
Abstract
Aggressive fibromatosis arising from the retroperitoneum is extremely rare. It may occur in association with previous trauma, abdominal surgery, drugs, Gardner’s syndrome, or familial adenomatous polyposis. We report a case of retroperitoneal fibromatosis presenting as a presacral mass with an infiltrating nature, relatively intense enhancement on enhanced computed tomography scanning, and low-signal intensity on T2-weighted magnetic resonance imaging in a patient with no significant medical or surgical history.
Introduction
Aggressive fibromatosis or desmoid tumor is an infiltrating fibroblastic proliferation arising from the musculo-aponeurotic structures (1,2). It either arises in musculoskeletal sites, including the paravertebral musculature and the anterior abdominal wall, particularly in relation to surgical scars, or within the abdomen, involving the mesentery, the retroperitoneum, or pelvis (1–3). Intraabdominal fibromatosis are rare but those arising from the retroperitoneum are even rarer. Several etiologies have been proposed, which include trauma, abdominal surgery, irradiation, drugs, genitourinary infection, Gardner’s syndrome or familial adenomatous polyposis (FAP). Therefore, the diagnosis of intra-abdominal fibromatosis should be strongly considered when an abdominal mass is detected in patients with a history of previous abdominal surgery or hereditary diseases (4).
We report a case of retroperitoneal fibromatosis presenting as a presacral mass in a young female patient with no significant medical or surgical history and describe its imaging findings.
Case report
A 23-year-old woman presented with dull periumbilical pain of 2 months’ duration. The
patient denied any history of constitutional symptoms including weight loss, fever,
diarrhea, or vomiting. She had no history of previous abdominal surgery or any other
noteworthy pathology. On physical examination, the periumbilical area was tender
without guarding or rebound tenderness, and a firm, fixed mass was palpable. All
laboratory tests were within normal limits. For evaluation of the palpable mass,
pelvic computed tomography (CT) scanning was performed. The pelvic CT scan revealed
a heterogeneously enhancing soft tissue mass (7.0 × 5.0 × 9.0 cm) that contained a
necrotic portion in front of the abdominal aortic bifurcation. There was no evidence
of calcification. The mass abutted the abdominal aorta and surrounded and compressed
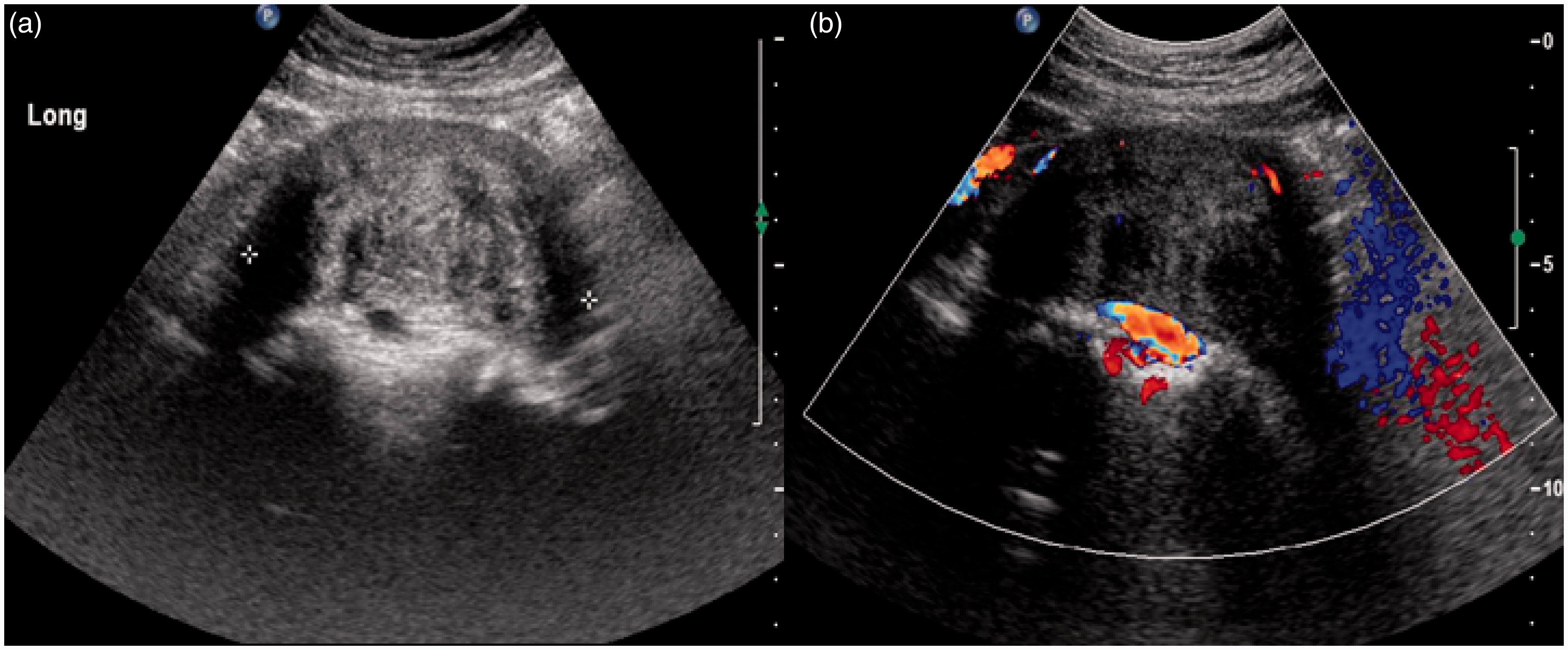
the inferior vena cava and right common iliac artery (Fig. 1). Additional abdominal ultrasonography
(US) demonstrated a presacral soft-tissue mass abutting with sacrum. There was no
evidence of increased intralesional vascularity (Fig. 2). To further characterize the mass,
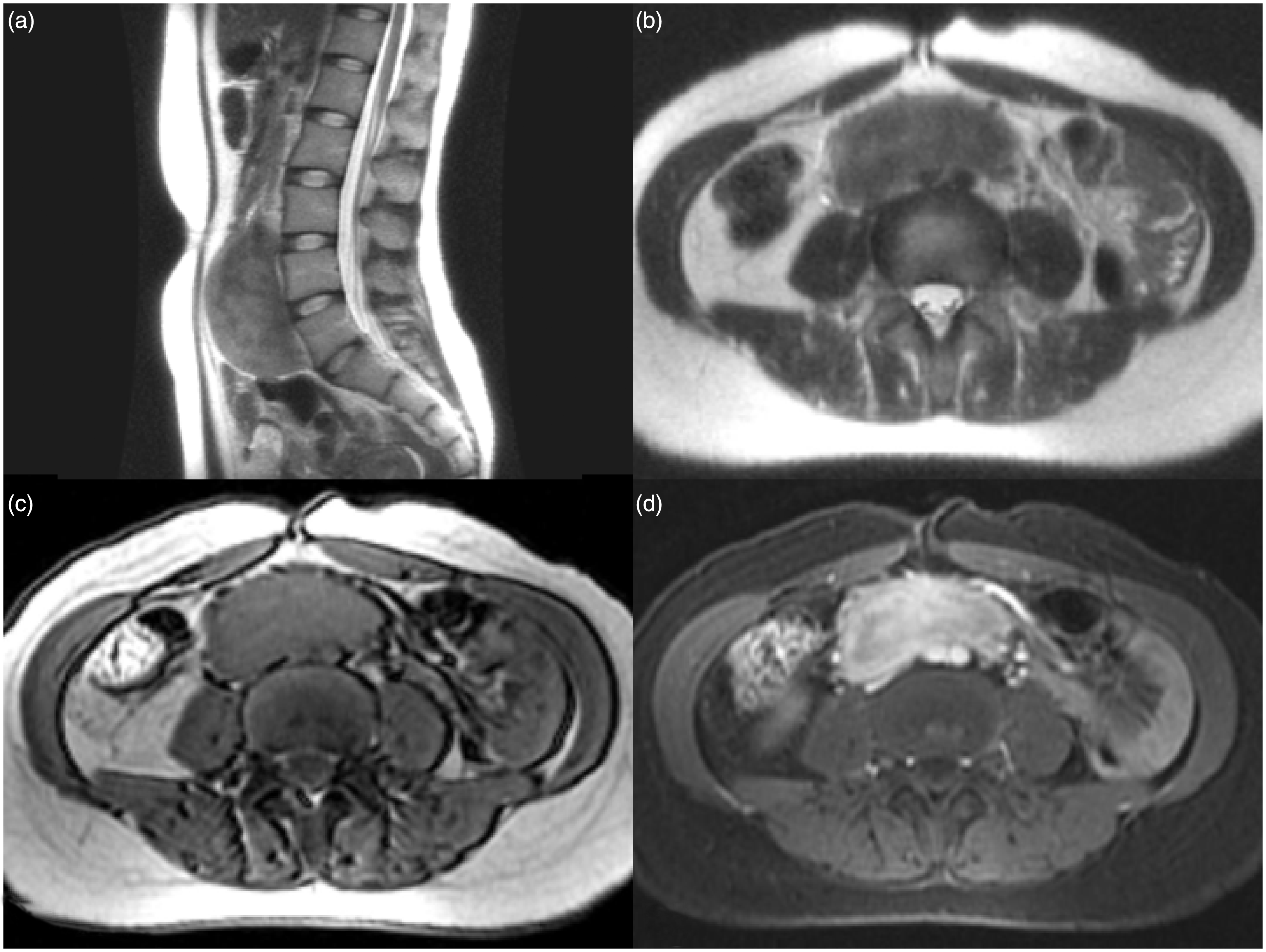
magnetic resonance imaging (MRI) was performed. On MRI, the mass showed iso-signal
intensity (SI) to muscle on T1-weighted (T1W) imaging, relatively low SI on
T2-weighted (T2W) imaging, and relatively homogeneous, strong enhancement on
fat-saturated contrast-enhanced T1-weighted (FS CE-T1W) imaging (Fig. 3). The preoperative
radiologic impression was neurogenic tumor or smooth-muscle-origin mass. In the
surgical field, the mass was hard and infiltrated to the aorta, right common iliac
artery, and inferior vena cava. A large, retroperitoneal mass measuring
9.0 × 5.0 × 9.5 cm, was removed, and resection and repair of the greater vessels was
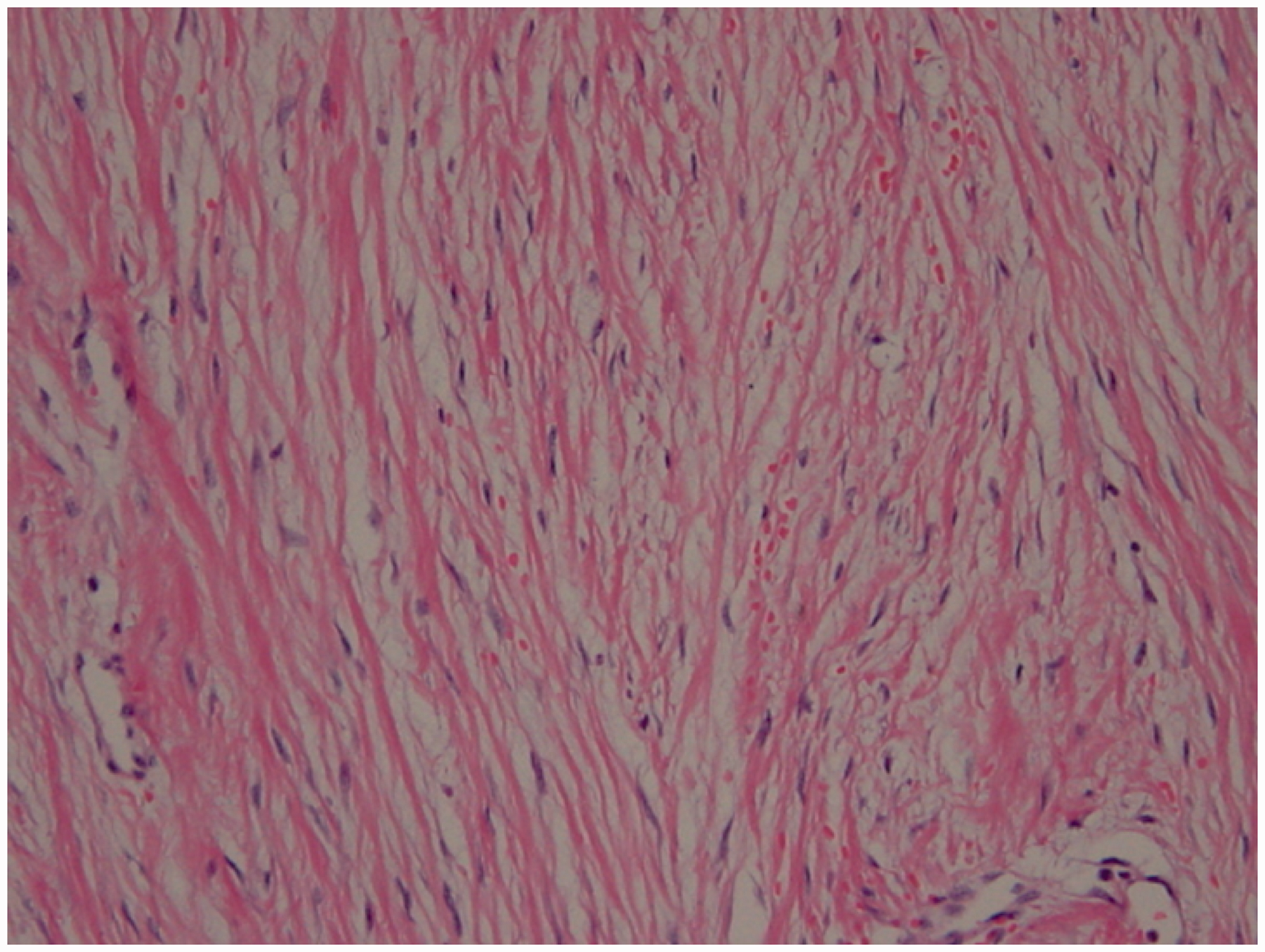
performed due to mass infiltration of greater vessels. On microscopic examination,
the tumor showed spindle cells, intervening collagenous stroma, and relatively rich
vascularity without cytologic atypia or mitoses. Special staining of the tumor cells
showed a positive reaction for vimentin and a negative reaction for smooth muscle
actin (Fig. 4). Finally, the
tumor was confirmed as fibromatosis on the basis of the pathology test. Axial CT scan before and after contrast
enhancement (a, b), shows a large heterogeneously enhancing
retroperitoneal soft-tissue mass. This mass compresses the inferior vena
cava and encases the right common iliac artery. The longitudinal trans-abdominal US shows a
slightly heterogeneous hypoechoic solid mass abutting the sacrum and
compressing the great vessels (a). There is no evidence of increased
intralesional vascularity (b). MRI reveals a large retroperitoneal soft-tissue
mass in the presacral area. The mass shows a relatively low SI on T2W
imaging (a, b), iso-SI with muscle on T1W imaging (c), and relatively
homogeneous strong enhancement on FS CE-T1W imaging (d). The MR images
indicate compression of the inferior vena cava and encasement of the
right common iliac artery. Photomicrograph of the histologic specimen
(Hematoxylic-eosin stain, original magnification 200×), reveals abnormal
proliferation of fibroblasts, indicating a positive reaction for
Vimentin and a negative reaction for smooth muscle Actin, S-100 protein,
and C-kit.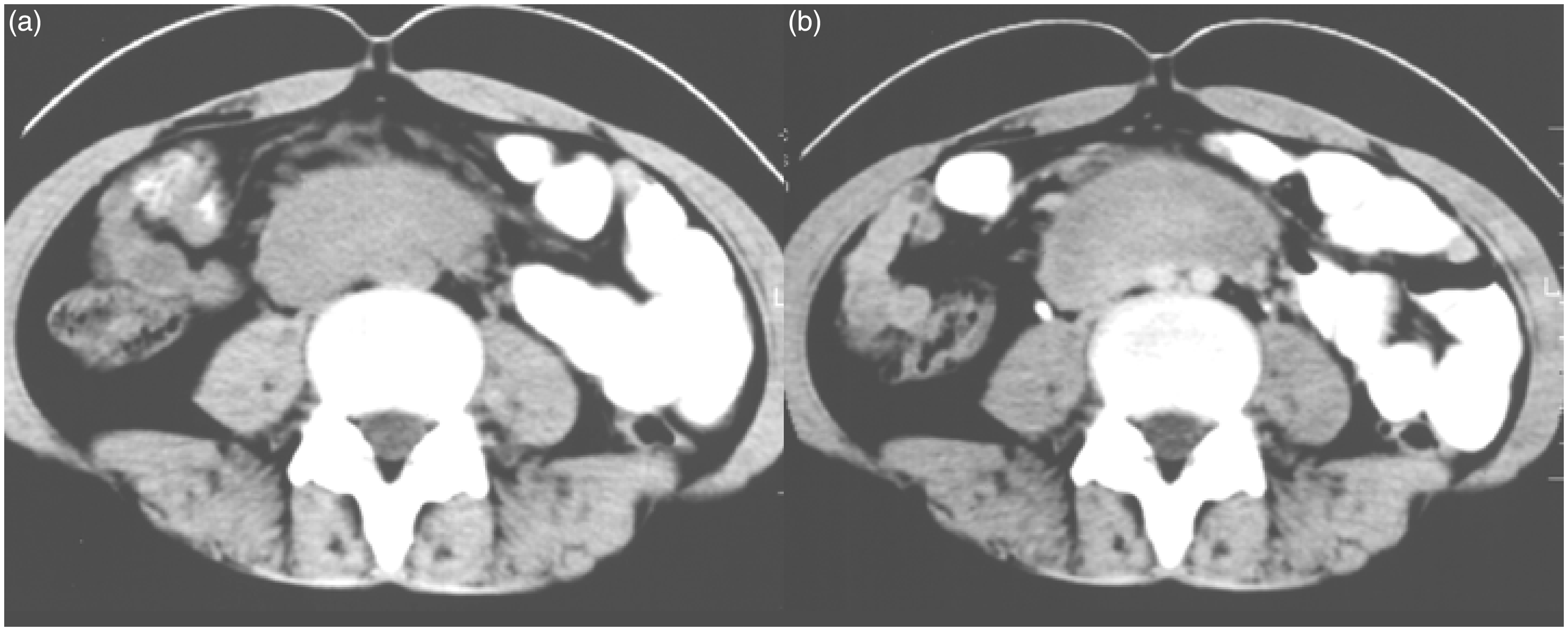
Discussion
Aggressive fibromatosis has been defined as an infiltrating fibroblastic proliferation without evidence of inflammation or definite neoplasia (1,4). Generally, these tumors occur more frequently in women, particularly in women of childbearing age. They may occur at any age but are seen most commonly in the third and fourth decades (5). The cause of this disease is not clear, but several etiologies have been proposed. In our case, the patient did not have any history of trauma, drugs, surgery, or hereditary disease. Our case therefore exhibits the sporadic or primary form of fibromatosis. The primary form is extremely rare and presents fibroblastic proliferation with no connection to the patient’s medical or surgical history (6). The diagnosis is difficult to establish preoperatively, especially in the case of a patient with no history of abdominal surgery or injury, drug medication, Gardner’s syndrome, or FAP, such as in our case.
Fibromatosis either arises in musculoskeletal sites, including the paravertebral musculature and the anterior abdominal wall, particularly in relation to surgical scars, or within the abdomen involving the mesentery, the retroperitoneum or pelvis (1–3). Fibromatosis arising from the retroperitoneum are extremely rare and most of the data in the literature are from isolated case reports. In a large study of 189 cases of fibromatoses over 30 years, only eight (4%) were located in either the retroperitoneum or the mesentery (7). In another study of 166 desmoid tumors complicating FAP, 83 tumors (50%) were intra-abdominal but only one (0.6%) arose from the retroperitoneum (8).
The clinical presentations of fibromatosis vary depending on the size of the tumor and the surrounding involved anatomical structures. These tumors tend to invade or surround muscles, tendons, nerves, vessels, the ureter, and bowel as a result of their infiltrating nature. Therefore, ureter or small bowel obstructions occur frequently in the presence of these tumors (1). In our case, the inferior vena cava, aorta, and right common iliac artery were invaded. However, there was no involvement of the ureter or bowel perhaps due to the midline location of the tumor which tends to be locally invasive (2,9,10). Fibromatosis often recurs after resection and the reported recurrence rate is in the range of 39–79% (2). Therefore, these tumors impose significant morbidity on patients who require a larger subsequent re-excision (5). Unlike the fibrosarcoma, fibromatosis exhibit normal mitosis and does not metastasize, but there is no correlation between its clinical behavior and its histologic appearance.
The radiologic appearance of fibromatosis depends on the relative amounts of fibroblast proliferation, fibrosis, collagen content, and the tumor vascularity (11,12). On US, this tumor has a variable echogenicity with a smooth, well-defined margin. On contrast-enhanced CT scans, fibromatosis generally has high attenuation (relative to muscle) and has either an ill- or well-defined margin. On MRI, this tumor has low or iso-SI relative to muscle on T1W images and variable SI on T2W images. The difference in the SI of T2W images appears to be determined by cellularity rather than collagen content (12). In our case, the tumor showed iso-SI to muscle on T1W images, low SI on T2W images, and strong enhancement on FS CE-T1W images. In a previous report (11), the low SI on T1W and T2W images might have been characteristic for aggressive fibromatosis and therefore significant enhancement might have been expected as these lesions are frequently hypervascular on the previous arteriography and on contrast-enhanced CT studies.
In conclusion, in our patient, retroperitoneal fibromatosis appeared as a presacral mass showing infiltrating nature, i.e. vascular encasement and invasion, low SI on T2W imaging, and relatively strong enhancement on FS CE-T1W imaging. This diagnosis is difficult to establish preoperatively, especially in patients without a significant medical or surgical history. Nevertheless, it is preferable to include aggressive fibromatosis in the differential diagnosis, when the presacral soft-tissue mass has an infiltrating nature, low SI on T2W imaging, and significant enhancement on CE-T1W imaging.