
Abstract
Background
Actinomycosis is a rare suppurative disease that may mimic other inflammatory conditions on imaging. Its invasive nature may lead to mass formation and atypical presentation thus making accurate diagnosis quite difficult.
Purpose
To describe the different aspects of abdominopelvic actinomycosis on cross-sectional imaging and indicate discriminative findings from other inflammatory or neoplastic diseases.
Material and Methods
In our study we analyzed 18 patients (15 women, 3 men; age range, 25–75 years; mean age, 50 years) with pathologically proved abdominopelvic actinomycosis. Contrast-enhanced abdominal computed tomography (CT) had been performed in all patients. Eleven patients had a history of using intrauterine contraceptive devices. Bowel site, wall thickness and enhancement degree, inflammatory infiltration, and features of peritoneal or pelvic mass were evaluated at CT.
Results
The sigmoid colon was most commonly involved. Most patients showed concentric bowel wall-thickening, enhancing homogenously and inflammatory infiltration of pericolonic fat was mostly diffuse. In 11 patients, one or more pelvic abscesses were revealed, while a peritoneal or pelvic mass adjacent to the involved bowel segment was seen in three cases. Infiltration into the abdominal wall was seen in three cases while in one case there was thoracic dissemination.
Conclusion
Actinomycosis is related not only to long-term use of intrauterine contraceptive devices and should be included in the differential diagnosis when cross-sectional imaging studies show concentric bowel wall-thickening, intense contrast enhancement, regional pelvic or peritoneal masses, and extensive inflammatory fat infiltration with abscess formation.
Introduction
Actinomycosis is a rare suppurative disease characterized by progressive, chronic, granulomatous infection caused by an anaerobic Gram-positive bacterium, Actinomyces Israelii (1). These organisms are not regarded as virulent human pathogens and are best considered as opportunistic pathogens, as they are normally present in healthy individuals, especially in the oral cavity and tonsillar crypts and in the colon. Abdominopelvic actinomycosis can manifest as fistula, sinus, inflammatory pseudotumor, or abscess formation. Its capacity to invade surrounding tissues and to form masses might mimic other diseases often leading to misdiagnosis (2). The aggressive nature of the infiltration is one of the most important radiologic characteristics of this infection. Computed tomography (CT) has been useful for determining the anatomic location and extent of the disease and for monitoring the effectiveness of treatment. The mainstay of treatment of the disease is the administration of high doses of penicillin, often leading to a favorable outcome (3). Therefore, early diagnosis minimizes the morbidity of disease and can avoid unnecessary surgery. The aim of this study was to describe the different aspects of abdominopelvic actinomycosis on cross-sectional imaging and indicate discriminative findings from other inflammatory or neoplastic diseases.
Material and Methods
The radiology, pathology, and infectious diseases databases of two hospitals, one university and one general (LUMC NL and Konstantopouleio Hospital in Athens, Greece), were structurally searched for actinomycosis. Between November 2001 and February 2011, 18 patients (15 women, 3 men; age range, 25–75 years) with abdominopelvic actinomycosis were identified. Contrast-enhanced abdominal CT had been performed in all patients, on 16 - and 64-slice multidetector scanners. The clinical data including age, symptom, mass size, presence of intrauterine device (IUD), and preoperative diagnosis were retrospectively analyzed. Bowel site, wall thickness and enhancement degree, inflammatory infiltration, and features of peritoneal or pelvic mass, were evaluated at CT by two readers in each center.
Results
In our databases we found 18 patients, 15 women and three men. The clinical symptoms and signs in these patients included abdominal pain (n = 18), fever (n = 11), changed bowel habits (n = 3) and palpable mass (n = 2). The duration of these symptoms and signs ranged from 5 days to 8 months. Laboratory results revealed leukocytosis in 16 patients (12.5–30.5/mm3) and inflammatory markers (BSR and CRP) were elevated. Eleven female patients had a history of using IUDs for an average of 7 years (range, 2–14 years). Six women carried hormone-containing IUDs and five women had inert IUDs. At the time of the symptoms nine women had the IUD in place, while in the other two it was removed 2 and 4 months before.
In the other seven cases (out of 18) there was a history of appendicitis (one male patient), diverticulitis (one female patient), inflammatory bowel disease (two male patients), and open or laparoscopic surgery (three female patients). No patients were immunocompromised.
CT findings confirmed the infiltrative nature of the disease, which tended to invade
across tissue planes and boundaries. In 11 patients an inflammatory mass involving
the uterus and ovaries was revealed (Fig. 1). The main differential diagnoses
proposed for all the patients were the following: tubo-ovarian abscess
(n = 6), Crohn’s disease (n = 3), complicated
diverticulitis (n = 2), colon cancer (n = 2),
ovarian cancer (n = 2), prostatic cancer (n = 1),
endometriosis (n = 1), and uterine cancer (n = 1).
(a) Contrast-enhanced CT axial image and (b)
contrast-enhanced CT coronal image: many “cystic” lesions consistent
with abscesses are seen in the pelvic area, in a woman wearing
IUD.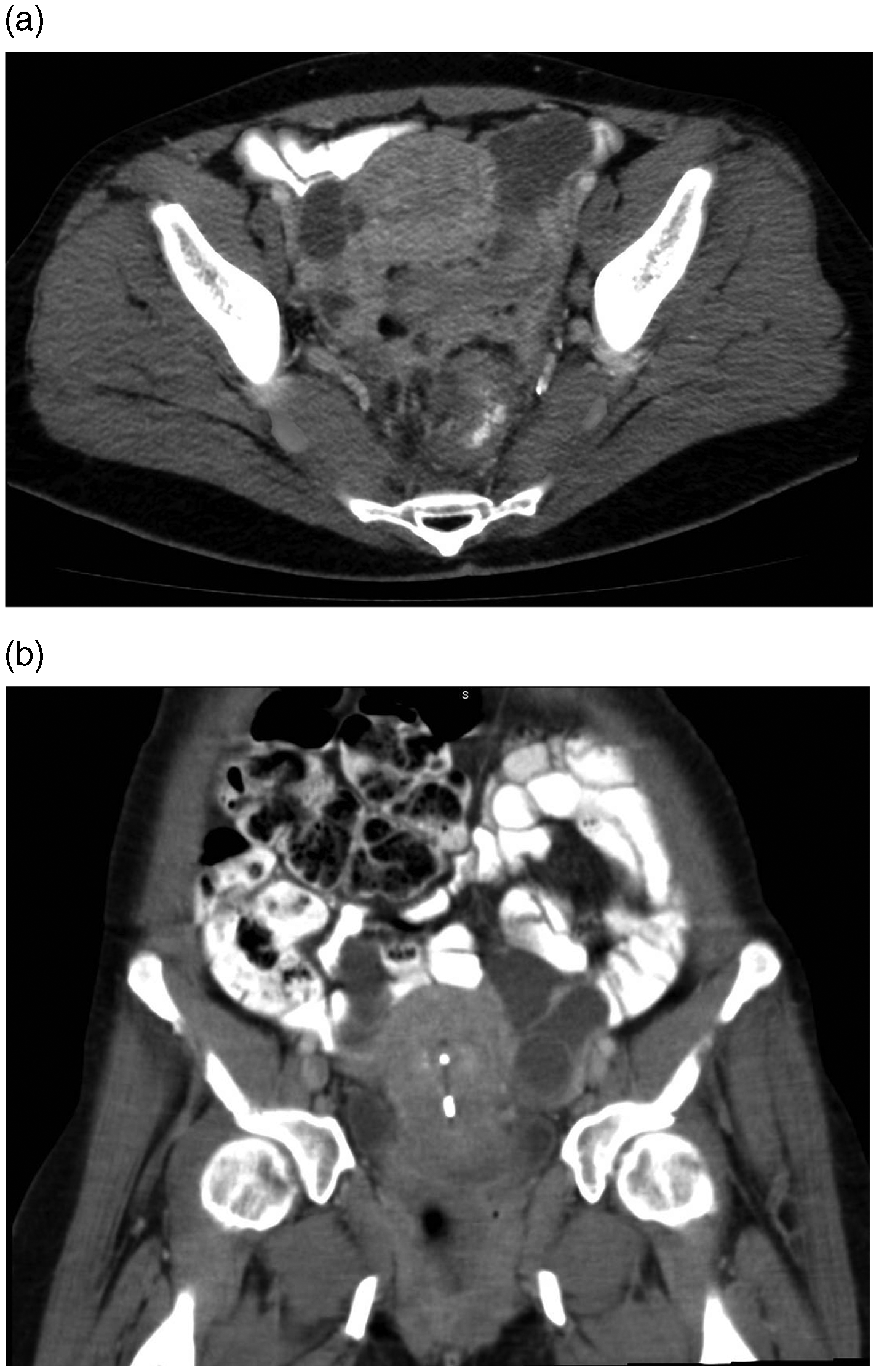
The most commonly involved sites in the gastrointestinal tract were the sigmoid colon
in five patients, the appendix and the distal ileum in three cases (Fig. 2). Most patients showed
concentric bowel wall-thickening (0.5–1.5 cm) while the length of the involved bowel
was 5–15 cm (Fig. 3). The
thickened bowel enhanced homogeneously in most patients and perirectal, pericolic,
or perienteric infiltration was observed in all patients (Fig. 4). An inflammatory mass
involving the right adnexa and the sigmoid region is seen on this CT
image. There is also extensive inflammatory infiltration of the pelvic
fat while some loops of small bowel are also
involved. (a, b) Many collections and abscesses are found in
the pelvis and there is also inflammatory involvement of the fat and
mild small bowel wall-thickening very well seen on these CT
images. (a, b) Abdominal CT images: bowel compression is
evident, thickening of the sigmoid colonic wall and an amount of free
fluid in the pelvis. There is also extensive inflammatory infiltration
of the left lateral abdominal wall.


In 17 patients, a peritoneal or pelvic mass was seen adjacent to the involved bowel. It appeared to be predominantly cystic and heterogeneously enhanced. In only one case, the mass contained solid components showing marked contrast enhancement. The diameter of the masses was 1–5 cm and the margins were irregular and indistinct. Small bowel dilatation was noticed in one case.
Infiltration into the abdominal wall was seen in three cases with a large abscess
formation in one patient (Fig.
5). Lymphadenopathy was noted in five patients but it was minimal and
involved the para-aortic, mesenteric, and pelvic lymph nodes. CT
image shows a very large abscess of the left lateral abdominal
wall.
In two cases abscesses were found in the liver and in one case there was an abscess in the prostatic gland. Finally in one case there was thoracic dissemination.
Discussion
Actinomycosis was first described by Israel in 1879. It is a rare infectious disease caused by Actinomyces Israelii, a Gram-positive anaerobic saprophyte bacterium. The organisms are indigenous in the oral cavity, gastrointestinal tract, and genital track. The destruction of the mucosal barrier by trauma related to endoscopic procedures, operations, or chronic inflammatory disease, is recognized as predisposing factors (1,2,4).
The three main clinical forms of this disease are cervicofacial (50–65%), thoracic (15%), and abdominopelvic (20%). Pelvic actinomycosis has recently become more prevalent and it is associated almost exclusively with women who use IUDs (5–9) which is confirmed in our study as we found that 11 of our 15 female patients used an IUD.
Clinical findings are variable, depending on the involved organ and the duration of the disease (1,7). Common symptoms and signs include abdominal pain with or without palpable mass, body weight loss, fever, vaginal discharge, constipation, or diarrhea. In laboratory analyses the dominating sign are leukocytosis, positive inflammation markers, and anemia as we confirmed in our results.
High dose intravenous penicillin injection is the treatment of choice. Tetracycline, clindamycin, and erythromycin can alternatively be used for patients allergic to penicillin. Therefore, early diagnosis is important to minimize the morbidity of this disease and avoid unnecessary surgery (3,6). In our study 12 of 18 patients responded to conservative therapy and only six patients were treated surgically.
Abdominopelvic actinomycosis may be the most indolent and latent of all the clinical forms of actinomycosis and diagnosis may be delayed for months after the inciting event. As we confirmed in our study actinomycosis may involve the abdominal wall, segments of the colon, uterus, ovaries, bladder, liver, gallbladder, and pancreas (5,10). The portions of the gastrointestinal tract commonly involved are sigmoid colon, rectum, cecum, appendix, distal ileum, and ascending colon (5,11). In our study the most commonly involved sites of the gastrointestinal tract were the sigmoid colon, appendix, and distal ileum. The common occurrence at the rectosigmoid colon contributes to the high frequency of pelvic involvement.
One of the important radiologic characteristics of abdominopelvic actinomycosis is the aggressive nature of the infiltration. This disease’s infiltrative nature, and its tendency to invade normal anatomic barriers, was confirmed in most of our patients. Such a pattern may be the result of proteolytic enzymes produced by Actinomyces. This results in extensive inflammatory fat infiltration with abscesses formation in the abdominal wall (12,13).
The organism in actinomycosis usually does not spread via lymphatic or hematogenous routes and regional lymphadenopathy is not a common finding. If lymphadenopathy is present, it is usually minimal as in five of our cases (4,7). It should be noted that despite the extensive inflammatory infiltration in the perirectal, pericolonic, or perienteric spaces, the disease process does not appear to spread into the whole peritoneal cavity and ascites is absent or minimal.
The radiology findings in a barium study include mural invasion with structure formation, mass effect with tapered narrowing of the lumen, and thickened mucosal folds. Such radiology findings are not specific for abdominopelvic actinomycosis. The disadvantage of barium studies is that it does not examine the abdominal wall and in general it is no longer considered a mandatory study in these cases.
On the other hand, the use of CT in abdominopelvic actinomycosis is essential for the diagnosis and for establishing the location and the extent of the disease. In our study and in other studies from the literature the most common findings are concentric bowel wall-thickening, enhancing homogeneously, and forming fistula (9,10,14–18). These radiologic findings are non-specific and are quite similar to those in Crohn’s disease, intestinal tuberculosis, or sometimes excavated malignant tumor. CT-guided fine needle aspiration may be not only diagnostic in equivocal cases but also therapeutic in cases of large abscesses.
The most important CT feature for the correct diagnosis in our study was a large mass adjacent to the involved bowel. These masses appeared to be predominantly cystic or solid (pseudotumor) with contrast enhancement in the walls or the solid components of the masses (5,8,19). Most cases of rectosigmoid colon involvement show predominantly cystic masses, whereas cases involving the transverse colon or appendix demonstrate predominantly or purely solid masses. These findings reflect the histologic features of actinomycosis: central suppurative necrosis surrounded by granulation tissue and intense fibrosis.
In conclusion, actinomycosis is a rare disease that is not exclusively related to long-term use of IUDs. Actinomycosis should be included in the differential diagnosis when cross-sectional imaging studies show concentric bowel wall-thickening, intense contrast enhancement, regional pelvic or peritoneal masses, and extensive inflammatory fat infiltration with abscesses formation, especially in the absence of lymphadenopathy.