
Abstract
Small bowel feces sign (SBFS) is a computed tomography (CT) finding that appears as fecal like material in dilated small bowel loops. This sign is usually seen in association with gradually progressive small bowel obstruction. We present a case of occlusive mesenteric ischemia in which the SBFS appeared on CT scan early on in the course of the disease. We put forward a suggested alternative mechanism to the appearance of this sign in association with mesenteric ischemia. The SBFS might have the potential to serve as an early sign of mesenteric ischemia on CT scan.
Introduction
Small bowel feces sign (SBFS) is a computed tomography (CT) finding that appears as
particulate, fecal-like material; mixed with gas bubbles in dilated small bowel
loops (1). This sign has
been frequently described in association with small bowel obstruction (SBO). There
are contradicting views on the prognostic significance of this sign in patients with
SBO. We present the first written description of the sign in association with
occlusive mesenteric ischemia. Initial CT study done within 6 h from
presentation. Coronal image in portal phase shows SBFS in a dilated
segment of the jejunum (arrows).
Case report
An 87-year-old Middle-Eastern man, with a medical history significant for chronic
atrial fibrillation, presented to the emergency department with complaints of severe
acute upper abdominal pain of 1 h duration. He reported no vomiting or change in
bowel movements. He did not reveal any previous history of postprandial abdominal
pain, food aversion, or weight loss. On examination, the patient had irregular
tachycardia (heart rate, 140 bpm), blood pressure was 164/95, temperature was
98.3°F. Abdominal examination was remarkable for tenderness in the left upper
quadrant accompanied by voluntary guarding. Bowel sounds were normal. Rectal
examination revealed no blood or melena, and stool sample for occult blood was
negative. White blood cell count was 14,600 with left shift. Blood chemistries
showed normal amylase and lipase levels, elevated serum lactate dehydrogenase (LDH)
(467 U/L; normal range, 72–182 U/L), and mild elevation in serum lactate
(2.41 mmol/L; normal range, 0.50–2.21 mmol/L) without metabolic acidosis. Acute
abdomen series X-rays showed no intramural, free peritoneal, or portal venous gas.
Portal phase, coronal image from the later CT
study. Note the filling defect in SMA (thin white arrow), SBFS (black
arrow), and feces in large bowel for comparison (white
arrow).
CT examination was performed on a 64-slice multidetector CT scanner (Discovery CT750
HD, GE Healthcare, Milwaukee, WI, USA). The study was performed following the
administration of 90 mL Iobitridol intravenous contrast medium (Xenetix300; Guerbet,
Roissy, France) bolus injection via a power injector at a rate of 3.0 mL/s. Images
were acquired in the arterial and portal phases. Acquisition was performed 30 s and
70 s from the start of injection for arterial phase and portal phase imaging,
respectively. Tube voltage was 120 kV, tube current 300 mA, collimation
64 × 0.625 mm, and slice thickness 5 mm. The CT study, which was performed within
6 h from presentation, revealed dilated (3.0–3.5 cm in diameter) jejunal loops
(Fig. 1). A 25 cm
segment of the distal jejunum was more dilated (3.5–4.0 cm in diameter) with SBFS.
There was no reduction in bowel wall enhancement. No arterial filling defect was
documented in the initial report but was noted retrospectively. A repeat CT scan
after 24 h showed a central arterial filling defect 6 cm from the origin of the
superior mesenteric artery (SMA) extending for 4 cm with minimal contrast filling in
the vessels distally (Figs.
2 and 3). The
dilated jejunal segment still had the same appearance with SBFS, but there was
obvious reduction in wall enhancement (Figs. 2 and 4). Arterial phase, axial image
from the later CT study show filling defect in SMA
(arrow).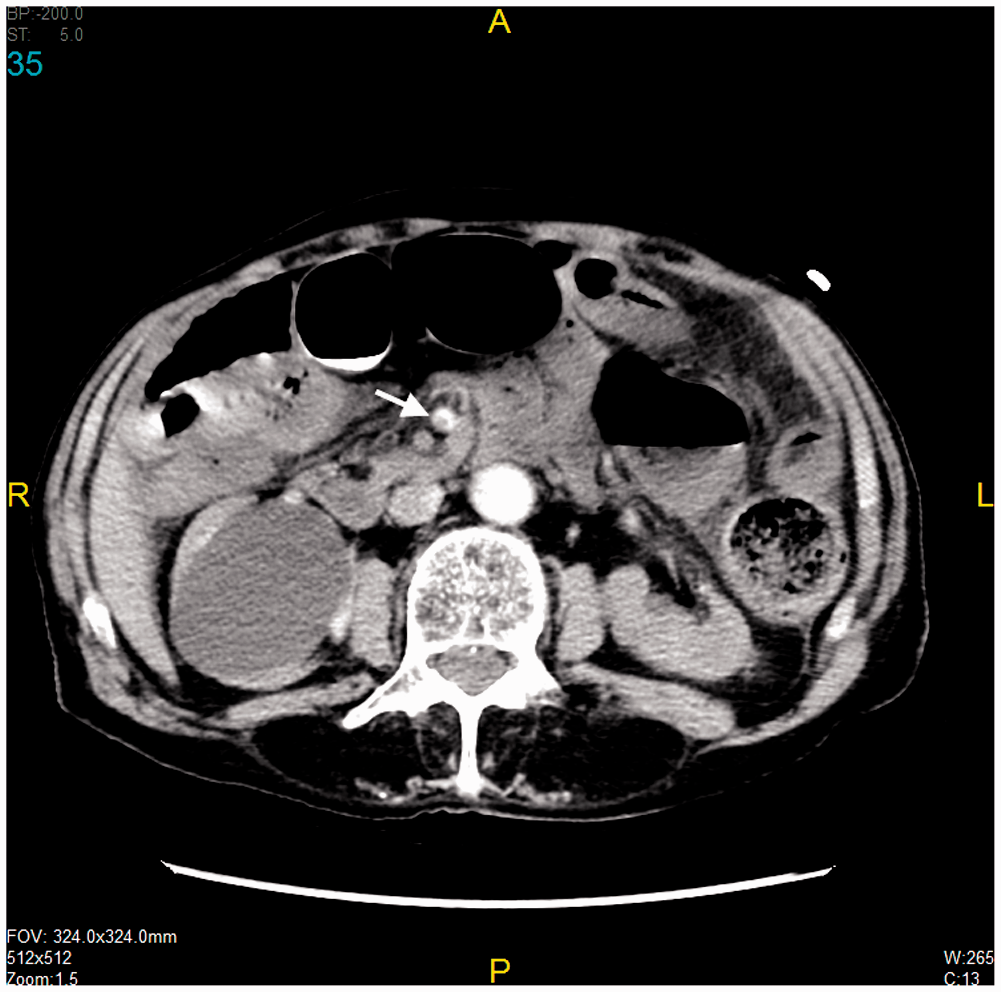
Exploratory laparotomy revealed a gangrenous segment of the distal jejunum 25 cm in
length, with discoloration and hypoperistalsis in the ileum distal to that segment.
SMA embolectomy resulted in improvement in the color and peristalsis of the ileum.
The gangrenous jejunal segment was resected, and stapled side-to-side anastomosis
was performed. Patient received unfractionated heparin postoperatively. Oral intake
was started on the fifth postoperative day, accompanied by return of normal bowel
movements. Warfarin therapy was commenced subsequently. Microscopic examination of
the resected jejunal segment confirmed the diagnosis of ischemic bowel necrosis.
Repeated CT scan after 24 h. Axial images from
portal phase still show the SBFS with decreased enhancement of the
jejunal wall (arrow).
Discussion
Acute mesenteric ischemia is a rare disease with substantial mortality. Timely diagnosis and surgery are key in limiting mortality. Multidetector CT scan (MDCT) has emerged as the tool with highest diagnostic accuracy in acute mesenteric ischemia (2), with reported sensitivity and specificity in the region of 94%, and 95%, respectively (2,3).
The SBFS was first described by Mayo-Smith in 1995 as gas bubbles mixed with particulate matter in dilated segments of small bowel (1). The particulate matter is thought to represent undigested food resulting from delayed transit (1,4–7). SBFS is found in 7.4–55.9% of CT scans of SBO (4,6–13). The sign appears mostly in the distal part of small bowel (1,4,6). When present, SBFS is indicative of slowly progressive, rather than complete abrupt, obstruction (6). It is usually located at or is most evident at the point of transition, thus facilitating the identification of transition zone in SBO (6). There is conflicting evidence regarding the prognostic significance of the SBFS. Delabrousse et al. (7), Zielinski et al. (9,11), and Deshmukh et al. (10) all found that the presence of SBFS in the CT scans of patients with SBO was significantly associated with successful non-operative management. On the other hand, Sheedy et al. (14), Geffory et al. (15), and Wang et al. (12), found that the presence of the SBFS was significantly associated with bowel ischemia complicating SBO, and therefore the need for surgical intervention.
Barrett et al. (16) reported the MDCT findings in 52 patients with mesenteric ischemia following cardiopulmonary bypass surgery. The SBFS had high specificity (94%) but low sensitivity (27%) for mesenteric ischemia in this group of patients. None of these patients had mechanical intestinal obstruction, and all had non-occlusive etiology for ischemia.
Up to our knowledge, this is the first written description of the SBFS in association with occlusive mesenteric ischemia. We believe this case is worthy of attention because the SBFS developed within a short period from the development of symptoms (less than 6 h) in absence of progressively developing mechanical obstruction. Obstruction developing over a sufficient period of time is typically required to allow for slowed intestinal transit, increased water absorption, and bacterial overgrowth to happen (4,5), leading to formation of the feces like intestinal content. In addition, the SBFS in our case was evident before any significant reduction in mural enhancement developed.
Given the short time duration from beginning of symptoms to appearance of SBFS on CT scan, and the absence of mechanical intestinal obstruction, we hypothesize that SBFS in this case might have represented sloughed ischemic mucosa accumulating in the bowel lumen rather than undigested food. This can be supported by the fact that ischemic small bowel injury occurs first at the tip of the villus and progresses downward to include the base as the ischemic episode deepens. Such changes can occur while the deeper layers of the intestinal wall are devoid of histological signs of tissue damage (17). Derikx et al. (18) found that enterocyte desquamation occurs as early as 30 min after ischemia in human jejunum. A noteworthy finding in all jejunal samples collected after exposure to ischemia-reperfusion injury in their study was the presence of a milky substance that appeared from the lumen. Histological analysis of this debris revealed sheets of enterocytes with apoptotic cells shed into the lumen of the bowel. This milky debris might have appeared as the SBFS in our case. Furthermore, the SBFS in our case was confined to the ischemic segment rather than appearing proximal to it, as would be expected in cases of mechanical (or functional) obstruction, where undigested food hold up (and subsequently the SBFS) occurs proximal to the point of obstruction (6).
In conclusion, SBFS can appear in association with occlusive AMI in absence of gradually developing mechanical obstruction. Further studies are needed to examine its utility as an accessory, possibly early, finding of mesenteric ischemia on CT scan, and to determine its significance, if any, as a prognostic indicator.
Footnotes
Patient consent
Informed consent has been obtained from the patient for the release of the above clinical information.
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.