
Abstract
We report a case of nodular fasciitis of the breast mimicking malignant tumor. A 41-year-old female patient with a palpable mass in the upper center of the left breast present for 1 week visited our hospital. A mammogram showed an oval isodense with a partially indistinct margin. Ultrasonography demonstrated a hypoechoic mass, 8 × 11 mm in size. Breast cancer could not be excluded based on mammographic and ultrasonographic (US) findings. A core needle biopsy and excisional biopsy were performed. Histopathologic examination revealed a diagnosis of nodular fasciitis of the breast. The mammographic and US findings of nodular fasciitis in the breast is reviewed.
Introduction
Nodular fasciitis is a benign fibroblastic proliferation of cells characterized by sudden appearance and rapid growth. The lesion is usually found in the soft tissue of the upper extremity and trunk in middle-aged individuals. It has been rarely described in the breast (1–7). Clinically, it presents as a palpable mass, which may mimic malignancy. We report the imaging findings and a brief literature review of nodular fasciitis of the breast.
Case report
A 41-year-old woman visited our hospital with the chief complaint of a palpable mass
in her left breast, which she had noticed 1 week prior. There was no history of
trauma or family history of breast cancer. A mammogram showed a 10-mm oval isodense
mass in the upper center of the left breast with a partially indistinct margin
(Fig. 1), which was
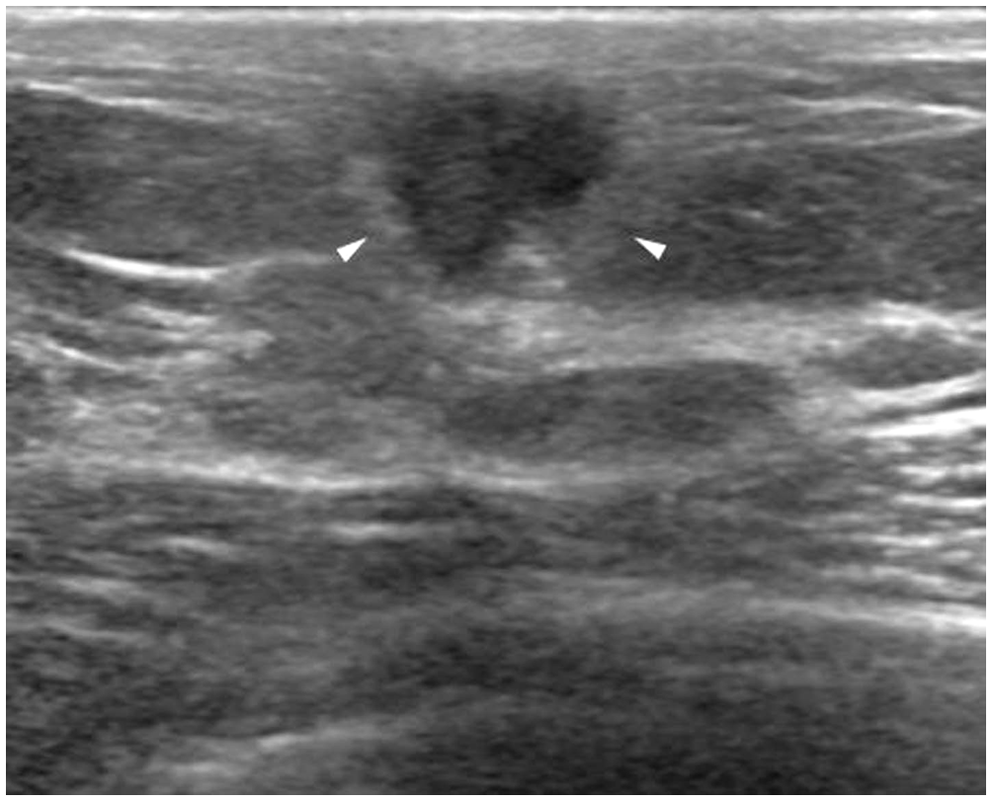
newly developed in comparison with her last mammogram 6 years ago. Ultrasonography
revealed an 8 × 11 mm, irregular, hypoechoic, microlobulated mass with echogenic
halo (Fig. 2) at the 12
o’clock position of the left breast. This finding was suspicious of malignancy;
therefore, she underwent an ultrasound-guided core needle biopsy. A
41-year-old woman with nodular fasciitis of the breast. (a) The
mediolateraloblique view of mammography showed a 10-mm-diameter oval
isodense mass with partially indistinct margin in the upper center of
her left breast (with a BB-marker). Ultrasonography at the 12 o’clock position of the
left breast revealed an 8 × 11 mm, irregular, non-parallel, hypoechoic
mass with microlobulated margin and echogenic halo (arrowheads). The
superficial margin of the mass touches the skin line and the deep margin
is located on the fibroglandular tissue.
Histologically the lesion had an ill-defined proliferation of short spindle cells admixed with occasional giant cells. Nodular fasciitis or spindle cell carcinoma was ruled out.
Excisional biopsy was done for further evaluation. Histopathology of excisional
biopsy showed nodular proliferations of short spindle cells and occasional giant
cells with dense collagenous stroma and surrounding chronic inflammatory cells,
consistent with nodular fasciitis (Fig. 3). Photomicrograph showed the features of nodular
fasciitis with nodular proliferation of spindle to oval cells and giant
cells admixed with collagenous stroma (H&E,
×200).
Discussion
Nodular fasciitis is a benign fibroblastic proliferative and reactive process of the soft tissues related to fascia. The most common site of nodular fasciitis is the subcutaneous tissue of the upper extremity. It can occur virtually anywhere in the body (8), but reports of its occurrence in the breast are rare. The most consistent characteristic of the lesion is a solitary, frequently painful and tender mass, leading to early presentation with the history typically being weeks instead of months. Cases occurring in the breast may have findings on mammography and ultrasound consistent with malignancy (3). To our knowledge, 19 reports of nodular fasciitis in the breast have been published, and only six case reports have presented imaging findings (1–6). A history of trauma may precede these reactive lesions, but the cause remains unknown. Nodular fasciitis can be divided into subcutaneous, intramuscular, and fascial types depending upon its relationship to anatomic location (9). Lesions in nodular fasciitis could be separated into three types based on a range of histological features: myxoid, cellular, and fibrous. The different types are roughly correlated with the duration of the nodule (10). Nodular fasciitis in the breast needs to be distinguished from benign and malignant breast tumor with non-specific findings, suspicious for malignancy (4,7) and the histological differential diagnosis of nodular fasciitis includes spindle cell tumors such as fibromatosis, myofibroblastoma, spindle cell lipoma, solitary fibrous tumor, phyllodes tumor, spindle cell metaplastic carcinoma, spindle cell melanoma, fibrosarcoma, and leiomyosarcoma. They can be differentiated based on cellularity, nuclear features, collagen content, and growth pattern (4). Sometimes, immunohistochemistry staining such as S-100, CD34 and cytokerain can be helpful for the differential diagnosis (4).
Previous reports of nodular fasciitis of the breast.

CNB, core needle biopsy; FNA, fine needle aspiration.
These differences in radiographic appearance may indicate that when the lesion becomes more mature, it becomes more fibrotic. Also, the US imaging findings may depend on the histologic characteristics of nodular fasciitis (2,3,9,11). The histologic type in our case was mixed cellular with a fibrous component. The mammogram showed a partially circumscribed and partially indistinct mass. On ultrasound, the lesion was irregular, non-parallel, and hypoechoic with a microlobulated margin and echogenic halo. These suspicious imaging features of nodular fasciitis show an alarming similarity to breast malignancy.
The treatment of nodular fasciitis is excisional biopsy because of the difficulties in distinguishing between nodular fasciitis and sarcoma by radiological appearance (2,4,9). Some authors are of the opinion that conservative management may be considered for suspected nodular fasciitis lesions because spontaneous resolution has been reported (11). Recurrence of nodular fasciitis after surgical removal is rare (11,12). Conservative management may be appropriate in cases with benign results from core needle biopsy and typical clinical history. However there are many spindle cell tumors to differentiate with nodular fasciitis. If the pathologic diagnosis is not conclusive, surgical biopsy should be considered.
In conclusion, nodular fasciitis is a rare breast lesion that can be confused with both benign and malignant tumors. Nodular fasciitis shows hyperdensity and a spiculated margin on mammograms, and hypoechogenicity with a non-circumscribed margin, echogenic halo, or non-parallel orientation on US imaging findings. Pathological examination by core needle biopsy is usually required for diagnosis. Radiologists should be aware of the clinical behavior, imaging features, and histopathologic features of nodular fasciitis to avoid a misdiagnosis.