
Abstract
Acute intestinal ischemia continues to be a challenging diagnostic problem with high mortality. We describe a rare case of acute intestinal necrosis, due to vasculitis, related with chemotherapy.
A patient was examined in our emergency department, presenting with abdominal pain. Three months before he had undergone an operation for lung carcinoma (lobectomy) and received chemotherapy.
CT of the abdomen demonstrated free air in 10 different locations: hepatic part of the portal vein, branches of mesenteric veins, femoral and iliac veins, the bowel wall, peritoneal cavity and retroperitoneal space, abdominal muscles, inguinal canals, meso-sigmoid space, and in the para-rectal space. Moreover, pathological findings revealed that the free air in the peritoneum and retropneumoperitoneum occurred without intestinal perforation, but with transudation through the necrotic bowel wall. This is a rare complication of chemotherapy. This case refers to the unusual CT findings which appeared in this patient. The key to a better outcome is early diagnosis of this condition and the CT examination of the abdomen plays an important role.
Introduction
Recent literature about vasculitis due to chemotherapy includes predominantly case reports, and mesenteric vasculitis is a very rare complication (1,2).
To our knowledge this is the first published report in the literature, which refers to a rare complication of chemotherapy, vasculitis, which in this case caused extensive intestinal necrosis. Due to delayed diagnosis, large amounts of air transudation appeared within the necrotic bowel wall, in the peritoneal cavity and in the retroperitoneal space. There are very few reports in the literature referring to free air in the retroperitoneum, both femoral veins as well as free air in the inguinal canal.
Case report
A 64-year-old man with a history of lung cancer (treated with lobectomy and chemotherapy with cisplatin and etoposide, 3 months before) was examined in our emergency department suffering from diffuse abdominal pain starting 6 days previously. The patient presented with abdominal fullness and constipation lasting for 3 days.
Physical examination revealed rebound tenderness and heart rate 100 bpm. Laboratory exams showed: WBC, 1100 cells/mm3 (NEUT = 44%); HCT, 32%; CRP, 360 mg/dL; K, 5.9 mEq/L; Na, 132 mEq/L; PLT, 69,000; Tbil, 2.90 mg/dL; Dbil, 1.90 mg/dL; CPK, 2530 U/L; LDH, 670; Na, 132 mEq/L; K, 5.9 mEq/L; SGOT, 180; SGPT, 183.
Abdominal X-ray did not demonstrate subdiaphragmatic free intra-abdominal air.
Emergency abdominal CT showed air in the hepatic portal veins (Fig. 1), focal dilatation of the small bowel with wall thickening, mesenteric fat stranding and peritoneal fluid collection, free air in the retroperitoneum, mainly to the right (retroperitoneum) (Fig. 2), air in the peritoneal cavity, mainly in the lower pelvic area, and free air in the pararectal space (Fig. 3). Air was also demonstrated in both inguinal canals mainly in the right and in both iliac-femoral veins (Fig. 4). Moreover, pleural effusion and atelectasis was found in both lower lobes of the lungs (Fig. 1).
Abdominal CT scan shows portal venous air in the left hepatic lobe, pleural effusion and atelectasis in both lower lobes. Abdominal CT scan depicts retropneumoperitoneum – mainly in the right space – in the lateral border of the psoas muscle and in the right preperitoneal compartment. Abdominal CT scan demonstrates: (i) pneumatosis intestinalis in rectum and free air in the pararectal space; (ii) pneumatosis intestinalis in sigmoid colon; and (iii) free air in lower pelvis in contact with the right inguinal canal. Abdominal CT scan demonstrates intravascular air in both femoral veins and air in both inguinal canals.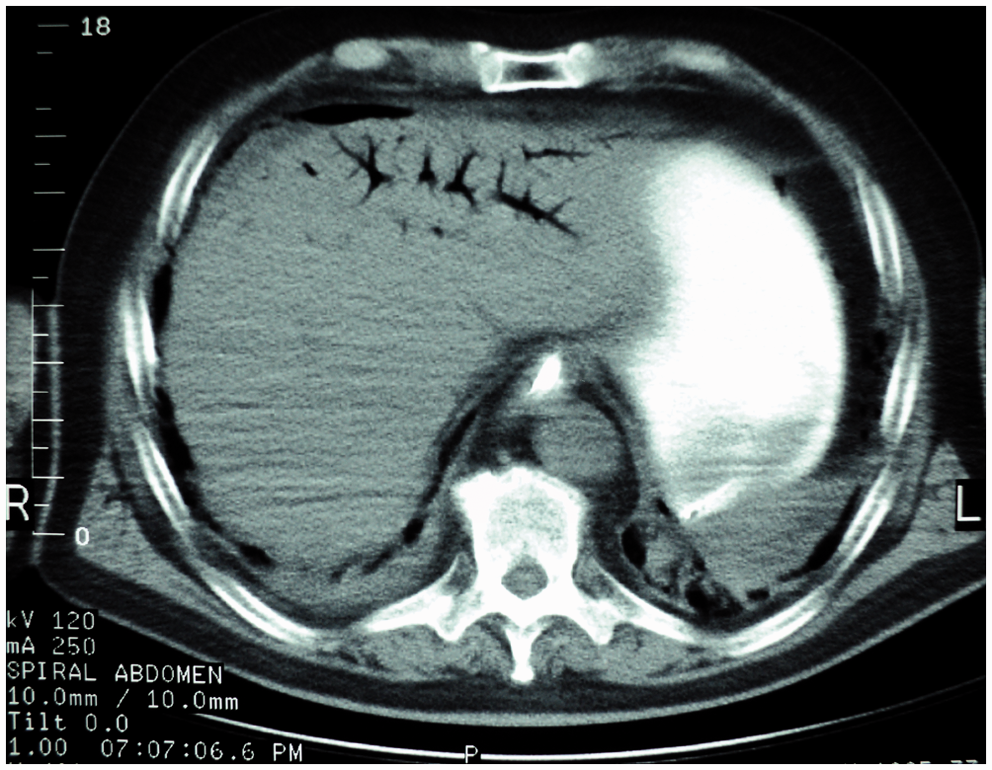



Laparotomy revealed extensive colon and small bowel necrosis distal to the jejunum. The affected region, ileum, and right colon up to the mid-transverse part, was resected, and an ileostomy and a transverse colostomy was made. The patient died after few hours in the intensive care unit from multiple organ failure.
Histology examination revealed transmural colonic and small bowel necrosis with evidence of active thromboembolic process and leucocytoclastic vasculitis.
Discussion
Acute bowel ischemia (ABI) is an often fatal disorder, with mortality between 59% and 100% (3,4).
Arterial embolism and thrombosis, non-occlusive ischemia, and mesenteric venous thrombosis are the most frequent causes of ABI (4,5). Chemotherapy agents may rarely cause ABI due to secondary vasculitis (6). Chemotherapy may also be related to thrombotic occlusion of the superior mesenteric artery (7). Hussein et al. reported a complication of Docetaxel leading to necrosis in the colon with histological findings revealing patchy bowel ischemia of varying degrees, associated with microvascular venous thrombosis within the bowel wall (8).
The key of definite treatment is early diagnosis of ABI and CT has an important role. The most common CT findings of this condition are: bowel wall thickening, pneumatosis intestinalis (PI), mesenteric or portal venous gas, mesenteric arterial or venous thromboembolism, and absence of bowel wall enhancement (9,10).
The CT findings of the patient in our case include a wide range of radiological findings suggesting miscellaneous abdominal pathology. Based on the CT findings of extensive PI mainly in the cecum-ascending colon and free air mainly in the right retroperitoneal space, history of chemotherapy and neutropenia, the initial diagnosis was acute ischemia-necrosis with perforation due to neutropenic colitis.
Four of the CT findings were associated with ABI and perforation (HPVG, PI, air in the branches of mesenteric veins, and the presence of free air in the peritoneal and in retroperitoneal space). Generally, gastrointestinal perforation is infrequent but with fatal toxicity related to chemotherapy (11,12).
The histologic findings did not confirm bowel perforation, but revealed necrosis of the gastrointestinal tract as a result of multiple thromboses in small mesenteric veins caused by chemotherapy.
The conclusion from these findings was that a neglected acute intestinal ischemia, could lead to extensive intestinal necrosis, with subsequent bowel perforation or transudation of air through the necrotic bowel wall.
However, to the best of our knowledge, there are few reports with free air in the peritoneal and retroperitoneal cavity without bowel perforation. Moreover, this is the first report of free air in the peritoneum and retroperitoneum due to excessive necrosis of intestinal segments and transudation of air through the necrotic wall.
The basic difficulty for the radiologists was to interpret the unusual CT findings as, the uncommon location of free air in the peritoneum, retroperitoneum, presence of air in the femoral veins and the inguinal canal in combination with the clinical and laboratory results.
The pneumoperitoneum in this patient appeared as free air in the peritoneal cavity mainly in the lower pelvic area, and not in the subdiaphragmatic space, which is the usual site of air after perforation. The reason for this was probably that there was no actual perforation, but transudation of free air from necrotic intestinal wall.
Therefore these findings suggest that free air in the peritoneal cavity can be present not only after intestinal perforation but also by transudation of air through the intestinal wall in cases of extensive necrotic bowel ischemia. Moreover, free air occurring by transudation in the peritoneum cavity may be entrapped in the mesenteric and mesosigmoid space and not appear, as usual, in the subdiaphragmatic space. The presence of retroperitoneal air should raise the suspicion of a perforated retroperitoneal viscus, which is a very rare condition (13).
The anterior pararenal space is the most common site of retroperitoneal gas. Air in the anterior pararenal space outlines the lateral border of the psoas muscle as in our patient.
CT has an important role in the assessment of retroperitoneal structures and can distinguish retroperitoneal from intraperitoneal air. Retroperitoneal air tends to be more fixed in its location although there may be some movement with changes in the patient’s position. Causes of retroperitoneal air except from bowel perforation due to intestinal ischemia, are inflammatory processes, blunt or penetrating trauma, iatrogenic manipulation, gas-producing organisms, and retroperitoneal gas gangrene (14,15).
The presence of air in the inguinal canal can be explained anatomically by the communication between the lower parts of the pelvic areas and the inguinal canal.
Thus, in cases of perforation or air transudation through the necrotic wall of the sigmoid colon, entrapped in the mesosigmoid space can move towards inguinal canal. Air in the inguinal canals can be due to colon cancer or perforated bowel diverticulum (16).
Air bubbles in the soft tissues may represent gas produced by anaerobic bacteria. CT is useful for the evaluation of patients with sepsis without a known source (17,18).
Intravascular gas in femoral or iliac veins is a very rare condition with very few reports in the literature. It may occur as a complication of femoral osteomyelitis, following removal of a jugular vein catheter, as an incidental finding after blunt abdominal trauma, as a complication of emphysematous cystitis, and as decompression illness (19,20).
Based on laboratory tests and the other symptoms in this patient, the presence of air in both femoral and iliac veins can be explained by septicemia. However, due to the fast deterioration of the patient it was not possible to confirm bacteremia by detecting anaerobic bacteria in the blood stream.
In conclusion, CT examination of the abdomen plays an important role in the diagnosis of acute intestinal ischemia, even in rare cases of vasculitis related with chemotherapy.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.