
Abstract
We present two cases of acquired uterine arterial venous malformation (AVM) which was diagnosed because of massive genital bleeding successfully treated with transcatheter arterial embolization (TAE), using N-butyl-2-cyanoacrylate (NBCA) under balloon occlusion. Balloon occlusion at the uterine artery was performed in both patients for diffuse distribution of NBCA in multiple feeding branches, as well as to the pseudoaneurysm, and for the prevention of NBCA reflux. In one of our patients, balloon occlusion of the draining vein was simultaneously performed to prevent NBCA migration through accompanying high-flow arteriovenous fistula (AVF). Doppler ultrasound at 6 months of both patients documented persistent complete occlusion of AVM. Complete and safe obliteration of acquired uterine AVM was accomplished using NBCA as embolic agent, under balloon occlusion at the communicating vessels of acquired uterine AVM.
Introduction
Acquired uterine arterial venous malformation (AVM) is a rare cause of obstetric hemorrhage. Uterine trauma has been identified as the cause of uterine AVM, including dilatation and curettage Cesarean section, previous uterine surgery, gestational trophoblastic disease, and other gynecological malignancies, such as carcinoma of the cervix and endometrium. Heavy vaginal bleeding is the common manifestation and could be life-threatening. Treatment options include hysterectomy, ligation of one or both uterine arteries, and, more recently, percutaneous transcatheter arterial embolization (TAE). TAE is less invasive and has the potential to preserve fertility, compared with surgical management. The treatment for acquired uterine AVM has been shifting from surgical operation to TAE (1).
Herein, we report two cases of acquired uterine AVM successfully treated with TAE using N-butyl-2-cyanoacrylate (NBCA), under arterial and venous balloon occlusions. A number of studies have investigated the use of TAE to treat uterine AVM (1–5). Kitagawa et al. performed ethanolamine oleate sclerotherapy under venous balloon occlusion, combined with transarterial embolization using NBCA for uterine AVM (6). However, to our knowledge, our cases are the first report of TAE under arterial balloon occlusion for acquired uterine AVM.
Case reports
Case 1
A 33-year-old woman with genital massive bleeding was admitted to our hospital.
She had undergone dilatation and curettage for a missed abortion 24 days earlier
at the first pregnancy. Doppler ultrasound revealed a large pseudoaneurysm on
the left side of the uterus, with blood flow from both uterine arteries.
Arterial-phase dynamic contrast computed tomography (CT) imaging showed a
homogeneously-enhanced mass lesion in the uterus communicating with dilated both
uterine arteries (Fig.
1a). Early enhancement of the right internal iliac vein was also
noted. Accordingly, an acquired uterine AVM with pseudoaneurysm and
arteriovenous fistula (AVF) was considered. She was referred to angiography for
TAE. An informed consent was obtained by one of the authors. A 33-year-old woman with excessive genital
bleeding 24 days after dilatation and curettage (D&C). (a) A CT
image at arterial phase shows a uniform mass -like enhancement in
the uterus which represents a pseudoaneurysm. (b) DSA from the left
uterine artery shows multiple feeding arteries connecting to the
pseudoaneurysm in the uterus. Direct draining from the
pseudoaneurysm to the uterine vein is simultaneously demonstrated
(arrow). (c) Diffuse distribution of NBCA is demonstrated on DSA
after TAE with NBCA. Disappearance of AVM enhancement is
confirmed.
The procedure was performed under local anesthesia. Sheaths (5 F) were introduced bilaterally at the common femoral arteries. Digital subtraction angiography (DSA) from the left uterine artery by using a 5.2-F balloon catheter (Selecon MP Catheter II, Terumo Clinical Supply Co., Ltd., Gifu, Japan) inserted from the right sheath showed enhancement of multiple arterial branches communicating to a pseudoaneurysm in the uterus, which drained directly into the right uterine vein (Fig. 1b). Meanwhile, a DSA from the right uterine artery did not show communication with the AVM; although, massive proliferation of arcuate arteries of the right uterine artery was identified. Accordingly, the left uterine artery was occluded using a 5.2-F balloon catheter (Selecon MP Catheter II, Terumo Clinical Supply Co., Ltd., Gifu, Japan) to inject NBCA into the pseudoaneurysm through multiple arterial supplies, and to prevent NBCA reflux. The right internal iliac vein was simultaneously occluded with a 7-F balloon catheter (Selecon MP Catheter II, Terumo Clinical Supply Co., Ltd., Gifu, Japan) inserted from the left femoral vein to prevent migration of NBCA into the vein though AVF. After confirmation of stasis and pooling of contrast material in the AVM under balloon occlusions of the artery and vein at the test injection, a 0.6-mL suspension of NBCA and Lipiodol (1/6) (Laboratoire Guerbet, Roissy, France) was introduced through a microcatheter (1.9F GOLD CREST, Koshin Medical, Tokyo, Japan) and co-axially inserted into the balloon catheter of the left uterine artery until NBCA filled the feeding arteries and reached the pseudoaneurysm. Subsequently, a small amount of gelatin sponge particles (2 mm in size) and contrast material mixture was introduced through a 5-F cobra-shaped catheter positioned at the right uterine artery until the flow of the right uterine artery became sluggish. DSA from both common iliac arteries after embolization showed obliteration of AVM and AVF (Fig. 1c). The blood flow to the uterus was maintained through collateral arteries. No adverse effects occurred during or after the TAE procedure. Contrast-enhanced CT images taken 2 days after the TAE procedure revealed no sign of AVM recurrence, and no migration of NBCA in the vein. The patient’s recovery was uneventful, and she was discharged on postoperative day 8. Six months after the TAE procedure, clinical and ultrasound examinations confirmed obliteration of AVM. She had resumed a normal menstrual cycle 1 month after TAE.
Case 2
A 30-year-old woman was referred to our hospital for repeat genital bleeding. She
had chorioamnionitis and threatened premature delivery 40 days earlier at the
first pregnancy. Color Doppler sonography revealed a low echoic lesion with
turbulent flow in the uterus. Magnetic resonance imaging (MRI) showed a mass
lesion of high signal intensity in the uterus on a short inversion-time
inversion recovery (STIR) image. No flow void was observed in the uterus on
T2-weighted (T2W) images (Fig.
2a). A fat-suppressed T1-weighted image of the early phase after
gadolinium injection showed the dilated left uterine artery and its branches
communicating with a homogeneously-enhanced mass lesion at the left side in the
uterus. Accordingly, acquired uterine AVM with a pseudoaneurysm was considered.
An informed consent was obtained by one of the authors. A 30-year-old woman with repeat genital
bleeding after threatened premature delivery. (a) A coronal T2W
image of the uterus shows a high signal intensity mass lesion at the
left side in the uterus (arrows). There is no signal void observed.
(b) DSA from the left uterine artery shows a pseudoaneurysm, with
two compartments, accepting blood flow from multiple feeding
arteries. (c) Complete obliteration of AVM is demonstrated on DSA
after TAE using NBCA under balloon occlusion of the left uterine
artery.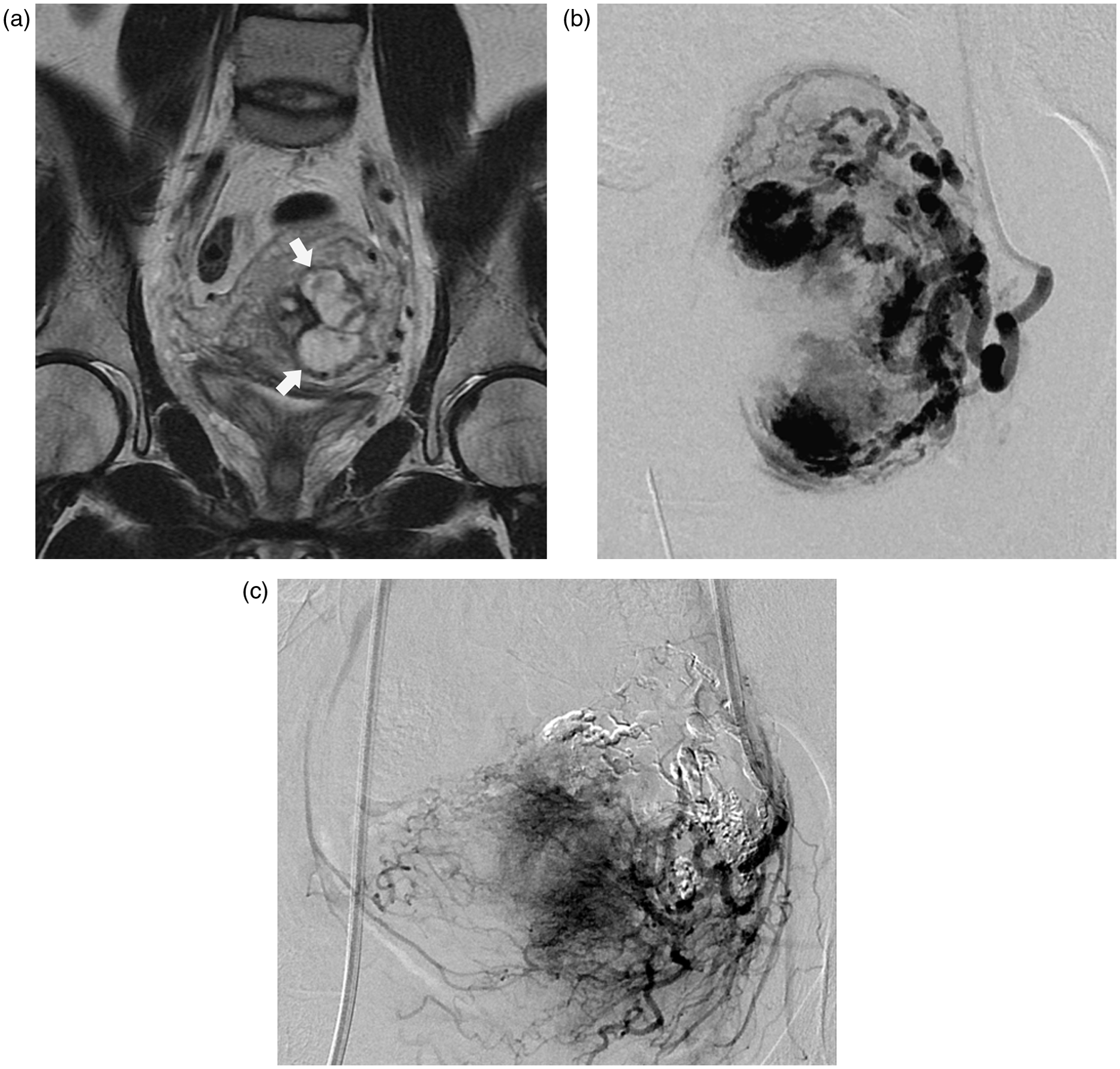
The procedure was performed under local anesthesia. Angiography was achieved with a 5-F sheath inserted through the right common femoral artery. DSA from the left internal iliac artery revealed dilated and proliferated branches of the left uterine artery supplying the pseudoaneurysm in the uterus (Fig. 2b). The blood flow towards the pseudoaneurysm did not appear to be particularly fast, as the aneurysm showed gradual enhancement during the DSA procedure, which was concordant with the findings of MRI, showing no flow void on T2W images. Accordingly, TAE using low-concentrated NBCA under balloon occlusion of the left uterine artery was attempted, with the purpose of filling the proliferated branches with NBCA, as well as the pseudoaneurysm, before polymerisation of NBCA, as well as to prevent NBCA reflux. A 3-F microballoon catheter (Attendant- LP, Terumo Clinical Supply Co., Ltd., Gifu, Japan), co-axially inserted into a 5-F guiding catheter (Elway, Terumo Clinical Supply, Tochigi, Japan) from the right sheath, was inflated at the main trunk of the left uterine artery. A 0.5-mL suspension of NBCA and Lipiodol (1/6) was introduced though the microballoon catheter until NBCA was distributed through the feeding arteries and the pseudoaneurysm was filled. Subsequent DSA from the right uterine artery showed dilatation of the arcuate branches of the uterine artery; although, there was no communication with the pseudoaneurysm. A small amount of gelatin sponge particles (2 mm in size) mixed with contrast material was injected through a 5-F cobra-shaped catheter placed at the right uterine artery. Finally, DSA from bilateral uterine and internal iliac arteries confirmed the complete absence of AVM (Fig. 2c). No complications were evident during or after embolization. The patient was discharged on postoperative day 4. The disappearance of AVM was confirmed by Doppler ultrasound at the 6-month follow-up visit after embolization. The patient had resumed a normal menstrual cycle 1 month after treatment.
Discussion
As described previously, acquired uterine AVM tends to represent a single connection between an artery and a vein without a nidus (1). However, our cases demonstrated complex features, with multiple feeding arterial branches communicating with the pseudoaneurysm in both cases, and accompanying AVF in one of the cases. TAE for AVM with complicating forms may need technical modification, as complicated AVM may have a possibility of recurrence due to recanalization of AVM or the development of new feeding arteries, due to proximal embolization, or incomplete obliteration of the feeding arteries and nidus. The outcome of TAE for AVM depends on both the embolization technique and the embolic material.
Balloon-assisted arterial embolization has been reported previously in cerebral AVM, hepatocellular carcinoma, and pseudoaneurysm at the femoral artery (7–11). In contrast, balloon-assisted arterial embolization for uterine-acquired AVM has not been reported previously. In our series, balloon occlusion at the main trunk of the uterine artery was considered useful, because it allowed NBCA to penetrate into the AVM, and prevented retrograde reflux of NBCA. One of our cases, case 1, presented an AVM accompanying AVF and had a possible risk of pulmonary embolization if the embolic material passed though the AVF. Incidents of fatal pulmonary embolization and paradoxical arterial embolization via an intrafibroid AVF during uterine fibroid embolization using microparticles have been reported (12). In our case, the accompanying AVF seemed sufficiently large to allow passage of the embolic material. Moreover, the NBCA concentration used was low for the aim of diffuse distribution in the feeding arteries. Therefore, NBCA with low concentration could migrate into the vein trough AVF more easily, without polymerization. Van Rooij et al. presented a successful embolization of intracranial high-flow AVF under arterial microballoon occlusion to control the blood flow (8). Mansueto et al. reported successful NBCA embolization of a high-flow renal AVF under flow control with balloon occlusion of the draining vein (13). Mori et al. demonstrated excellent packing of the high-flow renal AVF with a detachable coil, under balloon occlusion of the draining vein (14). In our case, the simultaneous balloon occlusion of the feeding artery and draining vein allowed us to control the distribution of NBCA with flow stagnation and to ensure the prevention of NBCA migration into the draining vein. Smaller microballoon catheters that allow passage through a diagnostic catheter at the body trunk have recently become available. Irie et al. demonstrated the usefulness of transcatheter arterial chemoembolization (TACE) using microballoon occlusion. In this report, the dense accumulation of lipiodol emulsion in a hepatocellular carcinoma (HCC) nodule was noted (7). A microballoon catheter demonstrated satisfactory trackability at the tortuous uterine artery in case 2, which would not allow a 5.2-F balloon catheter to pass through. The quality improvements and wide range of choices in balloon catheters may expand the application of balloon-assisted embolization and may contribute to better outcomes and safer procedures.
The outcome of our cases without balloon occlusion could be also successful. However, there will be a higher risk of recurrence without balloon occlusion because of incomplete obliteration of the feeding arteries and nidus. We selected NBCA as an embolic material for robust and long-time packing of AVM. However, there was a conceivable risk of proximal embolization with early polymerization of NBCA before reaching the pseudoaneurysm. Another concern was the adhesion of NBCA on the occlusion balloon catheter, followed by unwanted arterial embolization with reflux of NBCA during catheter withdrawal, or adhesion between the vessel wall and inflated balloon, resulting in vessel injury or rupture of the catheter. To prevent these adverse events, a low concentration of NBCA was prepared to extend the polymerization duration. Longer polymerization times allow the operator to carefully control the extent of NBCA, and to avoid contact between the balloon and NBCA with properly-timed dextrose solution flushing after injection of NBCA. There was no adhesion observed between NBCA and the balloon, or the balloon and the vessel wall during our procedures. Sonomura et al. reported about the possibility of uterine damage at uterine artery embolization with NBCA in comparison with gelatin sponge on the swine model (15). The pregnancy after NBCA had been shown by several reports (16,17). However the risk of uterine damage by NBCA has to be kelp in mind.
Onyx is another choice of embolic material for our cases. Onyx may allow prolonged injections and, therefore, better nidus penetration without causing an immediate obliteration of the vessel. However, Onyx will need longer procedure time resulting in more radiation, and is more expensive. Moreover, Onyx was not available for us to use in our institution. Microparticles are one of the common choices for embolization of AVM. However, the use of microparticles for AVF may cause critical complications including pulmonary embolization and paradoxical embolization (12). The larger particle for AVF may be safer but it may occlude the arteries proximally and may result in recurrence of AVM. Maleux et al. had chosen the microparticle size from 250 µm to 900 µm to treat AVF (4). However, there are no criteria regarding the size of the particle for embolization of uterine AVF. The size of microparticles for AVM and AVF depends on the size of the afferent arteries and is at the discretion of the interventional radiologist who performs embolization.
In conclusion, application of balloon occlusion for TAE of acquired uterine AVM contributed to complete and safe embolization of AVM complex configurations. TAE for acquired uterine AVM requires appropriate strategies regarding the choice of device and embolic material, which are based on the assessment of the hemodynamics, configuration, and vessel size of the AVM.
Footnotes
Conflict of interest
None declared.