
Abstract
Thyroid hemiagenesis is a rare form of thyroid dysgenesis characterized by an absence of half of the thyroid gland. Developmental hemi-thyroid anomalies can result from either an abnormal descent or an agenesis of one lobe of the thyroid gland. We report a case of a 40-year-old woman with history of a longstanding gradually progressive thyroid swelling without any complication. An ultrasonographic examination diagnosed the absence of the left thyroid lobe and enlargement of the right lobe, which was confirmed on a computed tomography (CT) angiogram and a radionuclide scan of the neck. A cytological examination showed nodular goiter with cystic degeneration. Right subtotal thyroidectomy was performed and histopathological examination confirmed adenomatous goiter with degenerative changes. We report the rarity of the condition and emphasize the role of a comprehensive radiological, cytological, and radionuclide algorithm for an accurate preoperative diagnosis and subsequent management.
Introduction
Thyroid hemiagenesis is a rare developmental anomaly in which one thyroid lobe fails to develop. It can result from either an abnormal descent or an agenesis of one lobe. This was first reported in 1886 by Handfield-Jones (see Tiwari et al. (1)) and is usually diagnosed following presentation with unrelated thyroid disorder like goiter and hypothyroidism (2). The true prevalence of thyroid hemiagenesis is hence not known, however it is estimated to be about 0.02–0.05% (2,3). We report a case of a hemiagenesis of the left lobe of the thyroid gland associated with multinodular goiter in right lobe with normal functional status and discuss the role of advanced imaging modalities including reconstruction computed tomography (CT) angiography in diagnosis of the condition.
Case report
A 40-year-old woman presented with longstanding gradually progressive thyroid
swelling with euthyroid status. The right thyroid lobe was enlarged, with a firm,
non-tender nodule at the lower pole but the left lobe could not be appreciated. The
biochemical thyroid profile was normal and ultrasonographic examination of the neck
revealed multiple circumscribed hypoechoic lesion in right lobe of the gland
suggestive of multinodular goiter. However the left lobe could not be visualized
(Fig. 1). A suggestion
of left thyroid lobe agenesis was entertained and a CT angiography was ordered to
visualize the thyroid arteries. The multi-planner reconstructions and maximum
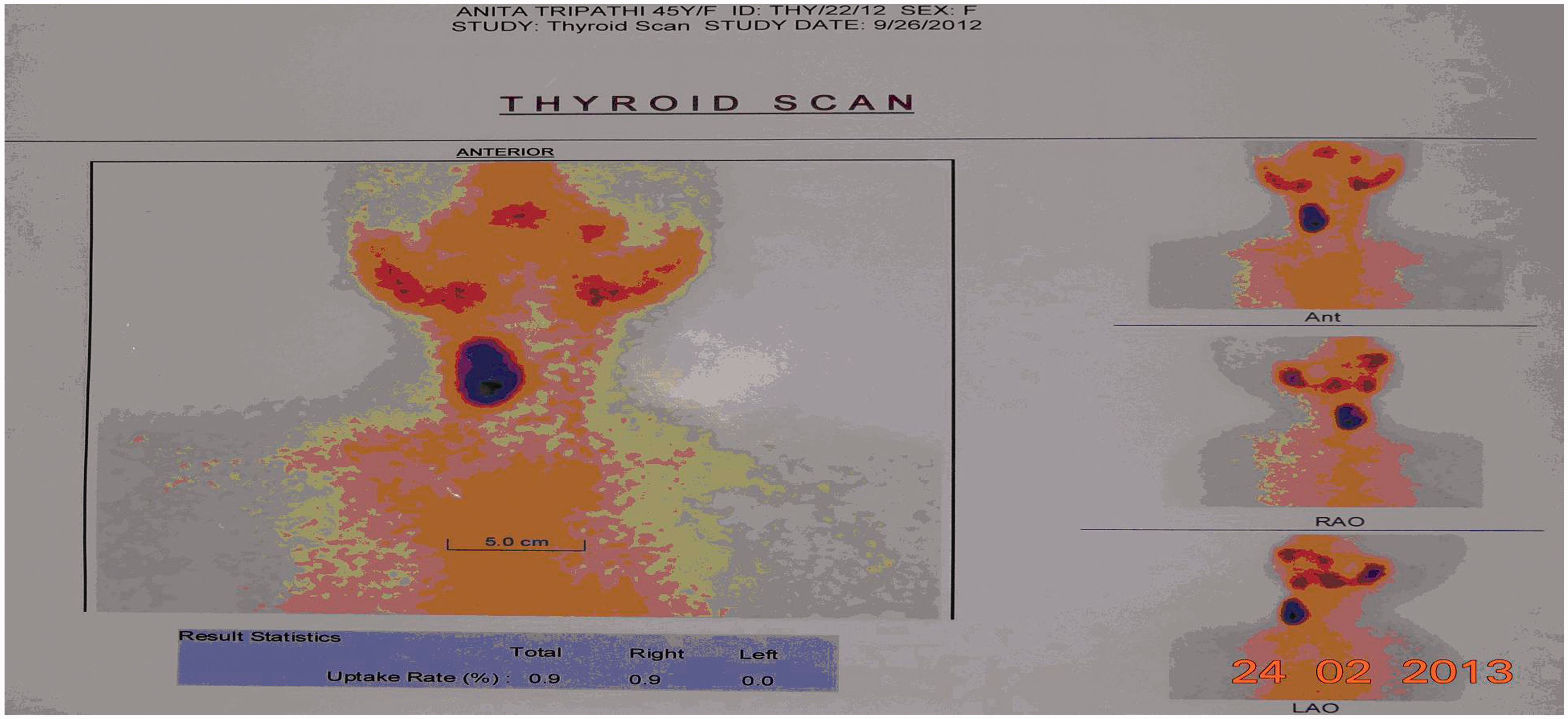
intensity projection images revealed aplasia of left inferior thyroid artery (Fig. 2a and b). A thyroid scintigram with
Tc-99 m partechnetate revealed absence of left lobe and isthmus, and a nodule in
right thyroid lobe, which was functional (“hot nodule”) (Fig. 3). A fine needle cytological
examination of the right lobe nodule revealed nodular goiter with cystic
degeneration. A right subtotal thyroidectomy was performed to prevent the
postoperative hypothyroidism and the agenesis of the left lobe and isthmus and the
left inferior thyroid artery was confirmed intraoperatively. Histopathological
examination of the specimen confirmed adenomatous goiter with degenerative changes.
The patient was discharged following an uneventful postoperative course and was
normal at 6-month follow-up. High frequency ultrasonography revealed
empty left thyroid fossa. (a) Oblique coronal (35°) thick MIP reconstruction
of CT angiogram, showing major neck vessels and their branches. On the
right side, the thyrocervical trunk shows origin of inferior thyroid
artery (straight arrow) ascending upwards. On the left side, no
comparable ascending branch could be noted from the thyrocervical trunk
(hollow arrow), which was dividing to end as intercostals and muscular
arteries. (b) Axial oblique (20°) thick MIP reconstruction of helical
non-contrast CT scan neck, showing an empty left thyroid fossa (hollow
arrow). Note the normal hyper-attenuating thyroid tissue in the right
thyroid fossa (straight arrow). Thyroid scintigraphy revealed absence of left lobe
with isthmus.

Discussion
Thyroid hemiagenesis has been reported as a rare developmental abnormality detected at autopsy or incidentally during surgery (4). Medical literature indicates an estimated prevalence rate between 1/1900 and 1/2675 population (5), which is similar to that observed for congenital hypothyroidism because of agenesis or ectopia.
At 16–17 days of gestation the thyroid gland develops as a tubular invagination of the primitive pharyngeal endoderm dorsal to aortic sac between first and second pharyngeal pouches. It then expands ventrally along the thyroglossal duct line and a spherical thyroid gland primordium continues to proliferate under the influence of thyroid progenitors. Its lumen obliterates and it becomes filled with thyroid rudiment cells. The thyroid gland primordium subsequently begins to expand laterally and leads to the formation of the final bilobed structure (6).
The initiation factor and temporal point for thyroid hemiagenesis are as yet unclear. The absence of compensatory hypertrophy of the contralateral normal lobe, in most of the patients, suggests a defect in lobulation to be the initiation point rather than an abnormal descent. A high incidence of the condition in monozygotic twins or with other thyroid malformations within the family may indicate a possible role of genetic factors (7–9). Although several genes have been implicated in thyroid morphogenesis and descent (like TTF-1, TTF-2, and PAX-8 for thyroid ectopia) (10), no such genetic analysis has been done in cases of thyroid agenesis. The genetic analysis of the present case could not be done due to non-availability of the facility.
Most patients with thyroid hemiagenesis present with unrelated thyroid symptoms. It is interesting to note that most cases have an agenesis of the left lobe (80% of cases) followed by the isthmus (44–50% of cases) (2). The prevalence is higher in women (3:1, as was also in the present case), which may indicate a possible gender association (2). Hyperthyroidism has been reported to be the most common clinical presentation leading to an incidental diagnosis of the hemiagenesis (11–13). Our case presented with multi-nodular goiter which has be reported as the second most common association.
The diagnosis of thyroid hemiagenesis can be suggested by a thyroid scintigram which shows accumulation of tracer on one side within the thyroid region. However, caution needs to be exercised for such finding, as there are several conditions, which may mimic hemiagenesis such as autonomous functioning nodule with suppressed normal thyroid tissue, infiltrative disease such as amyloidosis, primary and secondary neoplasm, and unilateral inflammation. Correlation with an initial high frequency ultrasonographic examination, which is widely available, is advisable and which was also done in the present case. Demonstration of the absence of ipsilateral thyroid arteries by CT further adds to the confidence level. The absence of left thyroid arteries was observed on CT angiography and was confirmed intraoperatively. This finding can be explained by the general embryologic dictum of failure of development of vasculature in case of erroneous organogenesis.
In conclusion, hemiagenesis is rare event in thyroid embryogenesis. It remains unsuspected until a disease of the existing lobe brings it under clinical attention. Radionuclide scan and CT angiography are investigations of choice for accurate diagnosis which is important to prevent inadvertent thyroid ablation during surgery.
Footnotes
Conflict of interest
None declared.