and Hospital Anxiety and Depression Scale (HADS); estimated data were calculated for participants who responded at both control times. Physical component score (pcs) and mental component score (mcs). Continuous clinical variable, self-care management, Short-Form 12 version 2 (SF-12v2) and Hospital Anxiety and Depression score (HADS). Values are numbers (%) unless stated.
Clinical measures and risk behaviour
Height and weight were measured, and body mass index (BMI) was calculated. Blood pressure was monitored in the supine position. A blood sample was drawn non-fasting to measure lipids (total-cholesterol, high density lipoprotein (HDL), low density lipoprotein (LDL) and triglycerides) and HbA1c in people with diabetes (n = 32). Alcohol consumption was measured in unit per week. Smoking was divided into current, previous and never smoking (Tables 2 and 3).
Exercise capacity was measured by a treadmill exercise test 12 combined with the Borg15 talk test 13 at the Hospital (Figure 1). At follow-up at the Municipal Health Centre, the patients were tested by the Borg15 talk test only, since the treadmill exercise test was not an option. Patients, who were unable to perform the initial test, had a 6-min walk test initial. This was only an option at the hospital (n = 7) (Table 2).
Psychosocial measures
Participants’ self-care management was determined by the NCM using the criteria from Chronic Care Model.10,11 This was determined according to how the patient engaged to promote health, to augment physical, social or emotional resources and to prevent sequela.
The self-reported health status was measured using the Short-Form 12 version 2 (SF-12v2) with psychical (pcs) and mental (mcs) component summery scores. 14 Anxiety and depression were measured by the Hospital Anxiety and Depression Scale (HADS).15,16 Participants scoring HADS anxiety ≥8 or depression ≥8 were encouraged to contact their GP.
Psychosocial measures were not taken at baseline due to the acute condition the patients were in.
Data at each of the follow-up times were transferred to the research database and checked for errors. If errors were encountered, the original questionnaire was investigated and the database entry corrected.
Ethics
According to Danish law, this study did not need approval by the Regional Ethics Committee. This was confirmed by the Chair of the South Danish Regional Ethics Committee. The Danish Data Protection Agency approved the research database (J no. 2008-58-0034). Signed informed consent was obtained from all participants.
Statistical analysis
Characteristics and outcomes were reported as means (SD) for normally distributed continuous variables, median (interquartile range (IQR)) for skewed continuous variables and number (%) for categorical variables. The effectiveness of the programme was estimated in terms of the differences between admission (phase IIa) and three months at discharge from hospital (phase IIb), and between discharge and 12 months follow-up from admission (phase III). We reported 95% confidence intervals to indicate the precision of the estimates. Wilcoxon signed-rank test was used to compare differences. A p value of 0.05 or less was used to signify statistical significance. The estimated data were calculated for the participants who responded at the comparative follow-up times (Table 3). Predefined subgroup analysis on sex was performed. Data were analysed using Stata software, version 12 (StataCorp, College Station, TX).
Results
Participant flow
Of the 292 patients invited to the study, 51 (17.5%) refused to participate (Figure 2). The non-participants were older, had known IHD and other chronic diseases, see Table 2. Fifty-eight of the included patients did not contribute to the analyses because of drop out or non-response to the questionnaires.
Six men died. Three of the non-participants (2 of myocardial re-infarction, 1 of cancer disease) and three of the non-responders in the cohort died (1 of myocardial re-infarction, 2 died suddenly without clarifying autopsy out of hospital). Of 241 patients, 183 (75.9%) provided data for analysis (Figure 2).
Participant baseline characteristics
Characteristics are shown in Table 2. The mean age was 63.8 (SD 9.0). The majority were men (76%) significantly younger than the women (mean age 62.9 ± SD 8.6 compared to 66.9 ± 9.7; p = 0.020). The majority of the participants were Danish (97.8%), were married/cohabiting (83.2%), retired 57.8%) and lived in immovable properties (77%). Statistical significant differences were found between female and male. More females lived alone (n = 30, female 32.6% versus male 11.9%, p = 0.004), were retired (n = 104, female 72.2% versus male 52.9%, p = 0.040) and had a shorter education, <3 years after primary school (n = 116, female 86.4% versus male 56.1%, p < 0.0001), respectively.
Most of the participants (66.1%) attended the CR after PCI without acute MI (Table 2). Of all, 17.5% had CABG (21.6% men compared to women 4.6%; p = 0.011). Of all, 20.8% had known IHD. Concerning risk factors, 50.3% had known family history of IHD, 70.5% had a smoking history. Few had diabetes (17.5%). Of all, 70.5% had medically treated hypertension and 91.3% had medically treated hyperlipidaemia at admission. Of all, 50.4% of the participants had low physical activity level (0 days/week with ≥30 min/day).
Of all, 16.6% of men had alcohol consumption above the limits recommended by the Danish Health and Medicines Authority (men <14 and women <7 units/week) compared to 2.3% of females (p = 0.011). Men were more obese (p < 0.0001). Of all, 26% of the participants had low self-care management at admission with no sex difference.
Non-participants and non-responders characteristics
Overall the CR non-participants and the non-responders in the study had more disease complexity and lower level of self-care management compared to the participants (Table 2). The non-participants differed significantly on baseline characteristics in age, type of MI and previous known IHD compared to the participants. They were older (mean age 68 (SD 11.6) compared to 63.8 (9.0); p = 0.006), fewer have had ST segment myocardial infarction (STEMI) at present (p = 0.003) and more had known IHD (p = 0.026). Furthermore, they had significantly more risk factors to CVD, e.g. more with a smoking history (p = 0.001), statin treated (p = 0.03), lower physical activity (p = 0.001) and comorbidity with lung disease (p = 0.042) and renal failure (p = 0.009). Moreover, they were stratified with lower level of self-care management (p < 0.0001).
The non-responders were compared to the participants followed significantly in risk factors for CVD, e.g. more with a smoking history (p < 0.0001), insulin treated diabetic (p = 0.022), statin treated (p < 0.0001), lower physical activity (p < 0.0001), lesser obesity (p = 0.004), comorbidity with lung disease (p = 0.019) and musculoskeletal disease (p = 0.012). Moreover, they had lower levels of self-care management (p < 0.0001). The same pattern was seen comparing the non-participants to the participants (Table 2). No difference in comorbidity was found between groups concerning previously ischaemic stroke, medically treated mental depression or peripheral vascular disease. The groups were comparable on other clinical variables. No sex differences were found.
The clinical and risk behavioural outcomes after three months and one year
Table 3 shows the difference in outcomes. No difference at discharge (3 months) was found in BMI, whereas significant improvement in BMI was found at one-year follow-up (mean −0.26, 95% CI: −0.50 to 0.03, p = 0.026).
No differences were found in systolic blood pressure (SBP). The level of diastolic blood pressure (DBP) was higher at one-year follow-up compared to three months at discharge (mean 2.69, 95% CI: 1.20–4.17, p = 0.0005). Total-cholesterol (difference mean −0.37, 95% CI: −0.51 to 0.22, p < 0.0001) and LDL (difference mean −0.31, 95% CI: −0.19 to 0.42, p < 0.0001) were significantly decreased due to treatment (for statins and aspirin, respectively, 94.5% and 96.7% at the one-year follow-up with no significant difference between the follow-up times). Total-cholesterol and LDL levels were maintained at one-year follow-up, whereas HDL increased (mean 0.05, 95% CI: 0.01–0.10, p = 0.027).
At admission 12.1% were smokers. Of all, 10.5% were still smokers at discharge and 9.9% at one-year follow-up. The differences were not significant. No differences on alcohol consumption were found.
At discharge from CR (3 months) significant improvement was found in metabolic equivalent of tasks (METS) compared to admission at the combined treadmill exercise/Borg15 talk test (mean 0.68, 95% CI: 0.19–1.17, p = 0.007). After one-year the effect was maintained, but not further improved.
The psychosocial outcomes after three month and one-year follow-up
Self-care management improved significantly at three months, as 12.0% had low level compared to 24% initial. A further decrease was seen at one-year follow-up (8.2%).
Health Status (SF12) improved significantly at three months compared to admission (pcs mean 4.63, 95% CI: 3.02–6.24, p = 0.000 and mcs mean 2.41, 95% CI: 0.75–4.08, p = 0.005). At the one-year follow-up further improvement in the pcs was found (mean 2.2, 95% CI: 0.80–3.60, p = 0.002) whereas the effect on mcs was maintained.
Of all, 14.3% had depression symptoms at admission to CR (HADS depression (HADS-D) ≥8). At three months 8.1% had depression symptoms significantly reduced (p = 0.008). At the one-year follow-up the reduction was maintained (7.4%). No significant difference was found in HADS anxiety (≥8) (Table 3).
No differences were found in sex at any of follow-up times.
Discussion
This one-year follow-up study supports the evidence of the principles of the Chronic Care Model and documents the effectiveness of CR across local and regional health authorities led by a NCM providing risk stratified care management.9,10 Thus, the study showed improvement in most clinical and risk behavioural factors, self-care management and self-reported psychosocial factors (SF12 and HADS). Effects at discharge were on total-cholesterol, LDL, functional capacities, self-care management, self-reported health Health status Short Form 12 version (SF12) and depression symptoms. At one-year follow-up the achieved benefits were maintained apart from a decrease in SF12 physical component and an increase in DBP. Improvements were moreover evident for BMI and HDL, consistent with the emphasis on behavioural lifestyle improvement. Optimal medical treatment was ascertained at discharge and at the one-year follow-up.
The results suggest that adherence to a specialised CR centre with dedicated long-term efforts beyond the early phase is not necessarily needed to maintain improvements in health outcomes. A locally anchored CR, where the NCM provides continuity, may be as effective as a pure hospital-based programme. 8 Furthermore, the programme may enhance women’s compliance which is a challenge in CR.5,6
The outcomes at the one-year follow-up support the strengths of the GoHeart compared to other studies where compliance to lifestyle and treatment regimens have declined after six 6 months. 17 In contrast, the large multi-centre randomised controlled RAMIT-trial 18 investigating CR in England and Wales after two years, compared to usual care, showed no effect on mortality, cardiac or psychological morbidity, risk factors, health-related quality of life or activity. However, the RAMIT study was criticised for methodological weaknesses and a lack of components from modern CR programme. 19 The increase in DBP at the one-year follow-up was unexpected, but in accordance to guidelines of ESC. 20 The achieved health behaviour at one-year -follow-up is not in accordance with general Danish guidelines, but not alarming. For example, 9.9% patients smoked compared to 19.0% in the study by Larsen et al., 21 and 17% in the general Danish population.
In our study, 14.3% of the participants had depression symptoms at admission to CR (HADS-D ≥8), which was reduced to 8.1% at three months (Table 2) and maintained at the one-year follow-up (7.4%). The prevalence of depression in the Danish population is 3–4%. However, that may be underestimated, as it is based on patient registers and does not include depression diagnosed outside the hospital. 22 In a recent Danish study of 897 patients discharged with first-time MI, depressive symptoms were found in 18.6% using the HADS-D Scale. Depressive symptoms following first-time MI were shown to be an independent prognostic risk factor for death, but not for new cardiovascular events. 23 The risk of depression after MI is well-documented and associated with increased mortality.24–27 In GoHeart, the majority had PCI without acute MI (66.1%). The findings support that the diagnosis of CVD is associated with depression and indicates the need for routine screening and for addressing depression in modern CR.8,25,28 Depression symptoms in the EUROSPIRE III survey were more prevalent in women than in men, 29 whereas no sex differences were found in our study.
We found no differences in HADS anxiety (≥8) (Table 2). However, the tendency was in the right direction. The prevalence of people with anxiety symptoms decreased from 22.4% at admission to 16.8% at three months and to 14.9% at the one-year follow-up. The level of anxiety at the three-month follow-up was lower than in a Danish study in people with AMI, where 23.6% reported anxiety (HADS-A) three month after the event. The one-year follow-up results corresponded to the Danish population, and to a Norwegian population in the study by Hanssen et al. 26
Health Status (SF12) in both physical and mental components was improved significantly at three months. At the one-year follow-up further improvement in the physical component was found.
Strengths and limitations
GoHeart is a follow-up study with participants undergoing a standardised CR programme according to offered session length, exercise training, time and duration at hospital and at the health centre. The different components are well described, which a strength for future implementation. The fact that health professionals (NCM, physicians, physiotherapist, etc.) participated in the planning phase, and actively contributed to ensure continuity and to help patients to navigate in the health system, may be a reason for the outcome.
All measurements were undertaken by trained staff following procedures, and information bias is likely to be low. Self-reported data from questionnaires may have potential limitations due to recall bias and social-desirable responses, but the impact may be diminished due to analysing differences.
The main limitation is the lack of a control group, e.g. a group given the previously hospital-based CR intervention before the transition to the municipal responsibility, or a group without a NCM. The characteristics of the non-participants and non-responders having more disease complexity and a lower level of self-care management compared to the participants (Table 2) reveals unresolved critical items in CR. The results are consistent with other studies showing that prevention needs to be individualised. 30
Future CR studies should be evaluated in randomised controlled trials. Further, new studies should be designed to understand organisation barriers for Shared Care and health economic issues of CR across sectors.
The GoHeart programme calls for further health services research including the patient’s perspectives on achieving rehabilitation in local settings, and how these interventions could be differentiated according to risk stratification, including self-care.
Footnotes
Acknowledgements
The authors acknowledge the assistance of nurse case manager Vibeke Pind Haslev, Department of Cardiology, Lillebaelt Hospital Vejle. The authors also wish to thank all patients who agreed to participate and the staff at the Municipal Health Centre Vejle for their valuable help.
Declaration of Conflicting Interests
None declared.
Funding
The work was supported by the Region of South Denmark through the Danish Health and Medicines Authority.
Ethical approval
None.
Guarantor
VBH is the guarantor for all the content presented in this paper.
Contributorship
VBH conceived the study question, and was responsible for the data collection. VBH and HTM were involved in the design phase, the analysis and the interpretation of the results. VBH and HTM drafted the manuscript together, and approved the final version.