
Abstract
Background
Neuroendocrine tumors (NET) represent a therapeutically challenging and heterogeneous group of malignancies occurring throughout the body, but mainly in the gastrointestinal system.
Purpose
To describe magnetic resonance imaging (MRI)-guided laser ablation of NET liver metastases and assess its role within the current treatment options and methods.
Material and Methods
Two patients with NET tumor hepatic metastases were treated with MRI-guided interstitial laser ablation (LITT). Three tumors were treated. Clinical follow-up time was 10 years.
Results
Both patients were successfully treated. There were no local recurrences at the ablation site during the follow-up. Both patients had survived at 10-year follow-up. One patient is disease-free.
Conclusion
MRI-guided laser ablation can be used to treat NET tumor liver metastases but combination therapy and a rigorous follow-up schedule are recommended.
Introduction
Neuroendocrine tumors (NET) represent a diverse group of malignancies occurring throughout the body, the estimated incidence is 5.25/100,000 and is increasing (1), though the reason for this phenomena remains unknown. NETs are the most common small bowel tumor (2) and overall the incidence of NETs in the gastrointestinal system is common (3). They share a typically indolent growth pattern and manifest often symptoms related to tumor-induced hormonal secretion. NET patients frequently suffer from neuroendocrine tumor liver metastases (NETLM). It has been estimated that 46–93% of NET patients have NETLMs at the time of diagnosis (4). Although these tumors progress slowly, the 5-year survival of NET patients with NETLMs is 40% compared to that of 75–99% in patients free of liver metastases (5).
Surgery is considered as the only potentially curative treatment method for the NETLMs. Surgical removal is typically considered if the disease is restricted to the liver, although surgical tumor debulking can be considered to control carcinoid syndrome in selected cases. Unfortunately, only <20% of patients with NETLMs are candidates for hepatic resection (6,7). Liver transplantation for metastatic NETs remains controversial (8).
The preferred primary treatment of NETLMs is surgical management, followed by liver-directed therapies, or a combination of these procedures (8). Liver-directed therapies include thermal ablation, hepatic artery (chemo)-embolization, and selective intra-arterial radiation therapy. It is known that ablative techniques may have curative potential when small liver tumors are treated. Of thermal ablation techniques, the radiofrequency ablation is most widely used (9,10). Other modalities that can be used to achieve local ablation are laser-induced thermal therapy (LITT), cryoablation, microwave therapy, electroporation, and high intensity focused ultrasound (HIFU) but there are very few, if any, reports with any of these methods in conjunction with treating NET tumor liver metastases. All ablative techniques are based on the cytotoxic effects of non-physiologic temperatures that are focally induced within the treated tumor by percutaneously or perioperatively placed probes (apart from HIFU, which is totally non-invasive). Ablation techniques can be applied in the setting of inoperable disease, or, at the surgeon’s discretion as a complement to resection (11). Indications for image-guided ablation are recommended as follows: adjunct intraoperative ablation; ablation in non-surgical patients; ablative debulking for symptom relief; and ablation of metastatic relapse after surgery (12).
Other NET therapy is mainly systemic and not specifically targeted to the liver but rather towards universal tumor volume in the body. The number of therapy options is voluminous, and their utilization partially depends on whether the tumor is hormonally an active functioning tumor or an inactive non-functioning tumor (5).
The target is to suppress the symptoms and the disease progression. Treatment is palliative, typically applied in a situation where there is systemic disease involvement and possible disease progression according to RECIST criteria (13). These therapies include somatostatin analogs, proton pump inhibitors, systemic peptide receptor radionuclide therapy (131I-mIBG, 90Y-DOTATOC, 90Y-DOTATATE, 177Lu-DOTATATE), chemotherapy, interferon-α, targeting vascular endothelial growth factors (sunitib), targeting mTOR pathway and micro RNA-regulated pathways (everolimus) (8).
Laser (Light Amplification by Stimulated Emission of Radiation) has been investigated and used in medicine since the 1960s. It currently permeates nearly every area of modern medicine from early diagnostic to therapeutic uses (14). Laser-induced thermotherapy has been used successfully to treat tumors in the brain, lung, prostate, kidneys, and liver (15,16).
Magnetic resonance imaging (MRI) provides excellent soft tissue contrast resolution and can be used guide percutaneous ablative therapy (16,17). MRI also is the only imaging modality that allows for noninvasive, real-time temperature monitoring during ablation procedure using a visualization of relative temperature values of the tumor and surrounding healthy tissue, here the proton resonance frequency (PRF) is the most widely used method but the thermal T1 effect can also be utilized (18–20).
It has been shown that laser-induced interstitial thermotherapy can help to achieve survival rates similar to those seen with surgical resection in liver metastases from colorectal and breast cancer, as well as in other abdominal tumors, although randomized studies are scarce (21). The largest published series of any percutaneous ablative technique is from laser ablation, the series consisted of liver metastases mainly from colorectal carcinoma (17).
A few small series and case reports of local ablative treatments have shown good response in liver metastases from NETs (5,22). Specific MRI-guided laser ablation reports on NETMLs management are still absent.
The purpose of this report is to describe technique for MRI-guided laser ablation of NET liver metastases and present the treatment results of two patients.
Material and Methods
Two patients with hepatic metastases from NET were treated. Informed consent from both patients and institutional ethical statement were acquired. In all, three tumors were treated. A preprocedural (1.5 T) abdominal MRI was performed for both patients prior to the laser ablation. A low field 0.23 T C-arm MRI scanner was used for imaging and procedural guidance. Postoperative imaging with MRI (1.5 T) or computed tomography (CT) was performed at intervals of 6 months to 1 year during the follow-up period.
Patient 1
Patient 1 is a 53-year-old man, who was diagnosed with Zollinger-Ellison syndrome, with elevated gastrin hormone and chromogranin A (CgA) levels at the age of 32 years. At that time, a primary resection was performed and small tumors from ventricle were excised (sporadic gastrinoma with low proliferation markers [Ki-67, low mitotic index]), and without further local or systemic involvement of the disease at that point. Ten years later there was an increase in the hormonal levels and one biopsy verified metastatic lesion was detected in the liver at segment VIII, size 2.8 × 2.6 × 2.5 cm. Surgical tumor resection and laser ablation were the primary treatment options considered and the ablation was chosen due to the patient’s preference and high likelihood of disease progression over time.
Patient 2
Patient 2 is a 65-year-old man who was diagnosed with jejuneal NET tumor, with synchronous metastatic spread to right liver lobe, at the age of 52 years. There was no abnormal hormonal activity detected at that time (normal CgA A and 5-hydroxyindoleacetic acid [5HIAA] levels) and tumor was of low proliferation type (Ki-67, low mitotic index). The primary operation included resection of hepatic metastases through right hepatectomy. Three years later, the patient developed two biopsy-verified metastatic lesions at the remaining left hepatic lobe (segment II, size 1 × 1 × 1 cm and segment III, size 2 × 2 × 2 cm). Due to the previous resection history laser ablation was chosen as a second line therapy option.
Procedural imaging and ablation
A resistive type horizontally open MRI scanner (Panorama I/T, 0.23 T, Philips Medical Systems, Vantaa, Finland) with optical instrument guidance hardware and software was used. The detailed description of the system has been provided elsewhere (23). MRI was used for procedural lesion localization, instrument guidance, thermal monitoring, and postprocedural imaging.
Ultrasound (US) (Toshiba powervision 7000, Toshiba Corp., Shimoishigami, Japan) was used as an additional operative imaging modality. Both patients received intravenous (i.v) prophylactic antibiotics, cefuroxime 1.5 g i.v., before the procedure.
Patient 1 was treated under spinal epidural anesthesia due to lesion localization and co-morbidities and Patient 2 was treated under general anesthesia.
Tracking software produced graphic overlay and instrument susceptibility in MRI
image sets were used as a reference to advance the needle to the target (24) or alternatively US
was used. After reaching the target, needle was replaced with laser treatment
instrumentation under MRI guidance (Fig. 1). Needle insertion, laser
fiber introduction and thermal monitoring of treatment. (a) Patient
2, liver tumor at segment 3. Needle (arrows) is inserted to the
tumor (arrowheads) under MR guidance. (b) Patient 2, laser fiber
(arrows) introduced into the tumor (arrowheads), same location as in
(a). (c) Patient 2, thermal monitoring of laser treatment, MRI
signal decrease is evident in the tumor area (arrowheads) after
10 min of treatment. Same location as in (a,
b).
Laser therapy was performed with a diffusor type laser fiber (diameter, 400 µm; Dornier Medizin technik, Germering, Germany) and MR-compatible irrigated 9 French laser catheter kit (Somatex GmbH, Berlin, Germany). We used A Nd-Yag type laser device with maximum power of 100 watts (W) (Fibertom medilas, Dornier Medizin technik, Germering, Germany). When several fibers were used simultaneously, a laser beam splitter was applied to facilitate synchronous energy delivery from two fibers simultaneously (Dornier Medizin technik, Germering, Germany). During laser treatment, a constant energy flow and power of 10 W/cm for active fiber section were maintained. Active fiber section lengths of 2 cm (n = 1) and 3 cm (n = 3) were used. Tumor geometry in preprocedural MR images was used to determine the number of laser applicators used for each tumor. The need for possible fiber realignment was determined by evaluating the fibers relation to lesion geometry in procedural guidance images. The need for possible second burn was evaluated using the procedural treatment images and the heat induced signal void spread. Additionally, treatment result was assessed using postoperative imaging and additional therapy session was to be scheduled if necessary. The laser treatment constant energy flow and power of 10 W/cm for active diffusion fiber length. The treatment was monitored using gradient echo MRI imaging (B-FFE3D; TR, 7.7 ms; TE, 3.8 ms; slices, 8; slice thickness/interval, 6.0/6.0 mm; field of view [FOV], 380 × 380; matrix, 160 × 160; FA, 63 degrees; acquisition time, 24 s) observing the change in T1 signal intensity, which was expressed as a signal void in the image (Fig. 1). This signal void was attributable to the temperature change in the heated tissue. The imaging sequence was repeated at 1 min 30 s intervals. In cases where the imaging sequence did not initially cover the lesion area entirely it was repeated in the orthogonal plane to the preceding sequence in order to better evaluate the signal void spread.
When the signal void spread beyond the tumor edge by a 0.5 cm margin or after a minimum of 15 min, the treatment was considered to be complete and the laser fiber, laser irrigator, and introducer sheath hosting the two devices were removed. Tissue glue (Tisseel duo, Baxter AG, Vienna, Austria) was injected into the treatment channel while retracting the introducer sheath.
Postprocedural imaging
Follow-up imaging was performed twice during the initial procedural hospital
stay. First scan was initialized within 30 min from the completion of the
treatment. Here, a T2-weighted respiratory-gated image set was acquired (T2 FSE;
TE, 140 ms; TR, 5000; slices, 14; slice thickness/interval, 7/8 mm; FOV,
360 × 309 mm; matrix, 256 × 216, estimated acquisition time, 5 min). Then,
contrast-enhanced sequences were acquired. First a breath-hold, T1-weighted
dynamic (Fig. 1) (T1
FE3D; TR, 13 ms; TE, 5.2 ms; slices, 64; slice thickness/interval, 7/7 mm; FOV,
350 × 350 mm; matrix 192 × 192; FA, 20 degrees; acquisition time, 33 s) sequence
image set without fat saturation was acquired before the contrast agent
administration. Contrast agent, 0.1 mmol/kg of gadopentetate dimeglumine
(Magnevist; Bayer Schering Pharma AG, Berlin, Germany), was then rapidly
injected via the cubital vein, followed by 30 cc saline flush. The T1-weighted
dynamic sequence was repeated at 10 s, 60 s, 110 s, and 200 s from the contrast
injection. After this, a T1-weighted contrast-enhanced sequence was obtained
(T1, FSE; TE, 14 ms; TR, 500 ms; slices, 12; slice thickness/interval, 7/8 mm;
FOV, 360 × 300 mm; matrix 324 × 270; acquisition time 5 min 40 s). The patients
were monitored for 6 h in the recovery room. The previously described MRI
protocol was repeated at 72 h from the treatment (Fig. 2) and the patients were dispatched
from the hospital. The further imaging protocol was scheduled to occur with in
clinical follow-up schedule, first two computed tomography (CT) or MRI scans
with 6-month intervals, followed by clinical follow-up with either MRI, CT, or
US imaging performed annually. Postprocedural MRI at 72 h after
therapy: Patient 2, dynamic T1-weighted imaging. Ablation sites are
depicted as non-perfusing regions (arrowheads) in segments II and
III.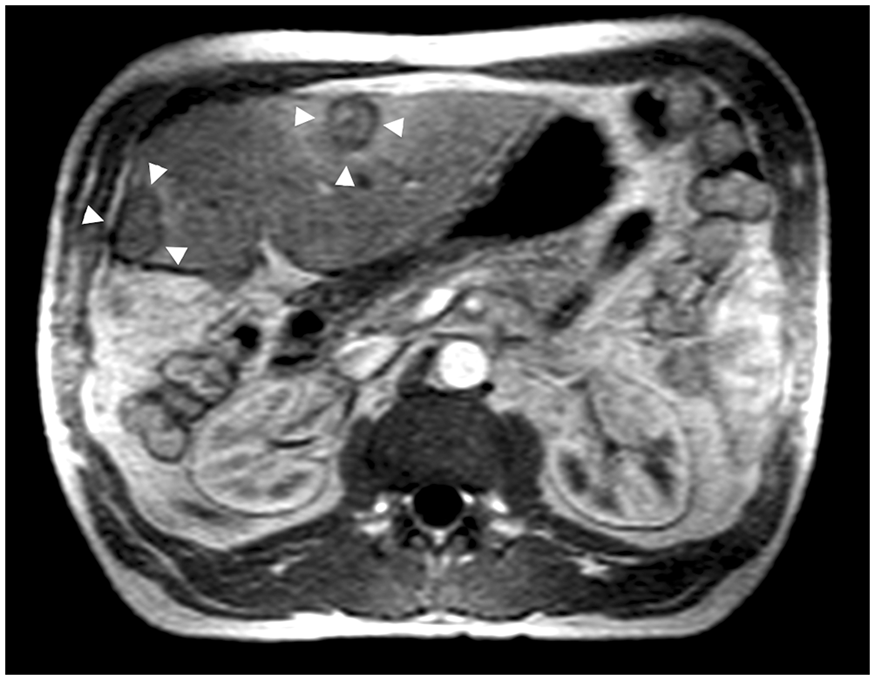
Results
Both patients were treated successfully with complete tumor ablation. The procedural times were 80 min and 126 min. There were no significant complications, but one patient (Patient 1) developed slight pleural effusion, segmental hepatic tissue, and capsular edema at a treatment site, which did not require further treatment. The energies delivered to tumors were: Patient 1, 54,000 Joules (J); and Patient 2, 12,000 J and 21,600 J at segments II and III, respectively.
During the follow-up, Patient 1 has remained disease-free with normal gastrin and GgA
levels (disease-free survival, 10 years; total survival, 21 years) (Fig. 3). He has been receiving
medical treatment (omeprazol) to prevent gastric symptoms but is currently without
medication. (a) Therapy follow-up, Patient 1, MRI at 72 h
after therapy. Dynamic T1-weighted imaging. Ablation site is depicted as
non-perfusing region (arrows) in segment VIII. (b) Therapy follow-up,
Patient 1, contrast-enhanced CT 7 years after therapy. Venous phase.
Ablation site is depicted as a small scar-like non-perfusing region
(arrows) in segment VIII.
Patient 2 had increasing CgA levels 3 years after the laser ablation and a concomitant octreotide scan revealed two new small metastatic lesions in liver and also one small extrahepatic, paraspinal lesion. Due to the extrahepatic disease, further invasive treatment was not chosen and treatment with somatostatin analogue medicinal therapy was initialized (Sandostatin LAR, long-acting repeatable, Novartis, Nürnberg, Germany). Since that time, patient CgA levels have remained stable but he has developed two additional metastatic lesions to the liver at new locations (5 years after initial laser ablation). The disease has remained stable for 5 years and the patient was free from carcinoid syndrome symptoms for 9 years from the initial laser ablation. Total survival time is 13 years. Due to lack of symptoms and currently stable tumor situation, no immediate local ablative therapy has been planned.
Discussion
Treatment options for hepatic metastases of neuroendocrine tumors are numerous and several treatment algorithms have been published (8,11,22,25). In general, the treatment must be tailored specifically to the patient by a multidisciplinary group of oncologists, surgeons, interventional radiologists, and endocrinologists.
Depending on the tumor grade, which is determined by the cellular proliferation (Ki-67, mitotic index), the NET tumors have a variable progress rate and thus patient survival is also capricious. Advances in loco-regional disease control and pharmacotherapy have led to better management and survival of NET patients. It is evident that as the survival times of these patients increase, and the prevalence of NET patients increases, the health system needs increased awareness of how to manage these patients. Here especially, the symptoms present a significant, quality of life (QoL) issue. This is especially pertinent should the patient have carcinoid syndrome. Symptoms can often be effectively controlled by medication but sometimes tumor mass removal or debulking through surgery or ablation is warranted for QoL amelioration. In our report, institutional multidisciplinary team of surgeons, oncologists, endocrinologists, and radiologists made treatment decisions and utilized these methods for patients benefit.
Both of our patients show long survival: one is disease-free and the other is symptom-free although with new hepatic metastases. The first of our patients undoubtedly would not be disease-free without the ablation. The second patient has two new metastases and it is impossible to estimate which part of his survival is contribution of the ablative treatment or pharmacological therapy and which is due to the indolent nature of the disease. It is remarkable that neither of our patients developed local recurrences at the primary operation or ablation sites.
As previously addressed, thermoablative treatments are effective in treatment of different types of hepatic tumors and MRI is feasible in monitoring thermal effects in tissue during and after the treatment (26–29). MRI is particularly well suited for thermal therapy monitoring as it enables multiplanar thermal monitoring during the ablation using either T1 effect or PRF-method. Also the novel development of miniaturized instruments (30,31) to achieve thermal laser ablation make the procedure less invasive and comparable to other thermal therapy methods, such as radiofrequency ablation, cryotherapy, interstitial electroporation, microwave, and brachytherapy. It must be acknowledged that most of these methods, apart from cryotherapy, do not facilitate seamless utilization of intraoperative MRI monitoring. We had no significant complications associated with the LITT and it is generally acknowledged that percutaneous ablative therapies are safe. There were no local recurrences at the treated liver site in our patients and it seems that MRI guidance combined with laser ablation may be more accurate in lesion obliteration than radiofrequency ablation when liver metastases are considered (32). Concerning NETs, our experience shows, and as others have noted (33), that in the treatment of NETLMs a multidisciplinary approach is of paramount importance.
In conclusion, laser-induced thermotherapy implemented with MRI, MRI guidance, monitoring, and careful clinical follow-up seems to be the safe and feasible method to manage endocrine tumor liver metastases in a situation where other treatment paradigms are not possible.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.