
Abstract
Meningioma rarely gives rise to metastases outside the brain and meninges. We report here a case of a patient who was treated for anaplastic brain meningioma with surgery and fractionated radiation therapy without any recurrence until 5 years after the operation, when she developed vertebral metastases.
Meningiomas are neoplasms of the central nervous system derived from meningothelial cells. These neoplasms account for 14–19% of intracranial tumors (1). Most meningiomas are benign and surgery is curative in the majority of cases. However, malignant meningiomas are more aggressive (with 5-year survival rates in the range of 50–60% versus 90–100% in benign meningiomas), tend to recur earlier, and invade the surrounding structures of the scull and the brain (with interval to recurrence estimated at 3.5 years versus 7.5 years in benign meningiomas) (2). Despite their malignancy, extracranial metastases of malignant meningiomas are rare with an estimated incidence of 1–5 out of 1000 cases (2). Only 7% involve vertebrae and just a few cases have been reported in the literature (3). We present here an unusual case of a patient who was treated for an anaplastic brain meningioma originally diagnosed in 2007 and treated by complete surgical resections and radiotherapy, with complete recovery for 5 years, after which she developed vertebral metastases.
Case report
The report involves a 51-year-old woman who presented in 2007 with a clinical history of headache, nausea, and vomiting. The initial cranial computed tomography (CT) and magnetic resonance imaging (MRI) showed a left parieto-temporal dural-based infiltrating tumor. The mass was mushrooming on the outer edge and had a heterogenous enhancement (Fig. 1a and b) with necrosis, central calcifications, marked edema (Fig. 1c), and bone destruction.
MRI: left parieto-temporal dural-based infiltrating tumor. The mass had an heterogenous enhancement (a, b) with necrosis, and marked edema (c).
The patient underwent a complete surgical resection. Histological diagnosis revealed an anaplastic meningioma (World Health Organization [WHO] grade III) with hypercellularity and a prominent mitotic activity with around 32 mitoses per 10 high power fields (hpf) (Fig. 2a and b). The postoperative course was uneventful and the patient was discharged. The operation was followed by fractionated radiation therapy. At the follow-up during the next 4 years, the patient presented in good condition and MRI showed no tumor recurrence. In March 2012, the patient developed a progressively invalidating lumbar pain. Spinal MRI showed a slightly circumscribed mass within the right transverse process of the third thoracic vertebra (T3) with paravertebral extension to surrounding soft tissue (Fig. 3). Brain MRI showed no recurrence of the intracranial meningioma (Fig. 4).
Histological diagnosis (hematoxylin and eosin HE x 200) anaplastic meningioma with hypercellularity and a prominent mitotic activity with around 32 mitoses per 10 hpf (a). Tumor cells display strong immunoreactivity for CD 99 (b). Spinal MRI: circumscribed mass within the right transverse process of the third thoracic vertebra (T3) with paravertebral extension to the soft tissues. Brain MRI: no recurrence of the intracranial meningioma.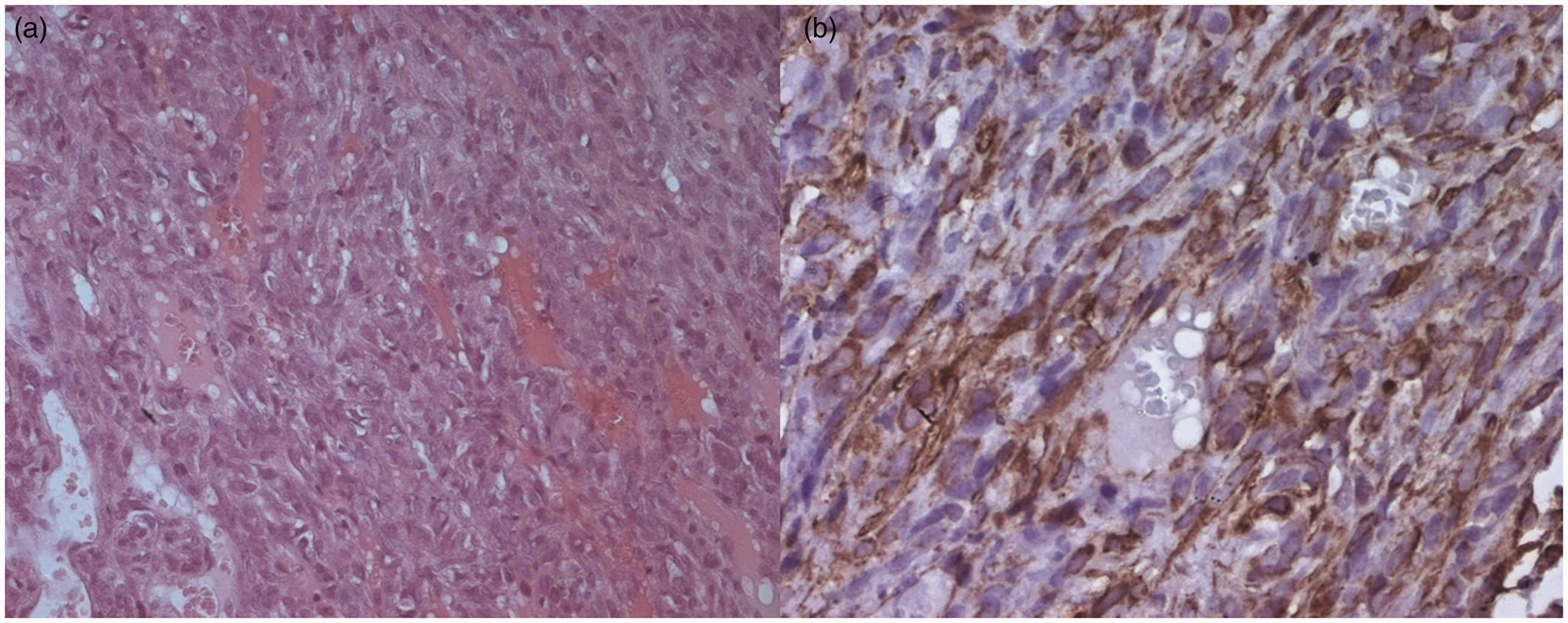


A percutaneous transpedicular biopsy was performed and the histological findings were identical to those found in 2007 (Fig. 5a and b). The patient was given palliative radiotherapy for bone metastases but she died 3 months later due to pulmonary embolism.
The CT-guided biopsy of the vertebral mass revealed a metastasis of a meningioma: hypercellularity with prominent mitotic activity (hematoxylin and eosin HE x 100) with area of necrosis.
Discussion
Summary of the 2007 WHO grading scheme for meningiomas (4).

Extracranial metastases of meningiomas are rare. The most common sites of metastases of meningiomas are the lungs (60%) (12), followed by the abdomen and liver (34%), cervical lymph nodes (18%), long bones, pelvis and skull (11%), pleura (9%), central nervous system (7%), and mediastinum (5%). The kidneys, bladder, thyroid, breasts, thymus, heart, skin, vulva, adrenal glands, and eyes are only occasionally affected (13, 14). Only 7% occur in the vertebrae. A few cases of spinal metastases have been published to date. Some of them were intra-arachnoidian and others were intraosseous; located in C-2 (15), T-1 (16), T-10 (17), T-11 (8), L-2 (17), L-5 (18), and sacrum (19). They can even be multiple. Distant metastases from benign meningiomas are extremely rare (1,20). However, the rate of distant metastases could reach 5% for atypical and 30% for anaplastic or malignant meningiomas (1,2,11). The mechanism of systemic spread is not yet known, but a passage of tumor through venous sinuses and channel is discussed in the literature (8,11,17). Surgical removal may also increase the risk of iatrogenic metastases of meningiomas with atypical histology, and malignant meningiomas could even disseminate without previous surgery (21,22). An intracranial lesion usually recurs locally several times before it metastasizes. This interval appears to be shorter for atypical and malignant tumors (about 1 year) compared to benign lesions (>5 years). The explanation for this variety remains unclear. There is quite a variable latency period between the diagnosis of the intracranial tumor and the appearance of the metastasis, ranging from a few months to >20 years (8). In our case, there were 5 years between the tumor resection and the vertebral metastasis.
Our case report is unusual because the patient developed distance metastases without intracranial recurrence of the meningioma. Factors that suggest the ability to metastasize include previous intracranial surgery and especially malignant histological grading.
Currently, to our knowledge, no consensus guidelines exist for treatment of metastasizing meningiomas (23). Treatment options available for metastatic disease of the spine include medical therapy, surgery, and radiation. Operative intervention is most often palliative with pain control, maintenance of neurologic function, and spinal stability as primary goals. For years, many considered that surgery is the best initial therapy, with the goal of gross total resection. Realistically, such an aggressive approach requires en bloc resection: it is rarely indicated in vertebral metastases, but can be considered for single lesions with a good prognosis (8,24,25). There is no proven effective chemotherapy agent for treating metastasizing meningiomas. In some studies irinotecan and hydroxyurea have had a marginal response. Progress in identifying alternative forms of therapy for patients with these metastases has been limited by poor understanding of the molecular pathogenesis of meningiomas and of the critical molecular changes driving tumor growth, as well as by the lack of meningioma cell lines and tumor models for preclinical studies (26). Extracranial bone metastases and multiple extracranial metastases of meningiomas predict poor prognosis (2).
In conclusion, although uncommon, vertebral metastases of meningiomas should always be included in the differential diagnosis in patients with a history of meningioma who developed lesions suggestive of distant metastases, especially patients who had malignant intracranial meningioma.