
Abstract
Abstract
Eagle's syndrome is a rare entity, which is not commonly suspected in clinical practice. The occurrence of similar signs in diseases other than Eagle's syndrome may make a precise diagnosis difficult and time-consuming for many clinicians. Radiological examinations are useful to make the accurate diagnosis. Three-dimensional volume-rendering CT scan is the most valuable diagnostic tool.
Eagle's syndrome, also known as elongated styloid process, is an entity that may be the source of craniofacial and cervical pain and is due to an elongated styloid process (1). Its diagnosis may be difficult because of similarities with other disorders but can be confirmed by clinical and radiological examinations.
Case report
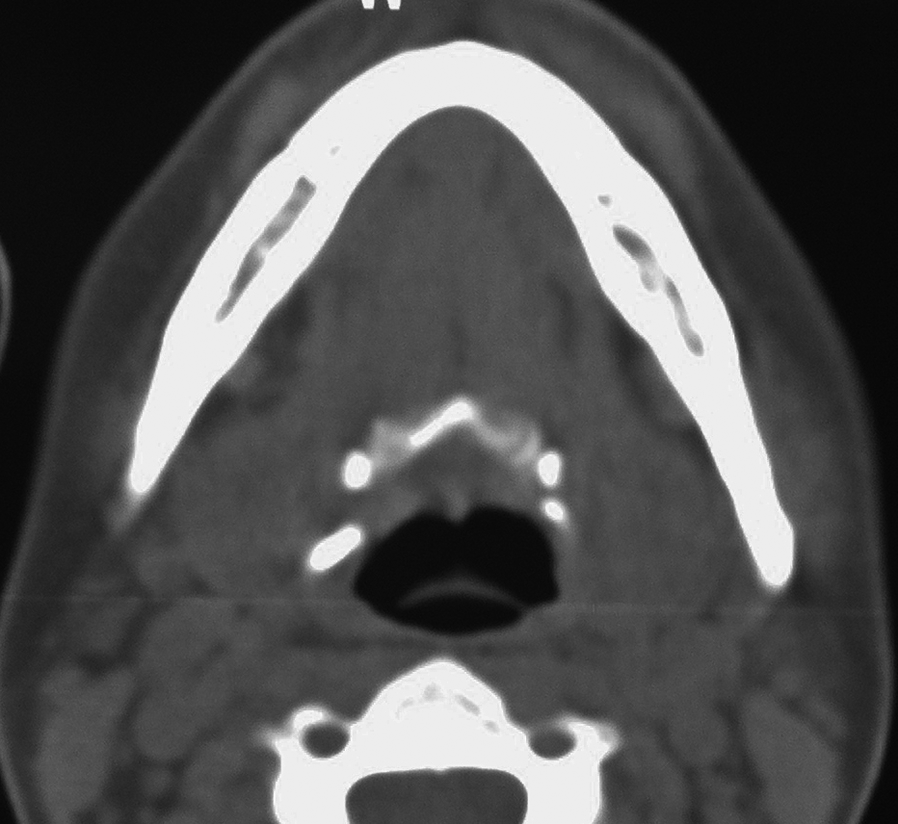
A 30-year-old woman presented with a 4-month history of right submandibular pain and swelling, as well as sore throat prominent on the right side of the pharynx, and difficulty in swallowing solid foods. On clinical examination she had referred pain on bilateral palpation of the oropharynx. Cervical ultrasonographic evaluation was unremarkable. Eagle's syndrome was suspected. A cervical lateral radiograph showed an elongated styloid process (Fig. 1). Computed tomography (CT) with axial (Fig. 2), coronal (Fig. 3), and three-dimensional (3D) volume-rendering CT images (Fig. 4) showed complete ossification of the stylohyoid ligaments with pseudoarticulations. A lateral neck radiograph showed calcifications from the base of the skull to the hyoid bone. An external approach for the removal of the styloid processes was planned and resulted in complete relief of the patient's symptoms.
Lateral view plain radiograph of the cervical spine shows a large ossified structure extending from the base of the skull anterolaterally and caudally to the hyoid bone Axial CT image showing a bilateral neck calcification extending from the base of the skull to the hyoid bone Coronal CT image shows ossification of the stylohyoid ligaments with pseudoarticulations 3D volume-rendering reconstruction of a computed tomogram shows ossification of the stylohyoid ligaments from the base of the skull to the lesser cornu of the hyoid bone


Discussion
The styloid process is an elongated conical projection of the temporal bone that lies anteriorly to the mastoid process, between the internal and external carotid arteries. It forms with the stylohyoid ligament and the small horn of the hyoid bone the stylohyoid apparatus which is derived from the cartilage of Reichert of the second brachial arch (2). Three muscles originate from the styloid process: the styloglossal, stylohyoid, and stylopharyngeous. The styloid and the stylomandibular ligaments are also attached to the styloid process (3).
The normal length of the styloid process is individually variable. Eagle reported that the average length of the styloid process was 2.5 cm, and any process >2.5 cm might be considered to be elongated (3). Bilateral elongation of the styloid process is quite common (4). However, bilateral symptoms are less frequent. Partial ossification of the stylohyoid ligament is not uncommon but complete ossification, as in our case report, is rare (5). The pathogenesis of elongation of the styloid process and ossification of the stylohyoid ligament is still under discussion and the main hypotheses rely on heredity, embryology, metaplasia, trauma, and degenerative transformation (6, 7). In 1937, the symptom complex associated with elongation of the styloid process or ossification of the stylohyoid ligament was first described by Eagle and called Eagle's syndrome.
The incidence of elongated styloid process has been reported in 4% of the general population, but of these, only about 4% present with symptoms that are attributable to elongation (4, 8). Patients are usually aged >30 years (3). A wide variety of symptoms have been attributed to elongation of the styloid process, including no specific cervical pain, throat pain, earache, odynophagia, foreign body sensation in the throat, and cerebrovascular symptoms induced by positional change (6, 9–11). These symptoms are non-specific and can be confused with a wide variety of disorders such as aerodigestive tract malignancies, neuralgia, temporomandibular joint dysfunction, dental malocclusion, and hyoid bursitis (1). These conditions have to be excluded before considering Eagle's syndrome. The tip of the styloid process can be palpable in the tonsillar fossa as a hard bony spicule that aggravates symptoms with local tenderness (6). The exact factor for the onset of this syndrome is still unknown and its etiology has not yet been fully understood.
The lateral neck views can be sufficient in some cases to diagnose an elongated styloid process (12). Modified Towne's view and an ortho-pantomogram can also confirm the diagnosis with the advantage that the entire length of the process can be seen very distinctly and its deviation can so be made out clearly (13). However, superimpositions of anatomical structures cause frequently difficulties in viewing the styloid process (14). 3D CT scan is the most valuable diagnostic tool because of its ability to facilitate accurate measurement of the length of the styloid process (15–17). Moreover, it can define its angulation, and anatomic relationship (18).
In the majority of the cases, surgical shortening of the elongated processes, using intra-oral or extra-oral approaches, is the effective method to provide relief of the troublesome symptoms (5). The intra-oral approach has some advantages such as simplicity of the technique, reduced operating time, absence of visible scars, and minor risks of operative complications (9, 19). Several alternative non-surgical treatment methods, such as transpharyngeal infiltration of steroids or anesthetics in the tonsillar fossa have been suggested but have turned out to be non-effective (3, 8). Infiltration of steroids or local anesthetics can be used a proof therapy to see if a patient's complaints are related to an elongated styloid process, especially when symptoms persist after surgery.
In conclusion, when dealing with cases of cervical pain, Eagle's syndrome must be taken in account. Plain radiographs can be helpful. CT scan is required to confirm diagnosis.