
Abstract
A case of isolated sphenoid fungal sinusitis in an elderly diabetic patient is described. A coexisting mass lesion located in the sellar region was detected incidentally. Coincidence of these two entities represents a potential surgical disaster which may result in direct intracranial spread of fungal infection.
Keywords
Introduction
Herein we describe a case of isolated sphenoid fungal sinusitis in an elderly diabetic patient. Coexisting mass lesion located in sellar region was detected incidentally.
Fungal sinusitis is an important cause of morbidity and mortality in patients whose host defences have been altered by primary disease or immunosuppressive therapy.
High index of suspicion prompt intervention and aggressive therapy are required to prevent complications arising from extensions of these lesions beyond the paranasal sinuses.
Preoperative imaging plays an important role in defining the extent of the disease and in detection of any coexisting lesions of concern.
Case report
A 72-year-old woman was referred to our department by a neurologist with a history of diabetes mellitus and hypertension. The patient had been suffering from headache for the past 8 months. The headache was throbbing and deep seated in nature. The physical examination and laboratory work-up were unremarkable with the exception of a slight increase in glycosylated hemoglobin indicating poor regulation of the blood glucose levels. The patient had used conventional analgesics and various other drugs for the past 3 weeks with no effect. There were no sinonasal symptoms like postnasal dripping, nasal discharge, or obstruction.
Nasal endoscopy revealed a small polypoid mass protruding from the ostium of the
sphenoid sinus. Computed tomography (CT) scan of the paranasal sinuses showed
opacification of the left sphenoid sinus containing calcifications and mucosal
thickening on the right side (Fig.
1). Coronal images displayed in soft tissue window settings reveal a
suspicious low attenuating mass lesion located in the sellar region (Fig. 2). Magnetic resonance
imaging (MRI) was performed to rule out possible intracranial extension of sphenoid
sinusitis and to evaluate coexisting masses in the sellar area. The left half of the
sphenoid sinus was of low to intermediate signal intensity on T1-weighted (T1W)
images and appeared with signal void on T2-weighted (T2W) images consistent with
fungal sinusitis (Figs. 3
and 4). The fungal disease
appeared to be confined to the sphenoid sinus without any sign of intracranial
involvement. A dynamic MRI study was undertaken to evaluate the pituitary gland and
the mass lesion located in the right half of the cella. The mass lesion incidentally
detected on the CT scan showed homogenous contrast uptake on late phase dynamic MR
images and a dural tail was apparent on sagittal images suggesting the diagnosis of
a meningioma. However, the mass lesion could not be differentiated from the
pituitary gland. It was seated in the right half of sella turcica and extended to
the suprasellar region where it pushed the right half of the optic chiasma
superolaterally. Differential diagnosis included macroadenoma of the pituitary gland
(Figs. 5 and 6). It is worth noting that
despite the indentation of the chiasma, the patient’s sight was not affected and
headache was the only symptom. Axial unenhanced CT scan showing
opacification of the left sphenoid sinus; calcifications are
noted. Coronal CT image with soft tissue window settings:
A suspicious mass lesion occupying the right half of the sellar region
is seen. Axial T1W image showing the hypointense lesion
filling the left sphenoid sinus. T2W image on the same level as Fig. 3:
characteristic signal void appearance of fungal sinusitis is seen in the
left sphenoid sinus. Signal void on the right side represents
air. Contrast-enhanced coronal T1W image demonstrates
homogenous enhancement of the intrasellar mass lesion and extension to
the suprasellar cistern. Indentation of the optic chiasma is
noted. Contrast-enhanced sagittal T1W image: dural tail
is seen anteriorly. Marked enhancement in the sphenoid sinus is also
evident.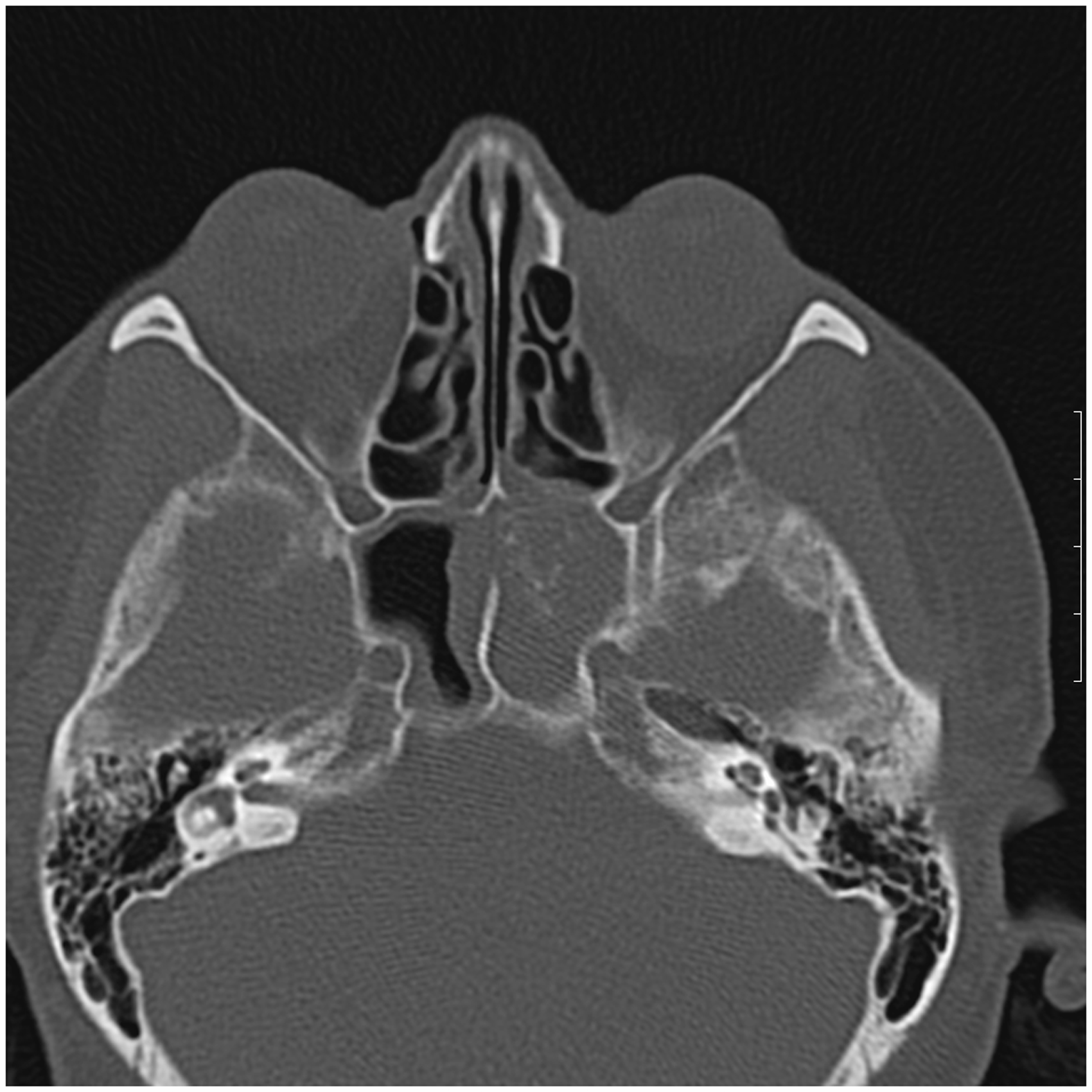





Endoscopic sphenoidotomy using transnasal approach was performed and a fungating mass was removed. The bony walls of the sinus were intact. Biopsies were taken from the sinus mucosa to rule out possible fungal invasion. Histopathologic evaluation demonstrated spore-forming structures confirming the diagnosis of fungal disease. Pathologic report stated healthy tissue margins confirming total excision of the fungal mass.
The patient was discharged the same day. On follow-up examination after 2 months
rhinoscopy was normal and CT scan confirmed a sphenoid sinus free of disease. The
patient’s headache still persisted but with decreased intensity. The incidentally
detected mass lesion is under follow
Discussion
Isolated sphenoid sinus disease (ISSD) is rare. Fungus ball is the third most common ISSD (1). In 2008 Socher et al. reported six cases of fungal sinusitis in a study involving 109 cases of isolated sphenoid sinus disease (2).
Various fungal diseases involve the sinonasal cavities. The most common and most important of these include mucormycosis, histoplasmosis, candidiasis, and diseases caused by Aspergillus (3). They all have propensity for invading blood vessels initiating thrombosis, which may lead to venous cerebral infarcts. Invasion of the orbits, cavernous sinuses, and ophthalmic veins is common. Sphenoid sinus is the least ventilated of the paranasal sinuses. Taking into account its close proximity to the major vessels located in the cavernous sinus, optic nerves, and skull base, it may serve especially in immunocompromised patients as an ideal gateway of pathogens to the CNS with possibly fatal consequences (4). Therefore mycotic infections of the paranasal sinuses have high morbidity rates and require prompt intervention by surgery or medical therapy.
Headache is the most commonly reported symptom of isolated sphenoid fungal disease. It may be accompanied by postnasal drips and facial pain, and in case of orbital complications, symptoms like diplopia and visual loss can be observed (5). In our case headache was the sole presenting symptom and the usual symptoms of sinonasal disease were absent as the infection was confined to the sphenoid sinus.
In most of the cases, imaging modalities establish the diagnosis and guide the therapeutic approach. The lack of air fluid levels and presence of calcifications on CT scan combined with signal void appearance on T2W images raises high suspicion for fungal disease. This signal void appearance can be attributed to the tendency of fungi to bind calcium, manganese, and other heavy metals (6). Our case demonstrated all the characteristic imaging findings mentioned above.
The goal of the surgery should be to remove all the fungal debris. The development of rigid nasal endoscopy has significantly reduced the operating time, morbidity, and hospitalization time (7).
If a fungal disease is suspected, the extent of the disease must be demonstrated preoperatively by imaging modalities as these lesions appear to be able to create bony destruction and spread to adjacent structures via invasion of blood vessels. Coincidence of other diseases with anatomical relevance to surgery are also documented by preoperative imaging and bear much importance since transsphenoidal approach is the preferred surgical technique for mass lesions located in the sellar area.
In conclusion, imaging modalities provide indispensable information in the preoperative planning.
Footnotes
Conflict of interest
None declared.