
Abstract
To date, no ideal endovascular strategy has been established for traumatic arterial occlusion. Here, we report the outcomes of a combination of endovascular recanalization techniques applied in two patients with high risk of leg amputation. A 33-year-old man with popliteal artery occlusion due to blunt trauma was treated by balloon angioplasty with long inflation time and aspiration thrombectomy. A 74-year-old woman with popliteal artery occlusion after total knee replacement was treated by aspiration thrombectomy and stent placement. In both cases, we achieved satisfactory recanalization, and peripheral ischemia was absent even 1 year later.
Keywords
Introduction
Blunt and iatrogenic vascular injuries of the extremities are uncommon, but are associated with a high rate of limb loss (1–5). Although endovascular management is gaining importance (2), an ideal endovascular strategy has not yet been established for such injuries. Here, we present two cases of traumatic popliteal artery occlusion with limb-threatening ischemia that were managed by a combination of balloon angioplasty, aspiration thrombectomy, and stent placement.
Case report
Patient 1
A 33-year-old man injured in a motorcycle accident had sustained compound open
fractures of the left tibia and fibula with remarkable backward dislocation of
the bone fragments (Fig.
1a). Distal pulses were not detected after external fixation of the
below-the-knee fractures, so emergency angiography was conducted to identify
arterial injury. A left lower extremity angiogram showed complete occlusion from
the popliteal artery to the tibioperoneal trunk and the origin of the anterior
tibial artery (Fig. 1b).
Because the occluded portion was at the same level as the dislocation site, we
deduced that intimal injury, and not a thrombus, was the primary cause of the
occlusion. The patient had large skin defects and deep muscular lacerations,
which we diagnosed as contaminated wounds. Surgical repair such as replacement
of the artery with venous or synthetic grafts was considered to have a high risk
of infection; therefore, endovascular recanalization was attempted. A 4-French
sheath (Medikit, Tokyo, Japan) was inserted into the left common femoral artery
via the antegrade approach. A 0.035-inch guidewire (Radifocus; Terumo, Tokyo,
Japan) was passed through the true lumen of the occluded portion and exchanged
with a 0.018-inch guidewire (Platinum Plus; Boston Scientific, Natick, MA, USA).
The lack of extravasation of the contrast medium and disruption of the vessel
wall suggested the absence of transection or laceration, so endovascular
recanalization was continued. Heparin was administered intravenously (5000-U
bolus, 1000 U/h) and a balloon catheter system (SLALOM; Cordis, Bridgewater, NJ,
USA) was introduced co-axially. Then, stepwise inflation with three balloon
catheters of 3-, 4-, and 5-mm diameters and 4-cm length was performed 10 times
for 3 min (Fig. 1c).
During the procedure, we observed gradual joining of the intimal flap to
arterial wall and sufficient peripheral blood flow through the repaired true
lumen (Fig. 1d). A 33-year-old man with popliteal artery
occlusion due to blunt trauma (Patient 1). (a) Radiograph of the
left knee showing compound fractures of the tibia and fibula with
remarkable backward dislocation. (b) Left lower extremity angiogram
showing complete occlusion from the popliteal artery to the
tibioperoneal trunk and origin of the anterior tibial artery. (c)
Stepwise balloon angioplasty with long inflation time. (d)
Recanalization by joining of the intimal flap to arterial wall. (e)
Left lower extremity angiogram showing re-occlusion of the popliteal
artery caused by formation of a thrombus adhering to the intimal
flap (arrow). (f) Restoration of sufficient blood flow after
aspiration thrombectomy.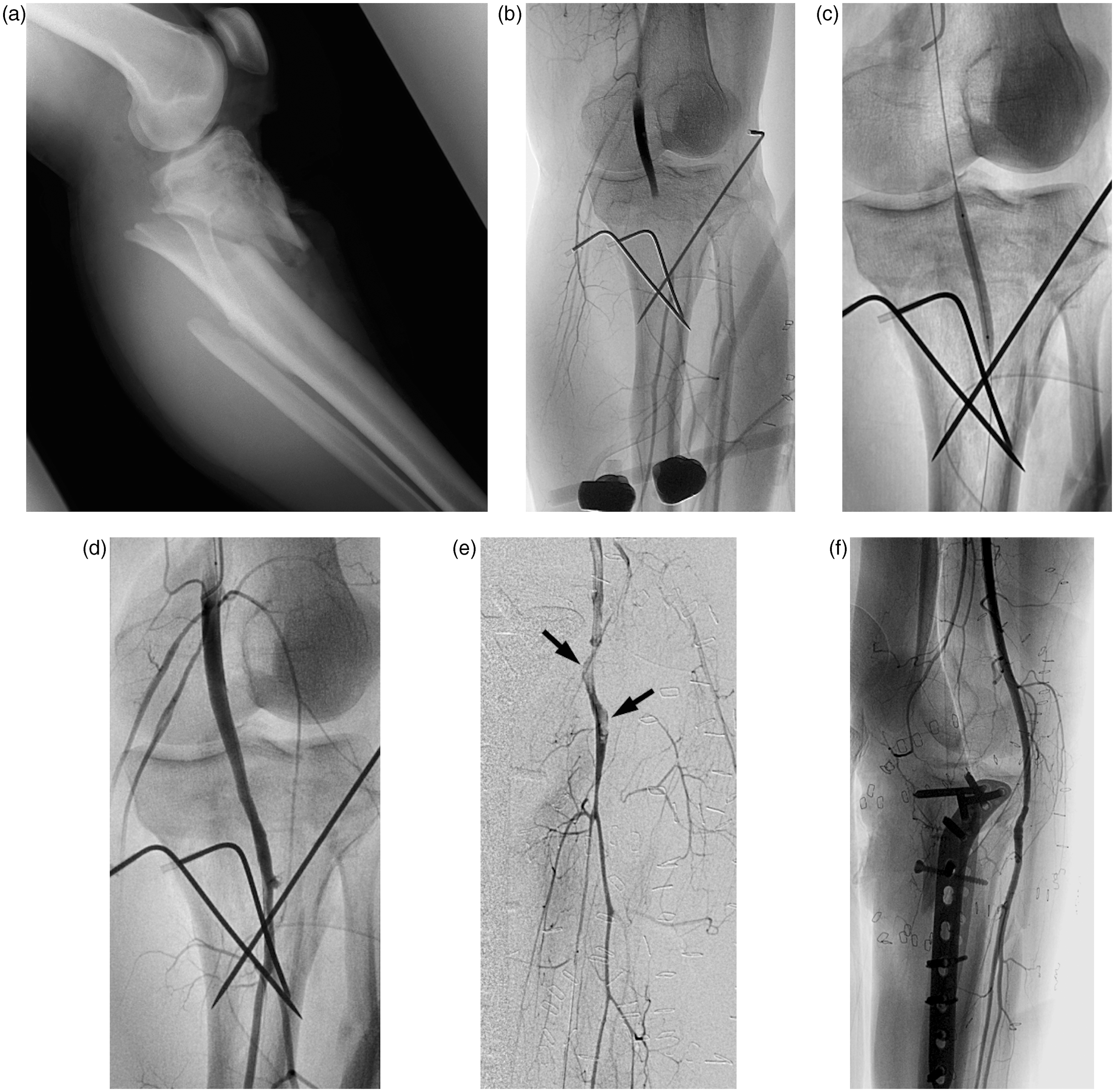
Satisfactory peripheral blood flow was maintained with anticoagulation therapy (continuous administration of intravenous heparin, 15,000 U/day). However, 14 days after the first endovascular treatment, the patient developed distal ischemia following internal fixation. Emergency angiography showed re-occlusion of the popliteal artery caused by formation of a thrombus adhering to the intimal flap (Fig. 1e). Bending of the popliteal artery was also observed. We assumed that the re-occlusion was caused by distortion of the vessel, which probably occurred during the internal fixation. As a secondary treatment, balloon inflation of the true lumen and aspiration thrombectomy with a 5-French guiding catheter (Launcher; Cordis, Bridgewater, NJ, USA) were performed. The thrombus was removed, and recanalization and sufficient peripheral blood flow were again achieved.
After the two sessions of endovascular treatment, adequate blood perfusion was maintained (Fig. 1f), and the patient was moved to a rehabilitation hospital 55 days after admission. Ischemia did not recur during the 15-month follow-up period.
Patient 2
A 74-year-old woman with knee osteoarthritis underwent left total knee
replacement. Around 3 h postoperatively, she developed calf pain, swelling, and
loss of the distal pulses in the foot. Compartment syndrome of the lower
extremity caused by acute arterial occlusion was suspected, and the patient was
transferred to our hospital 12 h after the initial operation. Emergency
angiogram of the left leg showed focal thrombotic occlusion and dissecting
pseudoaneursym of the popliteal artery (Fig. 2a), which we diagnosed as
iatrogenic intimal injury. The patient continued to suffer from compartment
syndrome and experienced vasospasm in the leg; as surgical reconstruction was
considered to be difficult, endovascular recanalization was attempted. The
thrombus was removed by aspiration thrombectomy with an 8-French guiding
catheter (Launcher; Cordis, Bridgewater, NJ, USA) inserted via the antegrade
approach from the left common femoral artery; however, the intimal flap and
dissecting pseudoaneurysm remained. Moreover, severe vasospasm was noted in the
distal arteries of the leg (Fig
2b). The primary goal was to prevent limb loss. Therefore, a bare
stent of 6-mm diameter and 4-cm length (E-Luminexx; BARD, Tempe, AZ, USA) was
placed to cover the injured site. A 74-year-old woman with
popliteal artery occlusion due to iatrogenic injury (Patient 2). (a)
Left lower extremity angiogram showing focal thrombotic occlusion
(arrow) and dissecting pseudoaneurysm (arrowhead) of the popliteal
artery. (b) Despite thrombectomy, the intimal flap (arrow),
dissecting pseudoaneurysm, and vasospasm of the distal arteries
(arrowhead) remained. (c) Follow-up angiogram 1 week after stent
placement showed satisfactory peripheral blood flow and
disappearance of the pseudoaneursym (arrow: bare
stent).
Immediately after recanalization, remarkably high pressures of 90 mmHg in the lateral compartment and 83 mmHg in the anterior compartment were confirmed. Therefore, fasciotomy was performed in the lateral, anterior, posterior, and deep compartments, and satisfactory peripheral blood flow was achieved (Fig. 2c). The patient was moved to another hospital for rehabilitation 28 days after admission. She could stand and walk unaided after rehabilitation, and ischemia did not recur during the 12-month follow-up.
Discussion
In the cases presented here, we performed balloon angioplasty with long inflation time, aspiration thrombectomy, and stent placement to manage traumatic popliteal artery occlusion. The procedures were successful, and promising clinical outcomes were achieved. With regard to the reported risk factors for limb loss (1), site of injury (popliteal artery) and associated injury (compound fracture) were risk factors in Patient 1, and site of injury (popliteal artery) and clinical status (compartment syndrome) were risk factors in Patient 2. Despite the high amputation risk and difficult surgical procedures, we successfully salvaged the lower limbs of both the patients.
Acute limb-threatening ischemia after blunt arterial trauma is usually managed by surgical bypass of the affected artery. However, in trauma cases, open reconstruction is difficult because of lower-extremity edema and vasospasm of the injured vessels (6). Patient 1 had compound open fractures with contaminated wounds, so surgical bypass was considered to have a high infection risk. Patient 2 had compartment syndrome and severe vasospasm in the lower leg; therefore, surgical bypass was a difficult option. Endovascular recanalization was assessed to be a suitable alternative to surgery. Advancements in endovascular and imaging techniques have allowed successful treatment of peripheral arteries and helped to overcome some of the obstacles in surgical repair. In particular, balloon angioplasty in combination with surgery, transcatheter embolization of hemorrhagic lesions, and stent or stent graft placement for dissecting or hemorrhagic lesions have been introduced (2,7). However, reports of treatment of occlusive lesions are limited (6).
Balloon angioplasty with long inflation time, the technique we employed to reduce the intimal flap, is used for treating infra-inguinal stenotic or occlusive lesions induced by obliterating arteriosclerosis (8). In Patient 1, we re-approximated the intimal flap and achieved and maintained sufficient peripheral blood flow through the repaired true lumen. Aspiration thrombectomy is used to treat thrombotic arterial occlusion (peripheral, intracranial, or coronary arteries) or peripheral venous and pulmonary arterial thromboembolism (9). We used this method to achieve sufficient removal of the thrombus in both cases. In Patient 2, we placed a bare metal stent into the P2-3 segment of the popliteal artery. Although stent placement up to the P3 segment is associated with a high risk of stent fracture and re-occlusion (10), this procedure was necessary for our patient. She had compartment syndrome of the lower leg, so immediate recanalization was very important in her case. Non-conformance of the stent was not observed during the 12-month follow-up period.
In conclusion, the combination of balloon angioplasty, aspiration thrombectomy, and stent placement is an alternative method to surgical bypass for treating traumatic popliteal artery occlusion even in cases with high amputation risk.