
Abstract
Idiopathic herniation of uncus and parahippocampal gyrus into the ambient cistern is a very rare entity, which could be mistaken for other pathology such as tumor. To the best of our knowledge, two prior cases of this kind of herniation have been described. One of these cases was with associated symptomatology and other abnormalities, and the other was characterized as idiopathic. In this case report, we report a case of accidental finding of a herniation of uncus and parahippocampal gyrus into the ambient cistern, without any other accompanying abnormalities, well depicted by magnetic resonance imaging without further necessity for surgical brain intervention.
Keywords
Introduction
Acquired brain herniation represents a forced mechanical displacement of a part of normal brain tissue into adjacent anatomical spaces due to a mass effect from traumatic injury, tumor, hemorrhage, infection, et cetera. This type of herniation is a well-known phenomenon. In this short report we present an extremely rare type of herniation of uncus and parahippocampal gyrus, which is not caused by a secondary mass effect but must be considered to be idiopathic.
Case report
A 46-year-old man was admitted to the Department of Neurology at Aalborg University Hospital with sudden onset of right-sided peripheral facial nerve palsy. His past medical history included left-sided peripheral facial nerve palsy 4 years previously for which no secondary cause was found. Hence, he was diagnosed with Bell’s palsy and achieved full recovery. Prior to the current facial nerve palsy there was no history of brain trauma, surgery, or medical illness. When informed of the abnormality, he admitted that for the past few years he had had intermittent pain located to the occipital region and neck muscles on the left side. On physical examination he had sore neck muscles on the left side. Neurological examination revealed no other neurological abnormalities except the right-sided facial nerve palsy. The remaining cranial nerves were intact. Blood samples were normal and investigations for Borrelia burgdorferi (Lyme disease) were negative. The cerebrospinal fluid was without pleocytosis.
During the current hospitalization magnetic resonance imaging (MRI) was performed before and after intravenous contrast agent administration. Images showed no pathology of the facial nerve neither on the right nor on the left side, but a sausage-shaped space-occupying soft tissue located in the ambient cistern was observed. This tissue had similar signal intensity as brain parenchyma in all sequences. An additional three-dimensional (3D) T1 sequence (BRAVO) with 1 mm slice thickness on a 1.5 T machine (GE Healthcare, Milwaukee, WI, USA) was performed, which very clearly illustrated full continuity from the tissue to the uncus and parahippocampal gyrus, and with clear separation of white and gray matter (Fig. 1). Images nicely depicted how mesial temporal parenchyma crawl on the edge of the tentorium and settles subtentorially in ambient cistern (Fig. 2). There was not observed any signal change either in herniated temporal tissue or adjacent mesencephalon tissue. Although there was a slightly larger distance between the medial edge of the tentorium and mesencephalon because of the herniated brain tissue, the images showed no abnormality in the dura or tentorium, which was symmetrical on both sides. During the previous hospitalization 4 years earlier a computed tomography (CT) scan of the cerebrum was carried out, in which one barely recognize herniation of the parahippocampal gyrus (Fig. 3).
A 1 mm slice thickness axial 3D T1-weighted image shows continuity from the herniated tissue (arrow) to the uncus and parahippocampal gyrus, with clear separation of white and gray matter. A coronal T2-weighted image, which shows nicely how, mesial temporal parenchyma (arrow) crawling on the edge of the tentorium and settles subtentorial in ambient cistern. An axial CT scan of the cerebrum, performed 4 years earlier, on which one could recognize the MRI verified herniation of left parahippocampal gyrus (arrow).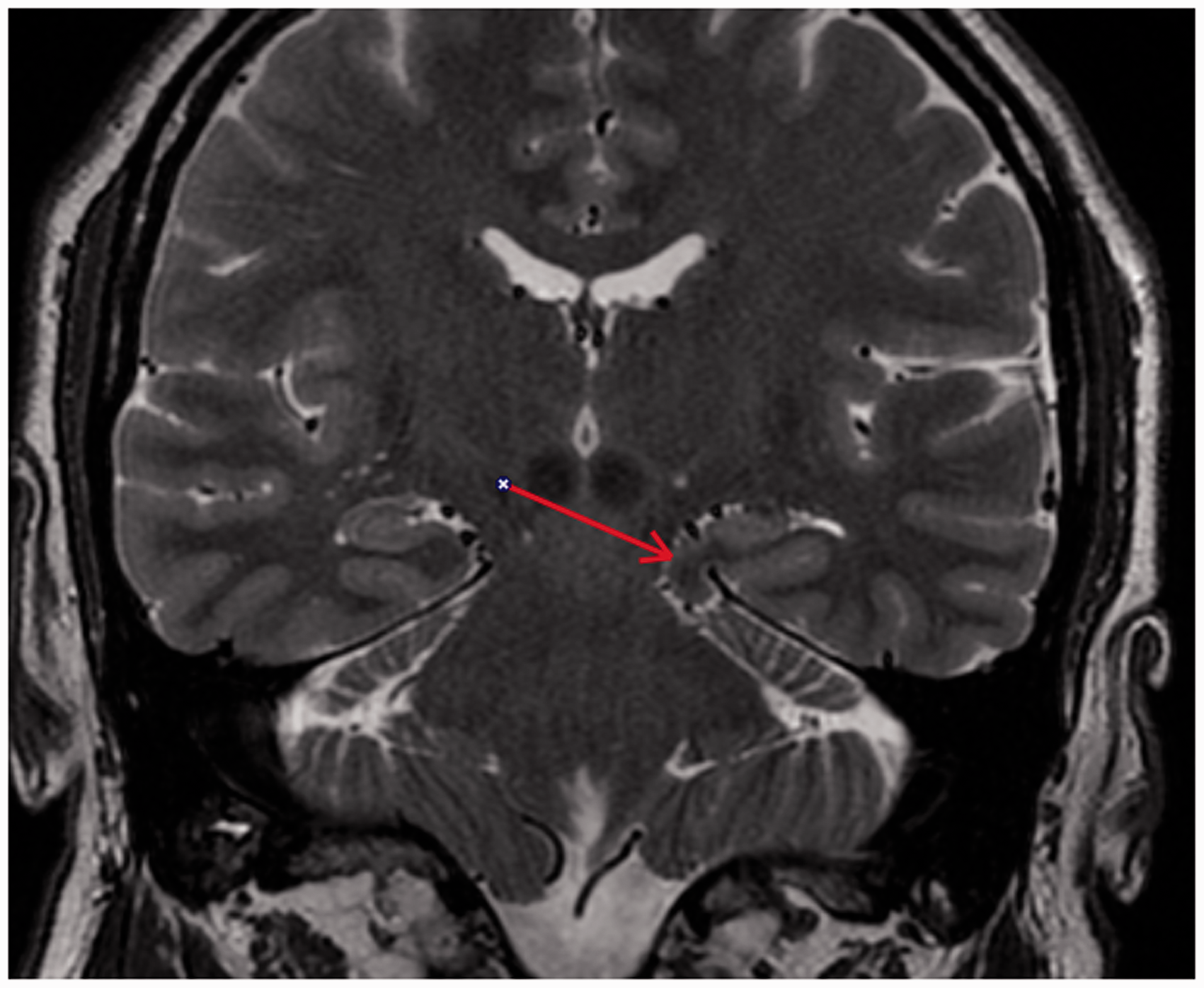


Discussion
Brain herniation can have several causes, e.g. tumors, trauma, ischemia, and infections. However, idiopathic gyral herniation is very rare and to the best of our knowledge only two cases have been reported.
The first reported case by Horowitz et al. involved a patient with atypical trigeminal neuralgia, who was found to have a parahippocampal herniation which was at first misinterpreted as a tumor (1). The second reported case by Duarte et al. involved a patient with chronic migraine-type headache, who was found to have a small parasagittal meningioma and a herniation of the uncus gyrus that was assumed to be congenital (2). In the latter case report, the authors proposed that the gyral herniation could be a plausible etiology for the headache, but that the herniation could also be either caused by the meningioma or be unrelated to the findings altogether.
Likewise, our patient also reported a history of headache. We considered that his headache and neck pain were unrelated to the gyral herniation since the pain seemed to have a muscular component. However, causality between the MRI findings and the headache cannot be quite ruled out, since the gyral herniation did not impinge on the facial nerve and could not explain the facial nerve palsy and could not even reach the trigeminal nerve. Because of location one could imagine that the trochlear nerve could be affected by the herniation, but a careful eye examination showed no clinical signs of trochlear nerve involvement.
In the above mentioned cases herniation was accompanied by other abnormalities. In the first case, with Chiari I malformation and very caudal transverse sinus and tentorium (1). In the second case, herniation was accompanied by a focal dural defect (2). Although it is reasonable to believe that this kind of anomaly is congenital and an embryonic meningial defect during embryogenesis of the developing meninges may allow herniation of parahippocampal gyrus in to the ambient cistern (2), in our case however we have not identified any accompanying intracranial abnormalities neither of the tentorium nor elsewhere.
In conclusion, a parahippocampal gyrus herniation may be misinterpreted as a tumor. It is important for radiologists to be able to recognize such abnormalities to avoid unnecessary interventions.
Footnotes
Conflict of interest
None declared.