
Abstract
Background
Fibroadenomas (FAs) are the most common tumors of the breast clinically and pathologically in adolescent and young women but may be discovered at any age. With increasing use of core biopsy rather than excision for diagnosis, it is now commonplace to follow these lesions with imaging.
Purpose
To assess the incidence of epithelial abnormalities (atypia, in situ or invasive, ductal or lobular malignancies) in FAs diagnosed by core biopsy and to re-evaluate the management paradigm for any growing FA.
Material and Methods
A retrospective review of the senior author’s pathology results over 19 years identified 2062 nodular FAs (biopsied by ultrasound or stereotactic guidance). Eighty-three core biopsied FAs were identified which subsequently enlarged.
Results
Twelve of 2062 of core biopsied nodules demonstrated atypia, in situ, or invasive malignancy (ductal or lobular) within or adjacent to the FA (0.58%). Eighty-three FAs enlarged and underwent either surgical excision (n = 65), repeat core biopsy (n = 9), or imaging follow-up (n = 9). The incidence of atypia, in situ or invasive malignancy was 0/83 (0%). Two enlarging FAs were subsequently surgically diagnosed as benign phyllodes tumors (PT).
Conclusion
Malignancy in or adjacent to a core biopsied FA is rare. The risk of cancer in a growing FA is even rarer; none were present in our series. FAs with abnormal epithelial abnormalities require excision. Otherwise, FAs without epithelial abnormality diagnosed by core biopsy need no specific follow-up considering the negligible incidence of conversion to malignancy. The breast interventionalist must know how to manage discordant pathology results.
Keywords
Introduction
Fibroadenomas (FAs) are common tumors of the breast. Since the 1990s, with the increasing use of core biopsy rather than excision to diagnose these lesions, it has become commonplace to follow these lesions with imaging. This paper is a retrospective review of a subset of patients with core biopsied FAs that have subsequently enlarged, and reports on their clinical management and outcome. There are two issues to consider when FAs enlarge: first, the possible development of malignancy in the epithelial component; and second, the possibility of having misdiagnosed a phyllodes tumor (PT) (or more rarely, the progression of an FA into a PT).
In order to determine the overall incidence of atypia, in situ, or invasive carcinoma within or adjacent to FAs core biopsied in our population, a retrospective review of the pathology from imaging guided, core biopsy-proven FAs was undertaken. These data are compared with the pathologies from enlarging FAs. All PTs diagnosed at our institution by core biopsy over the past 10 years were analyzed as to accuracy of biopsy.
Material and Methods
Incidence of epithelial abnormalities within FAs
The sequential, uninterrupted core biopsy pathology files (1995–2014) of the senior author (LS) were reviewed. All cores were performed at the Barnabas Health Breast Center and interpreted by the Barnabas Pathology Department. Atypia, in situ, or invasive malignancy (ductal or lobular) in or adjacent to an FA were recorded. There were two subgroups: those with nodules biopsied (2062 patients, either under ultrasound [US] or stereotactic biopsy) and those with calcifications biopsied (491 patients, under stereotactic guidance). US-guided core biopsies were performed with a Bard (non-vacuum) device. Sampling protocol dictates obtaining at least two cores on lesions <1 cm, at least three cores on nodules 1–2 cm, and four or more cores on nodules over 2 cm.
Identification of growing FAs
Three available databases were accessed to identify any growing FA since 2004: (i) the radiology reporting information system (RIS); (ii) PACS; and (iii) the Pathology database (US images first became available on PACS in 2004 and the Pathology database has been computer-accessible only since 2004). In total, 1430 patients were identified whose nodules had been biopsied since 2004 (by US or stereotactic guidance).
Inclusion as a growing FA was predicated upon the following criteria: (i) Core biopsy of a nodule either under US or stereotactic guidance with pathology demonstrating FA. We excluded patients with pathology reports indicating “fibroadenomatoid change or mastopathy” or “possible phyllodes tumor” (FAs diagnosed by stereotactic biopsy of microcalcifications were not included). (ii) Pathology was deemed concordant with imaging by the breast interventionalist. (iii) The FA enlarged over any time period following the biopsy, documented by any imaging modality, or a surgical pathology report indicating a larger size of the lesion compared to its size (by imaging) at the time of core biopsy.
The patient’s age at core biopsy was documented, and its maximum single dimension at T0 (time of core biopsy) based on imaging and the maximum single dimension of the growing FA at T1 (time of largest measurement). Percent growth was calculated.
Management of growing FAs occurred in three ways: excision, repeat core, or imaging only. If only imaging follow-up occurred, that length of time was recorded.
Identification of PTs
Using the Pathology database, all lesions diagnosed as PTs by core biopsy since 2004 were identified. All lesions diagnosed as FA by core which were subsequently surgically proven to be PTs were identified. The size of lesion and age of patient were recorded.
Results
Epithelial abnormalities in FAs
Enlarging fibroadenomas (FAs) in 2004–2014.

T0, time at initial core biopsy; T1, time at largest measurement.
In the nodule subset, 2062 patients were identified. In this group, 12 patients had abnormal pathology. Pathology within: three patients had atypia within their FA. Pathology contiguous: six had atypia and one patient had in situ immediately adjacent to the FA. Two had invasive malignancy adjacent to their FA.
There was no occurrence of invasive malignancy within an FA in either subgroup.
Thus, the incidence of atypia, in situ, or invasive malignancy within or contiguous to a nodular FA was 12/2062 = 0.58%.
All of the FAs with abnormal pathology at core biopsy were excised. Their surgical pathology was not tracked, since management of these lesions poses no dilemma. In daily practice, we frequently receive surgical pathology reports which show no residual atypia or malignancy, attributable to complete removal by core biopsy.
Identification of growing FAs
Since 2004, 1430 patients were identified with FAs following core biopsies of nodules. Of these patients, 83 patients were identified who had enlarging lesions, an incidence of 5.8% (Table 1). Many of the 1430 patients did not return for imaging follow-up, so a true incidence of growth cannot be calculated.
Of these 83 patients, the average age was 36.7 years (range, 15–75 years). The average size of original lesion (at T0) was 15.6 mm. (range, 6–60 mm). Average percentage growth was 60%.
Sixty-five of 83 patients underwent surgical excision (average age, 35 years; average size, 16.6 mm [range, 8.8–60 mm]). Nine of 83 patients underwent repeat core only (average age, 38.5 years; average size, 14 mm). Nine of 83 patients underwent imaging follow-up only (average age, 43 years; average size, 11.6 mm).
Of the 74 patients who underwent surgical excision or repeat core biopsy, second pathology revealed FA in 72 and a benign PT in two patients. Of the nine patients who underwent imaging follow-up only (average, 34.7 months; range, 7–82 months), none have been diagnosed with malignancy related to their FA. Total incidence of epithelial malignancy in growing FAs was 0% (0/83). Total incidence of PT in growing FAs was 2.4% (2/83). These two patients are included below in the identified PTs in the category of false negative core biopsies.
Identification of PTs
Of 23 surgically confirmed PTs, 18 core biopsies were true positive (3 malignant PTs correctly diagnosed, 15 benign or borderline PTs correctly diagnosed). Five cores were false negatives with biopsies showing FA: three had discordant imaging and underwent surgery, demonstrating PT; two demonstrated lesion growth (included in the data of growing FA) and were excised, demonstrating benign PTs. In one of these patients, the lesion doubled in 6 months and excision was recommended (Fig. 1). In the other, subsequent magnetic resonance imaging (MRI) showed doubling in size and intense enhancement with cystic areas, felt to be discordant with a diagnosis of previous diagnosis of FA, and excision was recommended (Fig. 2). (Eight patients had false positive fine needle aspirations (FNA) or core biopsies suggesting PT with subsequent surgery proving FA.) The average size of the surgically proven PTs was 37 mm at T0.
A 37-year-old woman with growing FA after core biopsy: doubled in size. Results after excision showed benign PT. A 52-year-old woman. Previous core biopsy showed FA but imaging was discordant on subsequent MRI after growth (intense enhancement with cystic areas). Results after excised showed benign PT.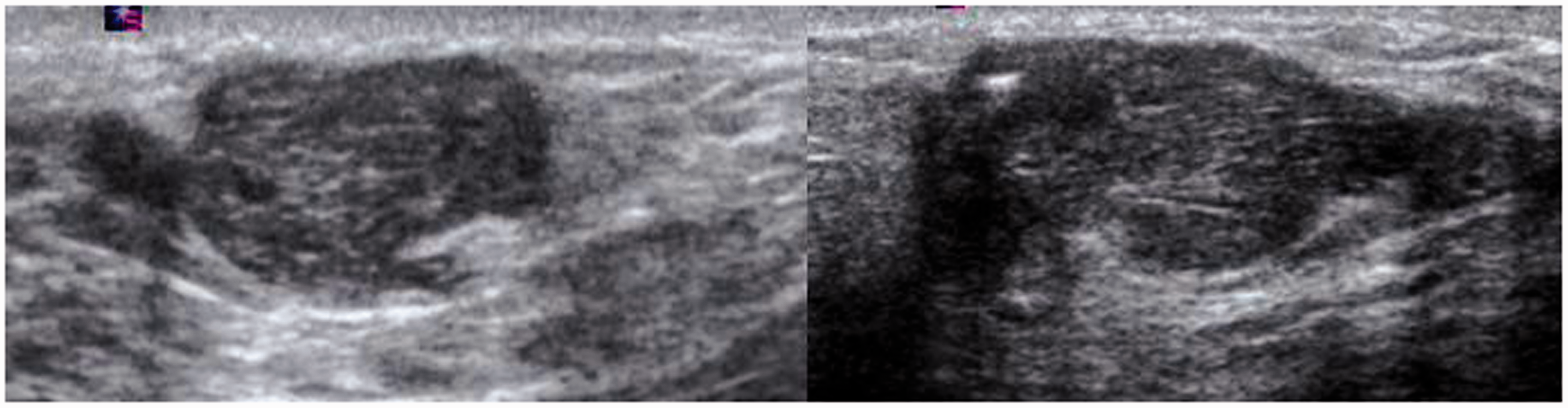

Discussion
FAs are extremely common breast tumors. They are the most common tumors clinically and pathologically in adolescent and young women (1), however, they may be found at any age. They may be single or multiple. FAs are biphasic, composed of epithelial and stromal components. The epithelial component of a FA can display the same pathologic aberrations as the epithelial component of the breast.
The purpose of this study was two-fold: to determine the incidence in our patient population of atypia, in situ, or invasive malignancy at core biopsy of FAs, and to determine the incidence of epithelial pathology in a subpopulation of growing FAs, including the potential re-classification of a growing FA as a PT (false negative core biopsy). We hypothesized that, once core biopsied, a lesion which continued growing might have a higher relative risk of pathology, which could justify its surgical removal or repeat core biopsy. Clearly, all FAs grow, to reach macroscopic size at the time of diagnosis. However, growth after core biopsy poses a management dilemma. Also, it is known that a PT may be misdiagnosed by core biopsy as a FA or rarely a FA may evolve into a PT (1). PTs are usually histologically distinguished from FAs based on the expansion and hypercellularity of the stromal component with a leaf-life stromal growth pattern (1). Jacklin et al. (2) emphasized that the distinction can be very difficult on core biopsy due to small samples and the fact that hypercellularity may also be present in juvenile FAs and the breast tissue of women on hormone replacement therapy. Malignant PTs are usually easier to identify due to their marked atypia and increased mitotic activity. Core biopsy correctly diagnosed three malignant PTs in our review. Our data showed atypia, in situ, and invasive malignancy in 0.58% of core biopsies of nodular FAs, consistent with previous literature (3–6). In the growing FA subset, we found a 0% incidence for epithelial pathology and 2.4% incidence for benign PT. How, then, to manage the core biopsy-proven enlarging FA? Over the past two decades, the management paradigm has evolved. Recommendations based solely on either clinical exam, mammography, or FNA are no longer standard of care.
Dupont et al. (7) in 1994 addressed the long-term risk of breast cancer in women with FAs, and found that “complex” FAs conferred elevated risk. A later study by Carter and Dupont (8) found that atypia within an FA did not confer a higher risk on the subsequent development of carcinoma. Another large study by Ashbeck et al. (9) found that FAs did not exhibit an association with breast cancer development. We did not address the complexity of the FAs in our study or the long-term risk of breast cancer, but rather the actual incidence of a high-risk lesion (atypia, in situ, or invasive malignancy) at first core biopsy and the risk of missing malignancy in growing FAs.
In 2008, Sklair-Levy et al. (10) reported a similar incidence of malignancy in their series of 401 patients (0.25%). They advised excision of any complex FA with a high-risk lesion on core biopsy, a recommendation with which we concur. They also recommended imaging follow-up of all simple FAs and excision if growth exceeded parameters proposed by Gordon et al. in 2003 (11). Gordon’s study, however, was limited by its use of FNA for diagnosis rather than core biopsy.
Foxcroft et al. (12) reported in 2007 on 84 surgically excised phyllodes tumors: only 65% were diagnosed accurately by core biopsy. The larger the lesion, the less accurate was the pre-surgical core biopsy. Six percent of their PTs were malignant (5/84). None of these five tumors underwent prior core biopsy. Of the PTs in their series where serial measurements were possible, nearly all grew more rapidly than the average growth rate for growing FAs in Gordon’s study. The authors concluded that even where there are no clues on imaging, cytology, or core biopsy to suggest PT, surgical removal should be considered for large (>3 cm) or rapidly growing lesions to exclude PT. The average percent growth of our growing FAs was 60.4%. If 50% were used as the percent growth threshold above which surgery would be recommended, excision would have been avoided in 27 of the 65 surgically excised growing lesions. A 2007 imaging article by Bode (13) analyzed 12 excised PTs, which had undergone previous core biopsy: two of the 12 were falsely diagnosed by core as FAs, yielding a false negative rate of 17%. However, in both of those cases, the imaging findings were discrepant: the lesions were large and heterogeneous on US imaging.
Our data differ slightly. Of the 23 surgically proven PTs which underwent prior core biopsy, 18 (78%) had a true positive core biopsy. Three lesions with a false negative core biopsy were imaging discrepant and excision was recommended. Only two of the 23 (8.7%) lesions were deemed concordant with a FA and were followed. When these lesions demonstrated size doubling (100% growth) at the first imaging follow-up, they were then excised and shown to be benign PTs. None of these growing FAs were determined to be malignant PTs. All malignant PTs were correctly diagnosed by core biopsy.
Diligence is required of the breast interventionalist. When core biopsy results are discordant with imaging, repeat core or surgical excision is warranted. Early papers on the incidence of epithelial malignancy in FAs in the surgical/pathologic literature do not include imaging features, and therefore do not address imaging discordance. Correctly managing discordant pathology results mitigates the effect of a falsely benign biopsy
Vade et al. (14) assessed the role of sonography in the diagnosis and management of solid masses in adolescents (ages 13–19 years) in 2008. They found that US could not predict a specific histology, but considering the extremely low incidence of breast cancer in adolescence and the accuracy of Stavros sonographic criteria for prediction of benignity (15), conservative management of sonographically benign lesions in the adolescent is recommended unless the lesion exhibits “progressive growth” or the patient has a history of primary malignancy. US-guided core biopsy was not utilized in this series, presumably because of the age of the patients. At our institution, adolescents are routinely cored (as young as 11 years) if they (and their parents) are amenable to the procedure.
Why is this report relevant to the breast radiologist since no new “imaging” findings have been presented? The breast interventionalist, with increasingly sophisticated imaging tools, must act as the managing breast clinician and analyze concordance between pathology results and imaging findings.
We suggest that there is no size threshold above which a lesion should bypass core biopsy and go straight to surgery. Even considering the average larger size of PTs compared to FAs (15.6 vs. 37 mm), core biopsy is a valid first step, since surgical excision of any PT requires wide excision and preoperative diagnosis will help preserve breast tissue in patients with large FAs. We cautiously suggest that once an FA is diagnosed by core biopsy, no specific follow-up is required, considering the negligible rate of either developing malignancy or conversion to benign PT.
We acknowledge some limitations to our review. Since the incidence of epithelial pathology in cored nodular FAs was 0.58%, 173 growing FAs would be required to document just one epithelial malignancy if the incidence of pathologic abnormalities were equal. However, we speculated that the subset of growing FAs should have a modestly higher rate of epithelial malignancy, but this appeared not to be true (0% vs. 0.58%). Also, we do not have data on many of the patients with core biopsy-proven FAs lost to follow-up and, therefore, and cannot know how many of their lesions grew. However, we would not be surprised if a very large percentage of them did grow. We feel safe in assuming, though, that if major errors in diagnosis had occurred, the legal system would have brought them to our attention.
In conclusion, with proper core biopsy technique and adequate sampling, FAs with epithelial malignancy may be identified, at an approximate rate of 0.58% and should be excised. The largest risk, albeit low, in the growing FA is misdiagnosing a benign PT since malignant PTs, while rare, are readily diagnosed by core biopsy. Finding an epithelial malignancy in a growing FA is rare, and we identified no cases in which this occurred. For growing FAs, our data suggest that a repeat core biopsy, not excision, is a reasonable approach to exclude progression to PT, provided imaging is concordant. Surgery is not warranted, and creates distorting scars which may mask developing malignancy. Additional studies providing long-term follow-up of biopsied FAs would be helpful to confirm this approach.
Footnotes
Conflict of interest
None declared.