
Abstract
Inflammatory myofibroblastic tumors (IMT) are a benign tumor entity, which rarely develop in the liver. Surgery is the most common treatment for these lesions as it is difficult to distinguish them from malignant liver tumors and local recurrent growth may occur. IMT is a diagnostic challenge for imaging. Only a limited number of reports of single cases or small number of patients described the imaging features on computed tomography. Reports on IMT appearance on magnetic resonance imaging are scarce. We present a case of IMT of the liver with infiltration of the abdominal wall treated with surgery and describe the imaging features with the use of the hepatobiliary contrast agent, gadoxetic acid (Gd-EOB).
Introduction
Inflammatory myofibroblastic tumors (IMT), in the past also referred as inflammatory pseudotumors, are mass-forming neoplastic lesions, which develop in almost every organ such as lung, kidney, ovary, pancreas, spleen, breast, in the abdominopelvic region and retroperitoneum (1–4). The first recognition in the literature of this entity as a pulmonary mass with necrosis and hemorrhage was in 1953 (5). IMT affects patient of any age, but with a predilection for children and young adults (6). The incidence of IMT in the liver is low. However, it was observed in 1% of 403 patients who underwent surgery for focal liver lesions, which makes it an important differential diagnosis in of liver lesions (7).
IMT of the liver remain a challenging diagnosis due to their low incidence. Malignant features in radiological imaging techniques make them difficult to distinguish from other hepatic malignancies (8). Sonography and computed tomography (CT) appearances are described but these methods do not allow to clearly differentiating IMT in the liver from malignancies such as metastases or primary liver cancers. There are reports of findings of IMT in magnetic resonance imaging (MRI), but insufficient to complete a specific imaging profile of this entity. Herein we report a case of IMT of the liver, which was imaged with CT and MRI with the use of gadoxetic acid (Gd-EOB) as a hepatobiliary contrast agent.
Case report
A 67-year-old woman presented with worsening diffuse upper abdominal pain. The medical and surgical history was unremarkable besides an uncomplicated dorsal stabilization of lumbar spondylolisthesis several years ago. Physical examination revealed moderate diffuse abdominal tenderness, greatest over the epigastric region. The initial sonography of the abdomen by a private practitioner (no images available) found a heterogeneous hypoechogenic tumor in the left liver lobe. The patient was then referred to us for further investigation and management. Upon admission both gamma-glutamyl-transpeptidase and C-reactive protein were elevated while other blood tests (white cell count, serum electrolytes, prothrombin time, bilirubin, hepatic transaminases) and alkaline phosphatase levels, hepatitis serology Ca19-9, carcinoembryonic antigen, and alpha fetoprotein were within the normal ranges.
CT abdomen (triple-phase contrast protocol) showed a contrast enhancing mass
(diameter, 65 mm) with irregular confluent non-enhancing areas in the center with a
hypodense late enhancing 10–15 mm rim and no wash-out in the late phase images. The
tumor was located in segment IV of the liver crossing the middle hepatic vein and
the borders to the left lateral sector with bile duct dilation in the left lateral
liver segments. Additionally minimal pleural effusion was present (Fig. 1). Contrast-enhanced triple phase CT of the liver
showing the heterogeneously defined mass with initially centric in the
arterial (upper) and portal venous phase (middle) and delayed peripheral
enhancement in the late venous phase (lower), leaving confluent areas
without contrast uptake in the center of the lesions. Note the dilated
bile duct on segment II and the close relationship to the anterior
abdominal wall suggestive for transcapsular
growth.
For further preoperative evaluation, an abdominal MRI (1.5 T; Gyroscan ACS-NT;
Philips Medical Systems, Best, The Netherlands) of the liver was performed 12 days
later with unenhanced T1-weighted (T1W) and T2-weighted (T2W) images with and
without fat suppression and contrast-enhanced sequences using Gd-EOB-DTPA
(Primovist; Bayer Healthcare, Berlin, Germany) as liver specific contrast agent.
Early dynamic T1W images were acquired first and delayed hepatobiliary imaging after
20 min (T1W fat-saturated sequences). The examination demonstrated a lesion which
was adherent to the abdominal wall and right diaphragm. In the T1W images the lesion
with irregular borders appeared hypointense and well defined without fatty
components. T2W images showed a heterogeneous slightly hyperintense lesion with an
ill defined moderately hyperintense rim. Similar to the early contrast phases in CT,
the dynamic images showed heterogeneous hyperperfusion in the central partition and
hypoenhancement in the peripheral rim of the tumor. In the hepatobiliary phase, the
lesion (center and rim alike) did not show contrast material accumulation and was
sharply delineated against the contrast enhanced liver tissue. Tumor borders were
irregular with small nodular extensions into the surrounding liver. No other hepatic
lesions were detected. The pleural effusions had resolved to a great part (Fig. 2). MRI of the liver shows a mild hyperintense mass in
segment IV adherent to the abdominal wall in T2W images (upper left).
The T1W images without (upper middle) and with fat suppression (upper
right) did not show methemoglobin or fatty components of the hypointense
lesion. The dynamic acquisition after intravenous Gd-EOB administration
in the arterial (lower left) and portal venous phase (lower middle)
demonstrated contrast enhancement first in the center and then in the
periphery of the mass. The sharpest demarcation of the mass with
irregular delineation and small extensions into the surrounding strongly
enhancing liver parenchyma is seen in the hepatobiliary phase 20 min
after injection of Gd-EOB (lower right).
There was no suspicion of an extrahepatic primary tumor in the diagnostic work-up,
which included colonoscopy and chest X-ray. With the strong suspicion of a hepatic
malignant tumor with ventral extension beyond the liver capsule, the patient
underwent a left hemihepatectomy with partial excision of the adherent abdominal
wall and diaphragm. Intraoperative histopathological analysis revealed necrotic
tissue with resolving granulocytes and proliferating fibroblasts in a scar rich
specimen but no malignant cells were present (Fig. 3). Microbiological cultures were
performed with no subsequent growth. The histopathological evaluation of the
specimen revealed a tumor with fibrosis and partially necrotic tissue infiltrated by
inflammatory cells, predominantly plasma cells, and also pigmented macrophages and
granulocytes. There was no evidence of infiltration of the portal fields and bile
ducts. The tumor appeared with a diffuse border of small nodular extensions into the
parenchyma. The final diagnosis was IMT without suspicion of malignancy. HE
Staining, 20 × magnification. Histology of surgical specimen showing
proliferating fibroblasts, vessels and inflammatory cells in scar rich
tissue. Loose areas of necrosis and hepatocytes without evidence of
cellular atypia. Pathologic diagnosis: inflammatory pseudotumor without
evidence of malignancy or cirrhosis.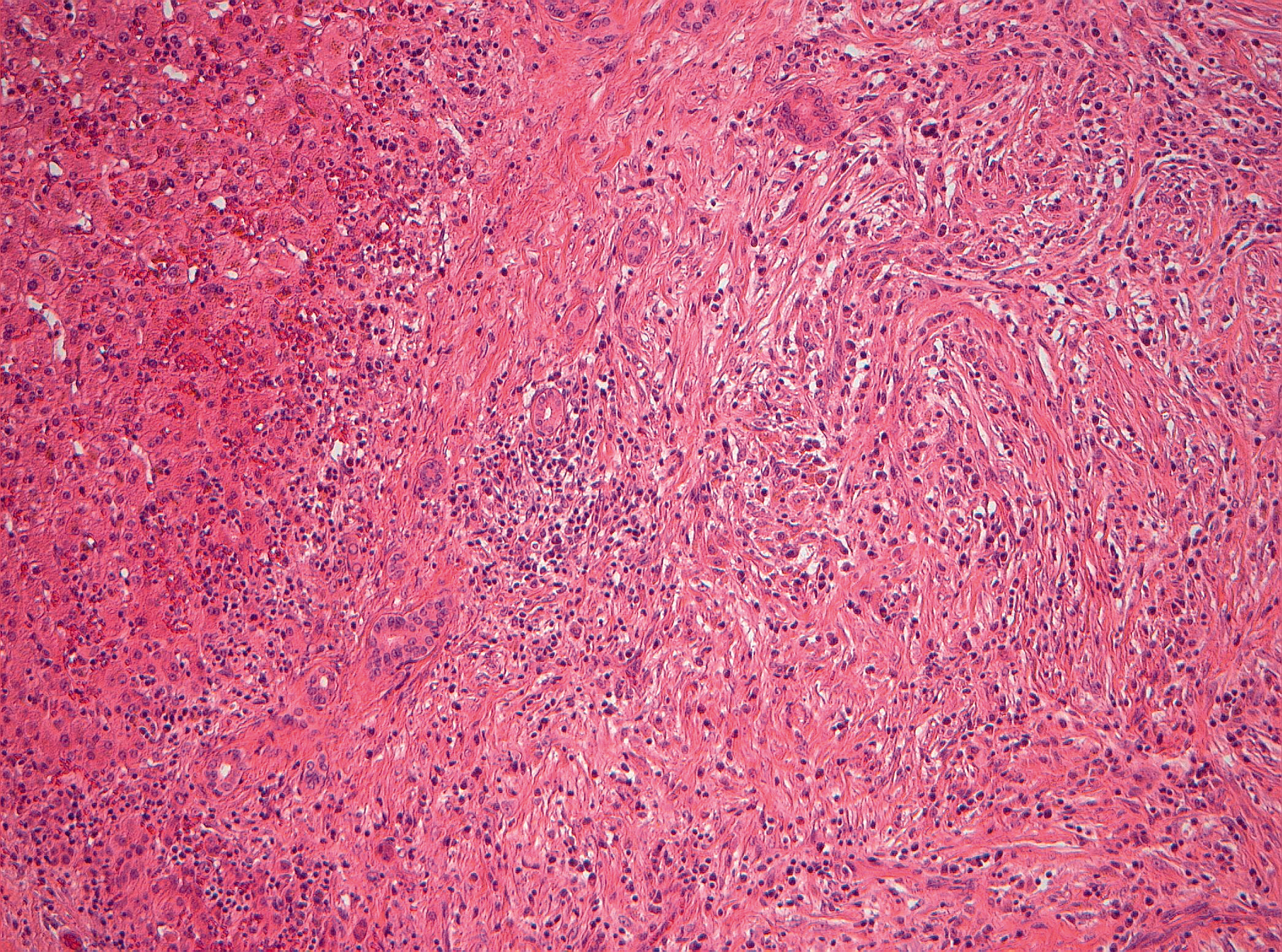
Discussion
IMT is generally considered as a benign entity, even though infiltrative growth is possible and local relapse may occur (9). Histologically these lesions are characterized by proliferating myofibroblastic spindle cells without cellular atypia with a prominent inflammatory infiltrate in fibrotic tissue (8). The infiltration is primarily composed of plasma cells and lymphocytes. Occasionally areas of necrosis and cell fraction of eosinophils and neutrophils are observed as well (1). It has been demonstrated that tumors matching histological features of IMT encompass entities of divergent biological behavior (10). The last World Health Organization classification ranges IMT as tumors of intermediate biological potential with possible local relapse (11). Whether additional lesions are metastases or multicentric IMT is not clear (12).
The etiology of IMT is not known. Sometimes IMT are associated with a trigger of inflammation such as foreign bodies, gall stones, or infections (8,13). In the present case, it is debatable whether the previous orthopedic surgery of the lumbar spine with metallic implants triggered a nonspecific inflammatory process, which might have caused the pleural effusion and the IMT of the liver. However, the theory of a true neoplastic etiology is strengthened by the presence of chromosomal rearrangements in the ALK gene on 2p23, which is why the term “pseudotumor” should be avoided (6,14). The detailed medical history of the present patient was unremarkable regarding potential causes for an IMT.
Surgery has a great importance in the therapeutic strategies of IMT treatment, which also comprise conservative treatment attempts with antibiotics, non-steroidal anti-inflammatory drugs, steroids and chemotherapeutics (15,16). Spontaneous complete regression of IMT has also been described (17). The prognosis of abdominal IMT that occur more often in younger patients (children and adolescents) is worse than that of thoracic IMT (predominantly occurring in elderly patients), because of the higher rate (30–35%) of local relapse (12). The most commonly chosen therapeutic approach is (if possible) surgery as IMT often mimics malignant tumors (8). This was the case for our patient as well. Even a biopsy would probably not have ruled out malignant disease, as IMT might be associated with malignomas or even rarer malignant de-differentiation of IMT, so called inflammatory fibrosarcomas (8,12). Therefore, distinction from a malignoma without examining the entire specimen is rather unsecure, which favors the surgical removal of IMT if possible. Furthermore, surgery has the advantage of very low recurrence rates after complete excision of IMT (17–21).
Possible differential diagnoses of the mass are primary hepatic tumors (e.g. hepatocellular carcinoma [HCC] or cholangiocarcinoma) or metastases as well as parasitic infection (echinoccocus), abscess, and hematoma. Clinical presentation, serology, and infection parameters did not favor parasitic infection, hematoma, or abscess, and the imaging appearance did not fit with these entities. Benign liver tumors such as hepatocellular adenoma and focal nodular hyperplasia (FNH) can be discussed as differential diagnosis. However, besides the lack of a number of morphologic features no fatty components or hemorrhages (sometimes seen in adenomas) or late enhancement of Gd-EOB (nearly always present in FNH) were present on the MRI images (22). The infiltrative behavior with crossing of the liver capsule and infiltration of the abdominal wall as well as the bile duct dilatation in the neighboring liver segments are highly suspicious for a malignoma. Previous reports showed that IMT of the liver are able to infiltrate the portal field (23). However, to the best of our knowledge there is no spontaneous IMT of the liver reported to infiltrate into the abdominal wall. MRI findings of the present case, even though matching with other reports of IMT (e.g. T1-hypointensity and T2-hyperintensity), are nonspecific to IMT of the liver (24–26). The contrast behavior with early enhancement of the central parts first and later in the hypodense rim of the mass without any wash-out in CT are rather atypical for cholangiocarcinoma, HCC, and metastases as these lesions usually present with an initial enhancement of the rim or the entire lesion. Additionally the hypodense non-enhancing areas (representing necrosis) as seen in the present case within the tumor are not a typical finding of primary hepatic malignomas and the tumor markers were negative.
Despite these findings, which are rather unusual for the common malignant diagnoses of focal liver lesions, the strong suspicion of a malignoma remained. The patient underwent partial liver resection for the strong suspicion of a primary hepatic malignancy as no extrahepatic primary was found in the preoperative work-up. The superficial infiltration into the neighboring diaphragm and the abdominal wall by the capsule penetrating hepatic mass was confirmed intraoperatively and the involved parts were excised en bloc with the specimen.
In conclusion, the differential diagnsois of this rare entity remains difficult. Beside other previously reported but rather non-specific and varying findings (24–26), we found small nodular extensions at the border of the lesion in the hepatobiliary phase of EOB-MRI as an additional and characteristic imaging feature of IMT, which could be a valuable criterion for imaging diagnsois if reproducible in other cases.
Footnotes
Conflict of interest
None declared.