
Abstract
Caseous calcification of the mitral annulus is a rare form of chronic degenerative process in the mitral valve fibrous ring with a mass-like appearance that has to be in the differential of the radiologist and cardiologist. We present the case of an 82-year-old woman in whom a tumor-like calcified mass in the posterior side of the mitral valve annulus was detected at echocardiography, and the diagnosis of caseous calcification was confirmed on multidetector computed tomography (MDCT). The diagnostic features of this rare cardiac mass are described.
Keywords
Introduction
Unlike common mitral annular calcification, caseous calcification of the mitral annulus is a relatively rare variant that has a distinct appearance. Usually found in elderly patients, it is typically located in the posterior mitral annulus. This disorder generally appears as a large spheric mass-like calcification with a central echolucent area that may lead to diagnostic errors. Hence, it needs to be differentiated from other potentially serious conditions as it has a benign prognosis. Cardiac imagers should be familiar with this rare form of periannular calcification. The present case refers to a patient with a mass-like calcification of the mitral annulus. An evaluation of the mass was provided at transthoracic and transesophageal echocardiography; and the diagnosis confirmation as well as the differential diagnosis were obtained by the use of multidetector computed tomography (MDCT).
Case report
An 82-year-old woman with a history of high blood pressure and hyperlipidemia underwent a routine transthoracic echocardiography (Fig. 1) which showed a large hyperechogenic mass, located at the posterior side of the mitral valve annulus and not associated to valvular dysfunction. Thus, a transesophageal echocardiography was completed and revealed this hyperechogenic mass with a heterogeneous central area resembling liquefaction. An atrial mass was suspected and to better evaluate this mass, a MDCT was performed (Figs. 2–4), showing a hyperdense mass with hypodense center and a calcified peripheral rim located at the anterior and posterior mitral ring. The central content had heterogeneous fluid density without significant contrast enhancement. The MDCT findings were considered highly suggestive of caseous calcification of the mitral annulus. The patient was asymptomatic at the time of diagnosis and was treated conservatively. Surgery was not needed due to the absence of co-existent mitral valve lesions. The echocardiographic follow-up at 6 months showed no significant changes.
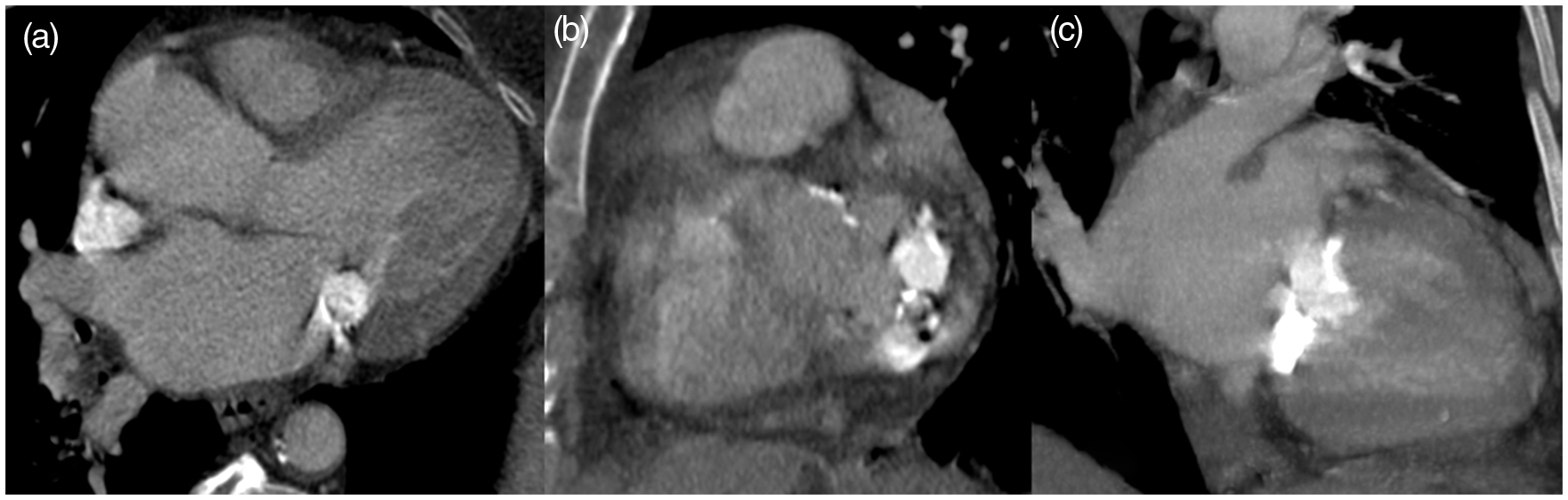
Transthoracic echocardiographic: apical four-chamber view (a), parasternal long axis (b), and short axis (c) views: showing an echodense, spherical, tumor-like mass located in the region of posterior mitral annulus (arrowheads), with a heterogeneous central area (arrow). Note that acoustic shadowing artifacts behind the calcification are absent. Ao, aorta; LA, left atrium; LV, left ventricle; MV, mitral valve. MDCT in axial (a, b) and four-chamber (c, d) views after injection of contrast: a hyperdense mass with hypodense unenhanced center and a calcified peripheral rim located at the anterior and posterior side of the mitral valve annulus. The four-chamber view shows the crescent-shaped dense mass. MDCT, long axis (a), short axis (b), and two-chamber (c) views: a tumor-like mass with a hypodense central area and peripheral dense calcification in the mitral valve annulus. Short-axis view (b) shows heterogeneity of the caseous calcification; this is confirmed by widely varying densities, including low attenuation value indicating fatty degeneration, as well as very high values indicating dense calcifications. Two-chamber view of the mass (c) demonstrates the close relation to the mitral valve. Volume-rendered CT image (a) shows the caseous calcification in the periannular region of the mitral valve (arrow). Coronal view of the caseous calcification, with maximum intensity projection reconstruction (MIP) (b).


Discussion
The caseous calcification of the mitral annulus, also called liquefaction necrosis, is a rare form of chronic degeneration that affects the fibrous skeleton of the mitral annulus (1). It is a less defined form of mitral periannular calcification which has been generally ignored up to recently (2). This condition is frequent in the elderly, mainly in women, without known clinical significance (3,4), which was the case in our patient. In fact, this disorder is observed at autopsy in 8% of the population, but rarely seen in imaging (1), occurring in <0.07% of patients of all ages who undergo echocardiography (5,6). The pathogenetic mechanism of the caseous calcification of mitral annulus has not yet been defined; but as an expression of atherosclerosis, it has identical risk factors as cardiovascular disease (1).
Typically, it is located at the level of the posterior mitral ring, sometimes extending to the whole mitral annulus and involving the mitral valve apparatus (3,4). However, in some cases, the differential diagnosis with other disorders is difficult. In fact, mitral annulus calcification may appear differently depending on its evolution stage: mitral annulus calcification; homogeneous calcified mass of the mitral valve; or liquefaction necrosis of the mass (7).
Caseous calcification is characterized echocardiographically as large, round, tumor-like calcifications, with well-defined edges, echodense periphery and a central echolucent area resembling liquefaction. It is less reflective than common calcification of mitral annulus, and usually there are no posterior acoustic shadowing artifacts behind it (1,3,6). Due to its unusual characteristics, a tumor may be suspected and the distinction should be based on the typical location of calcification, the possible extension to the whole mitral annulus, the well-defined borders, and the internal echolucent area. In some cases, transesophageal echocardiography can add more precise information regarding the internal area of the mass (8). In our patient, the transesophageal echocardiography permitted detection and evaluation of the central area of the mass.
On MDCT, this entity appears as a round or semilunar sharply marginated mass with a hypo- or hyperdense center and a calcified peripheral rim (1). Heterogeneity of the content is confirmed by the varying densities that can be seen, ranging from negative Hounsfield units suggesting fatty degeneration to dense material (9). The characteristic features are echodensity, sharp margins, peripherally denser calcification, very high Hounsfield units, and absence of enhancement after contrast agent administration (5,9).
Caseous calcification is often misdiagnosed as a cardiac tumor, thrombus, abscess, or even hydatid cyst, which may lead to unnecessary investigations and interventions (5,9). In our patient, the use of multislice CT permitted a correct diagnosis, showing clearly the characteristic features of caseous calcification of the mitral annulus.
Cardiac magnetic resonance imaging (MRI) may be used to exclude some potential etiologies (3,10), showing a typical behavior for the caseous calcification in different sequences: hypointense signal in gradient echo, T1-weighted and T2-weighted sequences, without late enhancement.
Blankstein et al. (10) highlighted the complementary role of different imaging modalities. They showed that echocardiography is helpful to detect the mass and to assess its functional significance, and that conventional CT imaging confirms the calcified nature of the mass and optimally demonstrates the transformation into caseous necrosis. Cardiac MRI can be used to exclude other etiologies.
Concerning the treatment of caseous mitral calcification, there is no clear consensus. Indeed, these lesions generally carry a benign prognosis and do not require specific treatment. Surgery is needed only in rare instances of severe valvular dysfunction (1,5). Fujiwara et al. (11) illustrated a case of a patient who was treated for caseous calcification by mitral valve replacement, because of the presence of mitral stenosis with an elevated transmitral mean pressure gradient. Surgery, when performed shows usually a central area filled with a toothpaste-like material composed of calcium, fatty acids, and cholesterol, explaining its heterogeneity on MDCT (1). Histological analysis, reveals a pasty, acellular substance that is culture-negative and free of cancerous or inflammatory cells (6).
In conclusion, the caseous calcification of the mitral annulus is a rare, benign condition, found incidentally when performing an echocardiographic study. With the increasing use of MDCT, this incidental lesion may be more commonly encountered in clinical practice and cardiac imagers should be familiar with it in order to avoid misdiagnosis.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.